Folate for Cardiovascular Health & Stroke Prevention
The story of folate and cardiovascular disease is more complicated than its story for neural tube defects. The "homocysteine hypothesis" — that elevated homocysteine causes atherosclerosis and that lowering it should reduce cardiovascular events — was tested in a series of large randomized trials in the 2000s (NORVIT, HOPE-2, SEARCH, WAFACS). All successfully lowered homocysteine, but none reduced primary cardiovascular event rates in unselected secondary-prevention populations. Stroke, however, was a different story. The 20,702-patient China Stroke Primary Prevention Trial (CSPPT) showed a 21% first-stroke reduction with folate. The Wang Lancet 2007 meta-analysis showed a similar ~18% stroke reduction. The pattern: folate lowers stroke risk in populations with low baseline folate, no fortification, and elevated homocysteine — not so much in well-supplemented Western populations. This page walks through each pivotal trial and synthesizes the modern integrative-medicine recommendation.
Table of Contents
- The Homocysteine Hypothesis
- How Folate Lowers Homocysteine
- NORVIT (2006)
- HOPE-2 (2006)
- SEARCH (2010)
- WAFACS & Other Negative Trials
- The Stroke Signal Persists
- CSPPT — The Definitive Stroke Trial
- Wang Lancet 2007 Stroke Meta-Analysis
- Folate, Nitric Oxide & Endothelial Function
- Who Benefits Most from Folate for CV/Stroke Prevention
- Practical Protocol
- Cautions
- Key Research Papers
- Connections
- Featured Videos
The Homocysteine Hypothesis
In 1969 the pediatric pathologist Kilmer McCully made an observation that would launch a 50-year research program: children with the rare genetic disease homocystinuria — who carry markedly elevated homocysteine levels from birth — develop severe, premature atherosclerosis and die from cardiovascular events in their teens and twenties. The arterial lesions found at autopsy were morphologically identical to ordinary adult atherosclerosis, just compressed into two decades instead of seven.
McCully proposed the "homocysteine hypothesis": that homocysteine itself is an arterial toxin, and that the milder elevations seen in adults (from nutritional folate, B12, or B6 deficiency, or from MTHFR polymorphisms) might contribute to ordinary adult atherosclerosis. If true, the corollary would be that nutritional intervention to lower homocysteine should reduce cardiovascular events — a remarkably cheap and accessible approach to cardiovascular prevention.
By the 1990s, observational epidemiology consistently supported the hypothesis: elevated homocysteine was associated with increased cardiovascular events in dozens of cohort studies. Each 5 μmol/L increment in homocysteine was associated with roughly 30% higher coronary heart disease risk. The biochemistry made sense — homocysteine impairs endothelial function, promotes oxidative stress, increases thrombogenicity, damages collagen cross-linking, and accelerates atherosclerotic plaque formation. The next logical step was to test the intervention: would lowering homocysteine through folate, B12, and B6 supplementation reduce cardiovascular events in randomized trials?
The answer, as it turned out, was complicated.
How Folate Lowers Homocysteine
Homocysteine is metabolized via three pathways:
- Folate-B12-dependent remethylation — 5-MTHF donates a methyl group to homocysteine, regenerating methionine. Methionine synthase enzyme; B12 cofactor; folate as methyl source. The primary pathway in most tissues.
- Betaine-BHMT remethylation — betaine (TMG) donates a methyl group to homocysteine via betaine-homocysteine methyltransferase. Operates primarily in liver; useful alternative when folate or B12 is limited.
- B6-dependent transsulfuration — homocysteine is condensed with serine by cystathionine β-synthase (CBS) to form cystathionine, which is then cleaved to cysteine. B6 cofactor at both steps. This is the only true clearance pathway — the others regenerate methionine for reuse.
Folate supplementation lowers homocysteine because the folate-B12 remethylation pathway is the highest-flux clearance pathway in most people. Even modest folate supplementation (400-800 mcg/day) typically lowers homocysteine 1-3 μmol/L, with the magnitude depending on baseline status. The Homocysteine Lowering Trialists' Collaboration meta-analysis (2005) found that 800 mcg/day folic acid lowered homocysteine by ~25% on average across 25 trials. MTHFR variants amplify the response — TT homozygotes with elevated baseline homocysteine see the largest drops.
The biochemistry left no doubt: folate lowers homocysteine reliably and substantially. The question became: does that translate into clinical event reduction?
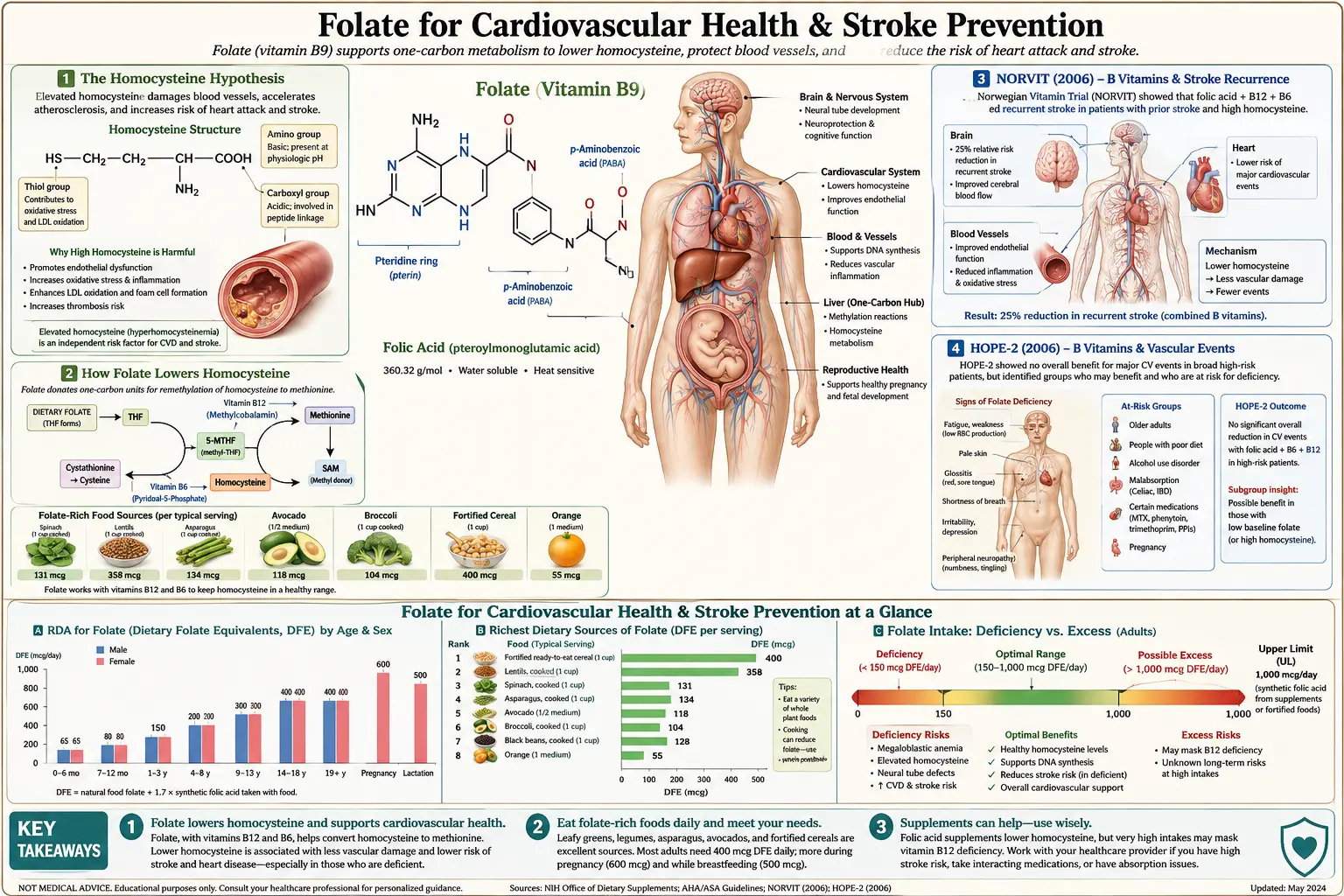
NORVIT (2006)
The Norwegian Vitamin Trial (NORVIT), published by Bonaa et al. in the New England Journal of Medicine in 2006, randomized 3,749 patients with recent acute myocardial infarction to four arms: folic acid 800 mcg + B12 400 mcg + B6 40 mg, folic acid + B12 only, B6 only, or placebo. Follow-up was 3.5 years. The primary outcome was a composite of recurrent MI, stroke, and sudden death.
Results:
- Homocysteine reduced 27% in the folic acid + B12 + B6 arm
- No significant reduction in the primary cardiovascular composite endpoint
- A trend toward harm in the folic acid + B12 + B6 group (RR 1.22, 95% CI 1.00-1.50, P=0.05)
- Investigators speculated that high-dose folic acid might accelerate restenosis after coronary intervention
NORVIT was the first major negative cardiovascular trial of homocysteine-lowering therapy. The trend toward harm was particularly troubling and contradicted the strong observational evidence.
HOPE-2 (2006)
The Heart Outcomes Prevention Evaluation 2 trial (Lonn et al., NEJM 2006) randomized 5,522 patients with vascular disease or diabetes to folic acid 2.5 mg + B12 1 mg + B6 50 mg or placebo. Follow-up 5 years. Primary outcome: composite of cardiovascular death, MI, and stroke.
Results:
- Homocysteine reduced 22% in the vitamin group
- No significant reduction in the primary composite endpoint (RR 0.95, 95% CI 0.84-1.07)
- However: statistically significant 25% reduction in stroke (RR 0.75, 95% CI 0.59-0.97)
- Modest increase in unstable angina hospitalizations in the vitamin group (counterbalanced the stroke benefit in the composite)
HOPE-2 was the first hint that stroke might behave differently than overall cardiovascular events. The 25% stroke reduction was statistically significant and clinically meaningful, but was lost in the composite primary endpoint because it was offset by changes in other components.
SEARCH (2010)
The Study of the Effectiveness of Additional Reductions in Cholesterol and Homocysteine (SEARCH), published by Armitage et al. in JAMA in 2010, was the largest single homocysteine-lowering trial: 12,064 post-MI patients in the UK randomized 2×2 factorial to folic acid 2 mg + B12 1 mg versus placebo, and to high-dose simvastatin versus standard dose. Follow-up 6.7 years.
Results for the folic acid + B12 arm:
- Homocysteine reduced 28%
- No significant reduction in major vascular events (RR 1.04, 95% CI 0.97-1.12)
- No reduction in stroke specifically (RR 0.99)
- No significant increase in cancer overall (a concern raised in earlier studies)
SEARCH was a large, long, well-conducted trial with a definitive negative result. Combined with NORVIT and HOPE-2, the conclusion for secondary cardiovascular prevention seemed clear: homocysteine-lowering with B vitamins does not reduce major cardiovascular events in patients with established disease, despite reliably lowering homocysteine.
WAFACS & Other Negative Trials
Additional trials reinforced the negative pattern for secondary prevention:
- WAFACS (Albert 2008, JAMA) — Women's Antioxidant and Folic Acid Cardiovascular Study. 5,442 women with prior CVD or risk factors. Folic acid 2.5 mg + B12 1 mg + B6 50 mg vs placebo. 7.3 year follow-up. No reduction in cardiovascular events.
- VITATOPS (2010, Lancet Neurology) — 8,164 patients with prior stroke or TIA. Folic acid 2 mg + B12 0.5 mg + B6 25 mg vs placebo. 3.4 year follow-up. No significant reduction in recurrent stroke (RR 0.92, P=0.10) — despite stroke being the primary endpoint and the trial being designed to detect a stroke benefit.
- VISP (Toole 2004, JAMA) — 3,680 patients with recent nondisabling stroke. High-dose B vitamins vs low-dose. No reduction in recurrent stroke, ischemic heart events, or death over 2 years.
- WENBIT (2008) — Western Norway B Vitamin Intervention Trial. 3,090 patients undergoing coronary angiography. Folic acid + B12 +/- B6 vs placebo. No reduction in cardiovascular events.
The cumulative evidence for secondary cardiovascular prevention in well-nourished Western populations was essentially negative. The homocysteine hypothesis appeared to have failed as a basis for clinical intervention in patients with existing disease.
The Stroke Signal Persists
While the cardiovascular composite endpoints were stubbornly negative, a stroke-specific signal kept reappearing across trials and meta-analyses:
- HOPE-2: 25% stroke reduction (statistically significant)
- SEARCH: no stroke effect (but well-fortified UK population)
- VITATOPS: trend toward stroke reduction (not significant in the primary analysis but significant in some pre-specified subgroups)
- Multiple meta-analyses: ~10-25% stroke reduction signal across pooled trials
Several possible explanations:
- Stroke is more sensitive to homocysteine than coronary events — homocysteine's adverse effects on small-vessel endothelium and on hypertension may matter more for stroke than for coronary atherosclerosis
- Folate independently lowers blood pressure in some studies (especially in MTHFR variant carriers), which would specifically reduce stroke risk
- Folate's effects on cerebral white matter — the VITACOG cognitive trial found 30% reduction in brain atrophy in high-homocysteine elderly, suggesting folate protects vulnerable small-vessel territory
- Trial populations — most secondary-prevention trials were conducted in fortified countries (US, Canada, UK) with already-adequate folate status, limiting the room for additional benefit
This led researchers to design a primary prevention trial in an unfortified population with high baseline homocysteine: the China Stroke Primary Prevention Trial.
CSPPT — The Definitive Stroke Trial
The China Stroke Primary Prevention Trial (CSPPT), published by Huo et al. in JAMA in 2015, addressed the limitations of prior trials by selecting an ideal population: 20,702 hypertensive adults in China — a country without mandatory folic acid fortification, with high baseline homocysteine, high stroke incidence, and a substantial MTHFR C677T TT genotype prevalence.
Design
- 20,702 adults with hypertension, no history of MI or stroke
- Randomized to enalapril 10 mg + folic acid 0.8 mg daily vs enalapril 10 mg alone
- Median follow-up: 4.5 years
- Primary outcome: first stroke (ischemic or hemorrhagic)
Results
- First stroke reduced 21% with folic acid + enalapril vs enalapril alone (2.7% vs 3.4%, HR 0.79, 95% CI 0.68-0.93, P=0.003)
- Ischemic stroke reduced 24% (HR 0.76, 95% CI 0.64-0.91)
- No significant effect on hemorrhagic stroke
- Composite cardiovascular events reduced 20% (HR 0.80, 95% CI 0.69-0.92)
- Benefit was largest in MTHFR TT genotype carriers with low baseline folate — reflecting the population for whom folate was most needed
- No significant cancer or other safety signals
CSPPT was the largest and most definitive trial to demonstrate that folic acid supplementation prevents first stroke. The trial was widely interpreted as validating the homocysteine hypothesis specifically for stroke and specifically for unfortified populations with elevated baseline homocysteine.
Subsequent CSPPT subgroup analyses showed the benefit was concentrated in:
- MTHFR TT homozygotes (the genetic group with highest baseline homocysteine)
- Subjects with low baseline serum folate (<5.7 ng/mL)
- Subjects with platelet count >210,000 (suggesting a thrombogenic mechanism)
The clinical implication: folate is most effective for stroke prevention in those who need it most — not in already-fortified, well-nourished, low-homocysteine populations.
Wang Lancet 2007 Stroke Meta-Analysis
Wang et al. (Lancet 2007) pooled 8 trials totaling 16,841 subjects to specifically test the folate-stroke relationship. The result: an 18% reduction in stroke risk with folic acid supplementation (RR 0.82, 95% CI 0.68-1.00, P=0.045), with the effect concentrated in:
- Trials with longer duration (>36 months)
- Trials with greater homocysteine lowering (>20%)
- Trials in populations without mandatory folic acid fortification (consistent with CSPPT's subsequent finding)
The Wang meta-analysis was the first pooled-data confirmation of the stroke-specific benefit that individual trials had hinted at. Subsequent meta-analyses have replicated this finding with broadly consistent effect sizes (10-25% stroke reduction).
Folate, Nitric Oxide & Endothelial Function
Beyond the homocysteine-lowering effect, folate (specifically 5-MTHF) has direct, homocysteine-independent effects on the vascular endothelium that may contribute to its stroke and cardiovascular benefits:
- 5-MTHF enhances endothelial nitric oxide synthase (eNOS) activity — the enzyme that produces nitric oxide, the master vasodilator and antiatherogenic signaling molecule. Antoniades et al. (Circulation 2009) showed that intravenous 5-MTHF immediately improved endothelial function in coronary artery disease patients, faster than any homocysteine effect could explain.
- 5-MTHF stabilizes tetrahydrobiopterin (BH4) — the essential cofactor for eNOS. When BH4 is oxidized to dihydrobiopterin (BH2), eNOS becomes "uncoupled" and produces superoxide instead of nitric oxide. 5-MTHF prevents BH4 oxidation, keeping eNOS coupled and producing protective nitric oxide rather than damaging superoxide.
- Direct antioxidant effects — 5-MTHF scavenges superoxide directly, reducing vascular oxidative stress.
- Anti-thrombotic effects — observational data suggest folate reduces platelet activation; the CSPPT platelet subgroup finding is consistent with this.
- Blood pressure reduction — particularly in MTHFR TT carriers; the McNulty group at Ulster has shown 5-10 mmHg reductions with riboflavin in hypertensive TT carriers (likely an MTHFR-stabilization effect that increases endogenous 5-MTHF and indirectly improves eNOS coupling).
The implication: methylfolate specifically (not synthetic folic acid) may provide cardiovascular benefits through eNOS-coupling and direct endothelial mechanisms beyond the homocysteine-lowering effect. This may partially explain why trials using methylfolate could show larger effects than the original folic acid trials, and supports the modern integrative-cardiology preference for 5-MTHF in homocysteine and endothelial-function-focused protocols.
Who Benefits Most from Folate for CV/Stroke Prevention
Synthesizing the CSPPT findings, the Wang meta-analysis subgroup data, and the broader trial literature, the populations most likely to benefit from folate supplementation for cardiovascular/stroke prevention are:
- Low baseline folate status — serum folate <5-7 ng/mL or RBC folate <400 ng/mL. Includes people avoiding fortified grains, with malabsorption, on anticonvulsants or methotrexate, or with chronic alcohol use.
- Elevated baseline homocysteine — >10 μmol/L. The integrated functional marker of inadequate methylation; identifies the people for whom folate-B12-B6 supplementation will both lower homocysteine and likely reduce stroke risk.
- MTHFR C677T TT homozygotes (and compound heterozygotes) — the genetic group with highest baseline homocysteine and the largest measured benefit in CSPPT subgroup analysis. Should preferentially use methylfolate to bypass the variant enzyme.
- Populations without grain fortification — many European countries, parts of Asia, much of Africa, and increasingly the segments of US/Canadian populations that avoid refined grains (paleo, keto, gluten-free).
- Hypertensive adults — CSPPT demonstrated benefit specifically in this group; folate is a defensible adjunct to standard antihypertensive therapy for stroke risk reduction.
- Cognitive impairment with elevated homocysteine — the VITACOG trial showed 30% reduction in brain atrophy in MCI patients with homocysteine >11 μmol/L.
- The elderly with marginal folate, B12, or B6 status — reduced absorption, marginal intake, and increased homocysteine all argue for screening and supplementation.
Populations least likely to benefit:
- Already well-nourished, fortified-grain-consuming Western adults with baseline homocysteine <8 μmol/L and normal MTHFR — the SEARCH and HOPE-2 populations.
- Established cardiovascular disease patients with normal homocysteine and adequate baseline folate — the secondary-prevention setting where most negative trials were conducted.
Practical Protocol
For high-risk cardiovascular/stroke prevention (per CSPPT-style indication)
- Test first: Serum or RBC folate, homocysteine, serum B12 + MMA, MTHFR genotype (one-time test). See Homocysteine for details.
- If homocysteine >10 μmol/L and/or MTHFR TT genotype:
- Methylfolate 800 mcg - 5 mg daily (start lower, titrate up based on homocysteine response)
- Methylcobalamin (B12) 1,000 mcg daily
- P5P (B6) 25-50 mg daily
- Riboflavin (B2) 25 mg daily — especially for MTHFR TT carriers
- Trimethylglycine (TMG/betaine) 1-3 g daily as adjunct if homocysteine remains elevated
- Recheck homocysteine at 8-12 weeks; titrate to homocysteine <8 μmol/L
- If homocysteine <8 μmol/L: Basic methylated B-complex (400 mcg methylfolate, 500 mcg methylcobalamin, 25 mg P5P, 25 mg riboflavin) is sufficient maintenance.
Companion cardiovascular protocols
- Omega-3 (DHA + EPA): 1-2 g combined daily — required for the B-vitamin brain atrophy effect (Jerneren 2015)
- Magnesium glycinate: 200-400 mg elemental daily — blood pressure and vascular function
- Vitamin D3 + K2: 2,000-5,000 IU D3 + 100-200 mcg K2-MK7 — vascular calcium handling
- CoQ10 ubiquinol: 100-200 mg daily, especially if on statins — mitochondrial cardiac support
- Aged garlic extract: 600-1,200 mg daily — modest BP reduction and anti-atherosclerotic effects
Cautions
- B12 deficiency masking — the universal folate caution. Always assess B12 status (serum B12, MMA) before initiating high-dose folate, and always co-supplement methylcobalamin. The risk is amplified in older adults, vegans, metformin users, and PPI users.
- NORVIT trend toward harm — the NORVIT post-MI trend toward harm in the folic acid + B12 + B6 group has not been replicated in other trials but warrants caution in the immediate post-MI period (first 6 months). Hold off on initiating high-dose B vitamins until cardiac status is stabilized.
- Restenosis hypothesis — some early data suggested high-dose folic acid might accelerate in-stent restenosis. Subsequent trials have not confirmed this concern. Methylfolate appears not to share this concern, but coordination with cardiology after recent PCI is prudent.
- Anticoagulant interactions — folate and B vitamins do not directly interact with warfarin or DOACs in clinically meaningful ways, but coordination with the anticoagulant clinic for INR monitoring is standard practice.
- Hypertension medication interactions — folate is safe with all standard antihypertensive classes including ACE inhibitors (CSPPT specifically combined folate with enalapril). May produce additive BP-lowering effect — monitor.
- Cancer history — very high-dose synthetic folic acid (5 mg+ daily for years) has been weakly associated with progression of pre-existing precancerous colorectal lesions. Use methylfolate rather than folic acid at high doses, and discuss with oncology if there is an active cancer history.
- Avoid synthetic folic acid above 1 mg/day chronically — the unmetabolized folic acid concern, the dual-effect cancer hypothesis, and the autism U-shape signal all favor using 5-MTHF when therapeutic doses are needed.
Key Research Papers
- Bonaa KH et al. (2006). Homocysteine lowering and cardiovascular events after acute myocardial infarction (NORVIT). N Engl J Med. — PubMed
- Lonn E et al. (2006). Homocysteine lowering with folic acid and B vitamins in vascular disease (HOPE-2). N Engl J Med. — PubMed
- Armitage JM et al. (2010). Effects of homocysteine-lowering with folic acid plus vitamin B12 vs placebo on mortality and major morbidity in myocardial infarction survivors (SEARCH). JAMA. — PubMed
- Huo Y et al. (2015). Efficacy of folic acid therapy in primary prevention of stroke among adults with hypertension in China: the CSPPT randomized clinical trial. JAMA. — PubMed
- Wang X et al. (2007). Efficacy of folic acid supplementation in stroke prevention: a meta-analysis. Lancet. — PubMed
- Toole JF et al. (2004). Lowering homocysteine in patients with ischemic stroke to prevent recurrent stroke, myocardial infarction, and death (VISP). JAMA. — PubMed
- VITATOPS Trial Study Group (2010). B vitamins in patients with recent transient ischaemic attack or stroke (VITATOPS). Lancet Neurol. — PubMed
- Albert CM et al. (2008). Effect of folic acid and B vitamins on risk of cardiovascular events and total mortality among women at high risk for cardiovascular disease (WAFACS). JAMA. — PubMed
- Antoniades C et al. (2009). 5-Methyltetrahydrofolate rapidly improves endothelial function and decreases superoxide production in human vessels. Circulation. — PubMed
- Yang Q et al. (2006). Improvement in stroke mortality in Canada and the United States, 1990 to 2002 (fortification effect). Circulation. — PubMed
- Homocysteine Lowering Trialists' Collaboration (2005). Dose-dependent effects of folic acid on blood concentrations of homocysteine: a meta-analysis. Am J Clin Nutr. — PubMed
- Wilson CP et al. (2012). Riboflavin offers a targeted strategy for managing hypertension in patients with the MTHFR 677TT genotype. Am J Clin Nutr. — PubMed
PubMed Topic Searches
- PubMed: folate homocysteine cardiovascular disease
- PubMed: folic acid stroke prevention trial
- PubMed: homocysteine endothelial dysfunction
- PubMed: MTHFR C677T cardiovascular
- PubMed: 5-MTHF endothelial nitric oxide eNOS
- PubMed: folate blood pressure hypertension
Connections
- Vitamin B9 Overview
- B9 Benefits Hub
- B9 Pregnancy & Neural Tube
- B9 Methylation & Homocysteine
- B9 Depression & Mental Health
- Vitamin B12
- Vitamin B6
- Vitamin B2 (Riboflavin)
- Choline
- Methionine
- Homocysteine
- Lipid Panel
- Cardiology
- Stroke
- Hypertension
- Alzheimer's Disease
- Oxidative Stress
- All Vitamins