Phosphorus — Benefits Deep Dive
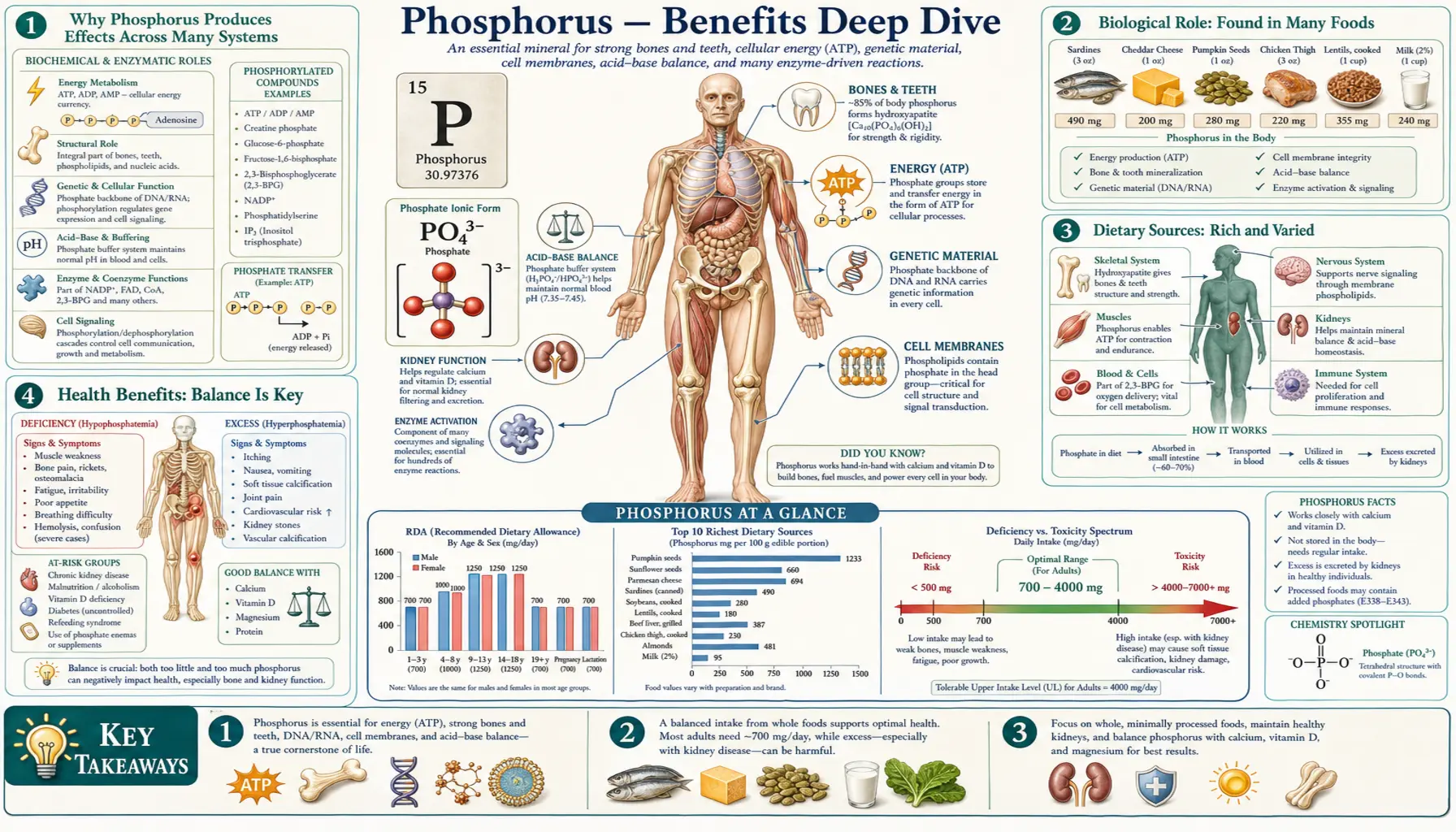
Phosphorus is the second most abundant mineral in the human body after calcium, present in every single cell as the phosphate group on ATP, the phosphodiester backbone of DNA and RNA, the polar head of every membrane phospholipid, the crystal lattice of every bone, and the buffering equilibrium that holds intracellular pH steady. Roughly 85 percent of the body's 600 to 700 grams of phosphorus is locked into bone as hydroxyapatite, and the remaining 15 percent does the chemistry of life everywhere else. Four benefit pages below explore the four domains where phosphorus chemistry produces the largest clinical effect — the universal ATP energy currency, the calcium-phosphate crystal of bone, the phospholipid bilayer that makes every cell membrane possible, and the buffer system that allows cellular biochemistry to run at constant pH.
Deep-Dive Articles
Energy Production
ATP structure and the high-energy phosphoanhydride bond (~7.3 kcal/mol per terminal phosphate), the phosphocreatine system as the cell's fastest ATP buffer, glycolytic phosphorylated intermediates (every step), mitochondrial oxidative phosphorylation through the rotary ATP synthase motor, and the clinical syndromes of severe hypophosphatemia, refeeding syndrome, and DKA-related phosphate shifts. The average adult turns over 40 to 70 kg of ATP per day — every gram of it built on phosphorus.
Bone Mineralization
Hydroxyapatite Ca10(PO4)6(OH)2 as 65 percent of bone mass, the Ca:P ratio (1.7:1 in bone), dietary Ca:P balance and bone health, the osteoblast / TNAP / pyrophosphate mineralization machinery, the PTH — FGF23 — calcitriol hormonal axis, X-linked hypophosphatemia and burosumab, renal osteodystrophy in CKD, and the hidden phosphate additives in processed food that accelerate vascular calcification.
Cell Membranes
Phospholipids as the universal bilayer building block (phosphatidylcholine, phosphatidylethanolamine, phosphatidylserine, phosphatidylinositol, sphingomyelin, cardiolipin), phosphoinositide signaling through PIP2 → IP3 + DAG and the PI3K / Akt / PIP3 pathway, lipid rafts as functional signaling microdomains, phosphatidylserine as the "eat-me" signal for apoptotic clearance, and the evidence on supplemental PS for cognition and athletic recovery.
Acid-Base Balance
Phosphate (H2PO4− ↔ HPO42−) with pKa 6.8 as the primary intracellular buffer, urinary phosphate as titratable acidity in daily renal acid excretion, phosphate shifts in diabetic ketoacidosis, the kidney's use of the phosphate buffer in renal tubular acidosis, and the under-recognized toxicity of phosphate-based enemas in vulnerable populations.
Table of Contents
- Deep-Dive Articles
- Why Phosphorus Produces Effects Across Many Systems
- Research Papers: Energy Production
- Research Papers: Bone Mineralization
- Research Papers: Cell Membranes
- Research Papers: Acid-Base Balance
- Research Papers: Cross-Cutting (Homeostasis, Toxicity, CKD)
- External Authoritative Resources
- Connections
- Featured Videos
Why Phosphorus Produces Effects Across Many Systems
Most minerals act through one or two principal mechanisms (calcium signaling at membrane channels; iron binding oxygen in heme; zinc as a structural cofactor in zinc-finger transcription factors). Phosphorus is unusual because it is the structural backbone of the chemistry of life itself. The phosphate group does five completely different jobs across five different molecular contexts, and each maps to a distinct category of clinical effect.
- ATP energy currency — the three phosphates of ATP store and transfer the energy that powers every cellular process. Each ATP ↔ ADP cycle moves a phosphate group and approximately 7.3 kcal/mol of free energy. The cell synthesizes ATP through both glycolytic substrate-level phosphorylation and the rotary ATP synthase motor of oxidative phosphorylation. This is the mechanism behind every energy-related effect of phosphorus — refeeding syndrome, hypophosphatemic muscle weakness, and the phosphocreatine reserve that powers explosive movement.
- Nucleic acid backbone — phosphodiester bonds link the sugar units of DNA and RNA. Without phosphate, no nucleic acid polymer can be assembled. The negative charge of the phosphate backbone is essential for DNA structure (the right-handed double helix), for chromatin organization (histones bind through positively charged amino acid clusters), and for the binding of nearly every transcription factor and DNA-binding regulatory protein.
- Phospholipid membranes — every cell membrane is a phospholipid bilayer. The phosphate head group is what makes the molecule amphipathic and the bilayer possible. Beyond structure, phosphoinositides (PIP2, PIP3) are central second-messenger lipids, phosphatidylserine on the outer leaflet is the apoptosis signal, and sphingomyelin dominates the myelin sheath. This is the mechanism behind much of the phospholipid-related biology and the supplemental phosphatidylserine evidence for cognition.
- Hydroxyapatite mineralization — Ca10(PO4)6(OH)2 is the crystal of bone and tooth enamel. 85 percent of body phosphorus is locked into this structure. The hormonal axis of PTH, FGF23, and calcitriol regulates the deposition and dissolution of the crystal. This is the mechanism behind rickets, osteomalacia, CKD-MBD, and the bone disease caused by chronic dietary phosphate excess.
- Phosphorylation cascades — protein phosphorylation is the most common post-translational modification in eukaryotic cells. The human genome encodes over 500 kinases that transfer phosphate from ATP to serine, threonine, or tyrosine residues on target proteins, switching them on or off. This is the mechanism behind the MAP kinase pathway, the PI3K / Akt / mTOR pathway, JAK / STAT signaling, and the cyclic-nucleotide second-messenger systems. Dysregulated phosphorylation drives most of human cancer.
Beyond all five of these structural and signaling roles, phosphate is the body's primary intracellular acid-base buffer with a pKa (6.8) perfectly matched to intracellular pH, and the urinary phosphate-bound titratable acidity is a major component of daily renal acid excretion. The same molecule that powers cellular biochemistry also holds the pH steady so the biochemistry can run.
The therapeutic asymmetry is striking. Too little phosphate is rapidly lethal (severe hypophosphatemia, refeeding-syndrome cardiac arrest). Too much phosphate is also lethal but on a longer timescale (CKD-MBD, vascular calcification, accelerated cardiovascular mortality). The healthy kidney is the master regulator of phosphate balance through tightly tuned PTH and FGF23 signaling; when that regulation fails, both bone disease and vascular calcification follow. For most healthy adults the dietary intake from whole foods is adequate or excessive; the practical concerns are hidden inorganic phosphate additives in processed food (which are absorbed at roughly 90 percent efficiency, compared with roughly 60 percent for naturally occurring organic phosphate) and the CKD-MBD cascade in patients with impaired kidney function.
Warning — hidden phosphate additives. Inorganic phosphate salts (sodium phosphate, potassium phosphate, hexametaphosphate, pyrophosphate) are added to a wide range of processed foods as preservatives, emulsifiers, leavening agents, and color stabilizers. Common offenders include processed meats and deli meats, processed cheese spreads, dark cola drinks (phosphoric acid), baking powder, instant pudding mixes, non-dairy creamers, and many bottled and canned beverages. These additives are absorbed at roughly 90 percent efficiency — substantially higher than the roughly 60 percent absorption rate of organic phosphate naturally present in whole foods. For healthy adults, modest additive intake is unlikely to cause acute harm, but for any patient with reduced kidney function — even early CKD that may not yet be diagnosed — the additive burden accelerates vascular calcification, elevates FGF23 chronically, and drives the entire CKD-MBD cascade. Read ingredient lists for any added "phosphate" or "phosphoric acid" and favor whole foods.
Research Papers: Energy Production
- Boyer PD (1997). The ATP synthase — a splendid molecular machine. Annual Review of Biochemistry. — PubMed: Boyer 1997
- Mitchell P (1961). Coupling of phosphorylation to electron and hydrogen transfer by a chemi-osmotic type of mechanism. Nature. — PubMed: Mitchell 1961
- Wallimann T et al. (1992). Intracellular compartmentation, structure and function of creatine kinase isoenzymes ("phosphocreatine circuit"). Biochemical Journal. — PubMed: Phosphocreatine circuit
- Subramanian R, Khardori R (2000). Severe hypophosphatemia: pathophysiologic implications. Medicine. — PubMed: Severe hypophosphatemia
- Mehanna HM et al. (2008). Refeeding syndrome: what it is, how to prevent and treat it. BMJ. — PubMed: Refeeding syndrome BMJ
- Hultman E et al. (1996). Muscle creatine loading in men. Journal of Applied Physiology. — PubMed: Hultman creatine loading
- Friedli N et al. (2018). Management of refeeding syndrome: evidence-based algorithm. Nutrition. — PubMed: Friedli algorithm
- Knochel JP (1977). The pathophysiology and clinical characteristics of severe hypophosphatemia. Archives of Internal Medicine. — PubMed: Knochel classic
- Walker JE (2013). The ATP synthase: the understood, the uncertain and the unknown. BST. — PubMed: ATP synthase Walker
- Brosnan ME, Brosnan JT (2016). The role of dietary creatine. Amino Acids. — PubMed: Dietary creatine
Research Papers: Bone Mineralization
- Murshed M (2018). Mechanism of bone mineralization. Cold Spring Harbor Perspectives in Medicine. — PubMed: Murshed mineralization
- Boskey AL (2013). Bone composition: relationship to bone fragility. BoneKEy Reports. — PubMed: Boskey bone composition
- Whyte MP (2010). Physiological role of alkaline phosphatase explored in hypophosphatasia. Annals NYAS. — PubMed: Alkaline phosphatase
- Quarles LD (2012). Skeletal secretion of FGF-23 regulates phosphate and vitamin D metabolism. Nature Reviews Endocrinology. — PubMed: FGF23 review
- Carpenter TO et al. (2018). Burosumab therapy in children with X-linked hypophosphatemia. NEJM. — PubMed: Burosumab NEJM
- Razzaque MS (2009). The FGF23-Klotho axis: endocrine regulation of phosphate homeostasis. Nature Reviews Endocrinology. — PubMed: FGF23-Klotho
- Moe SM et al. (2006). Definition and classification of renal osteodystrophy and CKD-MBD. Kidney International. — PubMed: CKD-MBD definition
- Block GA et al. (2004). Mineral metabolism, mortality, and morbidity in maintenance hemodialysis. JASN. — PubMed: Mineral mortality dialysis
- Calvo MS, Uribarri J (2013). Public health impact of dietary phosphorus excess. AJCN. — PubMed: Dietary phosphorus excess
- Tucker KL et al. (2006). Colas associated with low bone mineral density in older women (Framingham). AJCN. — PubMed: Cola and bone
Research Papers: Cell Membranes
- Vance JE (2015). Phospholipid synthesis and transport in mammalian cells. Traffic. — PubMed: Vance phospholipid synthesis
- Balla T (2013). Phosphoinositides: tiny lipids with giant impact on cell regulation. Physiological Reviews. — PubMed: Balla phosphoinositides
- Berridge MJ (2009). Inositol trisphosphate and calcium signalling mechanisms. BBA. — PubMed: Berridge IP3
- Cantley LC (2002). The phosphoinositide 3-kinase pathway. Science. — PubMed: Cantley PI3K
- Lingwood D, Simons K (2010). Lipid rafts as a membrane-organizing principle. Science. — PubMed: Lipid rafts
- Leventis PA, Grinstein S (2010). The distribution and function of phosphatidylserine in cellular membranes. Annual Review of Biophysics. — PubMed: PS distribution
- Fadok VA et al. (1992). Exposure of phosphatidylserine triggers macrophage recognition. J Immunology. — PubMed: PS apoptosis signal
- Glade MJ, Smith K (2015). Phosphatidylserine and the human brain. Nutrition. — PubMed: PS and brain
- Monteleone P et al. (1992). Blunting by chronic PS administration of stress-induced HPA activation. EJCP. — PubMed: PS HPA blunting
- Zeisel SH, da Costa KA (2009). Choline: an essential nutrient for public health. Nutrition Reviews. — PubMed: Choline essential
Research Papers: Acid-Base Balance
- Hamm LL et al. (2015). Acid-base homeostasis. CJASN. — PubMed: Acid-base homeostasis
- Adrogué HJ, Madias NE (1998). Management of life-threatening acid-base disorders. NEJM. — PubMed: Acid-base NEJM
- Kitabchi AE et al. (2009). Hyperglycemic crises in adult patients with diabetes. Diabetes Care. — PubMed: DKA Kitabchi
- Fisher JN, Kitabchi AE (1983). A randomized study of phosphate therapy in DKA. JCEM. — PubMed: Phosphate in DKA
- de Brito-Ashurst I et al. (2009). Bicarbonate supplementation slows CKD progression. JASN. — PubMed: Bicarbonate CKD
- Markowitz GS, Perazella MA (2009). Acute phosphate nephropathy. Kidney International. — PubMed: Phosphate nephropathy
- Ori Y et al. (2012). Fatalities with sodium phosphate enemas. Archives of Internal Medicine. — PubMed: Enema fatalities
- DuBose TD Jr (1997). Hyperkalemic hyperchloremic metabolic acidosis. Kidney International. — PubMed: Type 4 RTA
- Rodriguez Soriano J (2002). Renal tubular acidosis: the clinical entity. JASN. — PubMed: RTA review
- Lemann J Jr et al. (2003). Bone buffering of acid and base in humans. AJP Renal. — PubMed: Bone buffering
Research Papers: Cross-Cutting (Homeostasis, Toxicity, CKD)
- Bergwitz C, Jüppner H (2010). Regulation of phosphate homeostasis by PTH, vitamin D, and FGF23. Annual Review of Medicine. — PubMed: Phosphate homeostasis
- KDIGO Clinical Practice Guideline for CKD-MBD (2017 Update). — PubMed: KDIGO CKD-MBD
- Tonelli M et al. (2009). Phosphate and cardiovascular disease. Kidney International. — PubMed: Phosphate and CVD
- Faul C et al. (2011). FGF23 induces left ventricular hypertrophy. Journal of Clinical Investigation. — PubMed: FGF23 and LVH
- Uribarri J, Calvo MS (2014). Hidden phosphorus in the typical American diet. Seminars in Dialysis. — PubMed: Hidden phosphorus
- Chang AR et al. (2014). High dietary phosphorus intake and all-cause mortality in NHANES III. AJCN. — PubMed: Dietary P and mortality
- Hruska KA et al. (2008). Hyperphosphatemia of chronic kidney disease. Kidney International. — PubMed: Hyperphosphatemia CKD
- Isakova T et al. (2011). FGF23 and risks of mortality and end-stage renal disease in CKD. JAMA. — PubMed: FGF23 mortality
- Goyal R, Jialal I (2023). Hyperphosphatemia. StatPearls. — PubMed: Hyperphosphatemia review
- Sherman RA, Mehta O (2009). Phosphorus and potassium content of enhanced meat and poultry products. CJASN. — PubMed: Additive phosphorus
External Authoritative Resources
- Linus Pauling Institute — Phosphorus Micronutrient Information Center — the single most authoritative scientific summary of phosphorus biology, regularly updated
- NIH Office of Dietary Supplements — Phosphorus Fact Sheet (Health Professionals)
- National Kidney Foundation — Phosphorus and Your CKD Diet
- KDIGO — CKD-MBD Clinical Practice Guideline (the global standard for managing the bone-mineral disorder of chronic kidney disease)
- MedlinePlus — Phosphorus in Diet
- PubMed — All research on phosphorus / phosphate in human biology
Connections
- Phosphorus (Main Page)
- Phosphorus for Energy Production
- Phosphorus for Bone Mineralization
- Phosphorus for Cell Membranes
- Phosphorus for Acid-Base Balance
- All Minerals
- Calcium
- Calcium and Bone Health
- Magnesium
- Potassium
- Vitamin D3
- Vitamin K (K2 for Bone)
- Vitamin B6 (PLP)
- Vitamin B1 (TPP)
- Creatine
- Omega-3 Fatty Acids
- Organ Meats (Beef Liver)
- Eggs
- Salmon
- Osteoporosis
- Hyperparathyroidism
- Kidney Disease
- Cardiovascular Disease
- eGFR
- Kidney Function Tests