eGFR (Estimated Glomerular Filtration Rate): Stages and Interpretation
Estimated glomerular filtration rate (eGFR) is the single most important number for staging chronic kidney disease. It is not measured directly — it is calculated from serum creatinine using a regression equation that adjusts for age and sex. The current US standard is the 2021 race-free CKD-EPI equation, which replaced the 2009 version after a 2020 NKF/ASN task force recommended dropping the race coefficient. Combined with urine albumin-to-creatinine ratio (ACR), eGFR forms the backbone of CKD diagnosis, staging, and risk stratification.
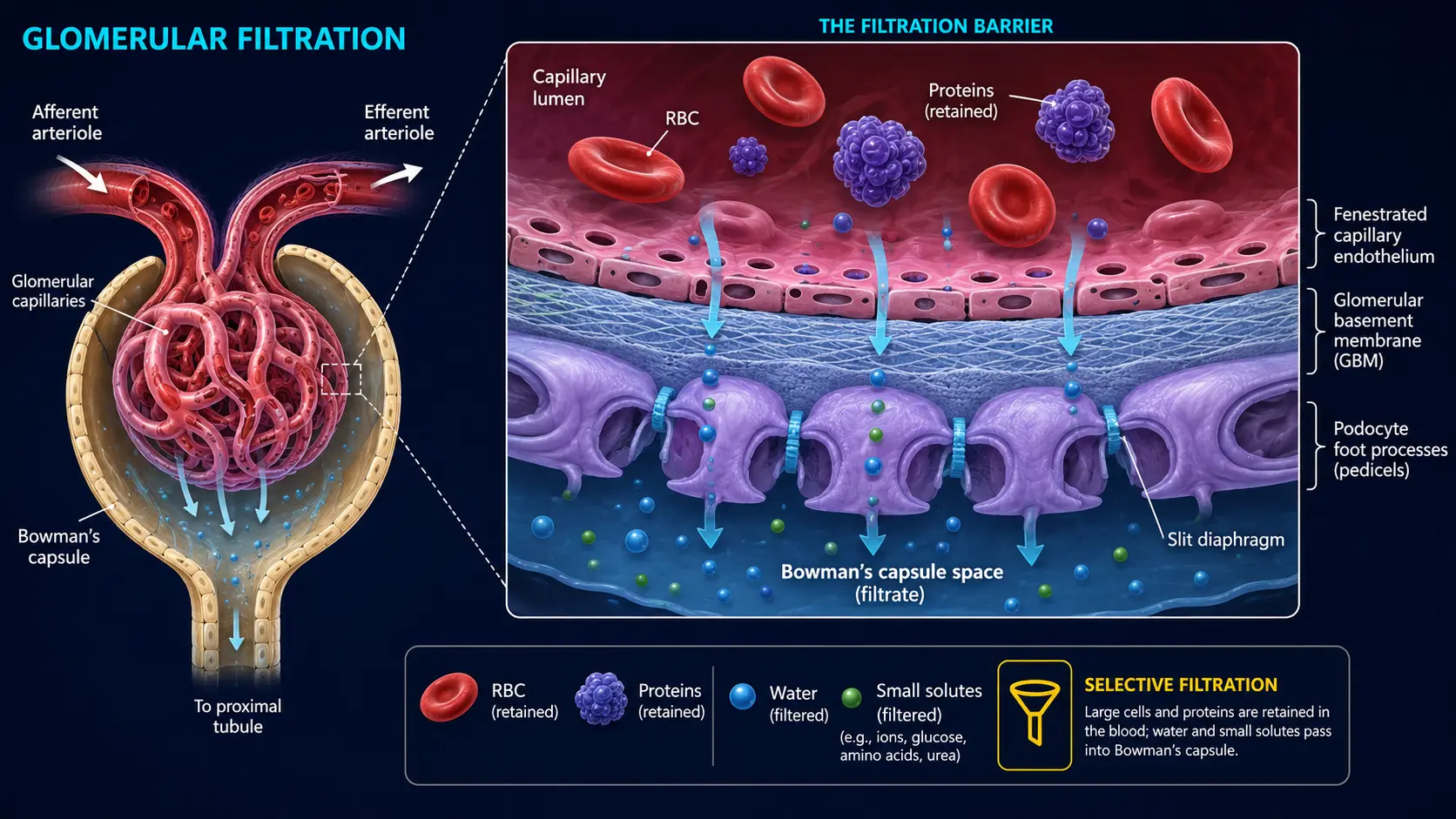
Interactive Visualization Kidney Nephron — watch blood become urine Follow blood into the glomerulus and see filtration and reabsorption turn 180 litres of filtrate into urine — then toggle dehydration or diabetes. Launch →Table of Contents
- What eGFR Measures
- The Equations: CKD-EPI 2021
- Reference Range
- CKD Stages G1–G5
- Combined G/A Staging
- Where eGFR Misleads
- Cystatin C eGFR and Combined Equations
- Trajectory Matters More Than Snapshots
- What to Do at Each Stage
- Research Papers and References
- Connections
- Featured Videos
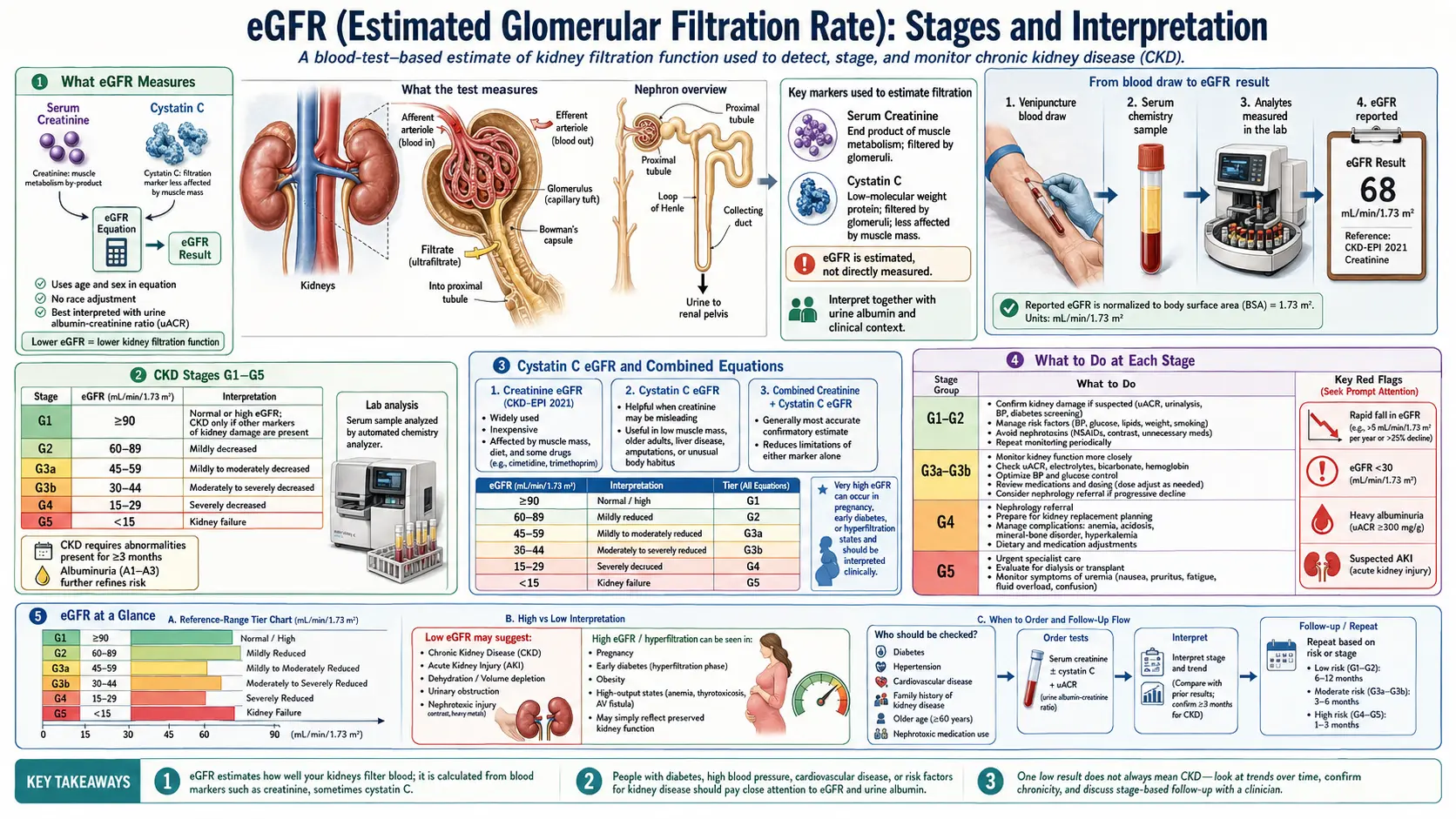
What eGFR Measures
The glomerular filtration rate is the volume of plasma the kidneys clear per minute, normalized to a body surface area of 1.73 m². A young, healthy adult typically has a measured GFR around 100–130 mL/min/1.73 m². The "estimated" prefix indicates that the number on your lab report comes from a formula, not a direct measurement of inulin clearance or iohexol clearance (the gold standards, used mainly in research and transplant evaluation).
eGFR is the variable used to stage CKD, decide which medications to start or stop, dose-adjust drugs cleared renally, time pre-dialysis education and vascular access creation, and counsel patients about prognosis. Most clinical decisions are anchored to eGFR rather than serum creatinine alone, because eGFR adjusts for the demographic factors that bend the creatinine–GFR relationship.
The Equations: CKD-EPI 2021
The 2021 CKD-EPI creatinine equation uses serum creatinine, age, and sex (no race coefficient). For most patients, the formula yields:
- Female, creatinine ≤ 0.7 mg/dL: eGFR = 142 × (Cr/0.7)-0.241 × 0.9938age × 1.012
- Female, creatinine > 0.7 mg/dL: eGFR = 142 × (Cr/0.7)-1.200 × 0.9938age × 1.012
- Male, creatinine ≤ 0.9 mg/dL: eGFR = 142 × (Cr/0.9)-0.302 × 0.9938age
- Male, creatinine > 0.9 mg/dL: eGFR = 142 × (Cr/0.9)-1.200 × 0.9938age
You don't need to compute it by hand — every modern laboratory information system reports eGFR alongside serum creatinine. Online calculators are available at the National Kidney Foundation site if you ever need to recompute one yourself.
Why the change from the 2009 equation? The 2009 CKD-EPI equation included a race coefficient that multiplied results by 1.16 for Black patients. This systematically over-estimated eGFR in Black patients, delaying CKD diagnosis, transplant listing, and nephrology referral. The 2021 equation drops the coefficient. Most laboratories transitioned during 2022–2023.
Reference Range
eGFR (mL/min/1.73 m²)
The "normal" range collapses with age. A measured GFR of 70 mL/min/1.73 m² in an 80-year-old is consistent with healthy aging; the same value in a 30-year-old is a red flag. eGFR formulas already adjust for age, but the population reference at age 80 is meaningfully lower than at age 30.
CKD Stages G1–G5
The KDIGO 2012 framework defines six G-stages based on eGFR:
- G1 — eGFR ≥ 90: normal or high. Considered CKD only with concomitant albuminuria, structural abnormalities, or known kidney pathology.
- G2 — eGFR 60–89: mildly decreased. Same caveat as G1; mild reduction alone does not equal CKD.
- G3a — eGFR 45–59: mildly to moderately decreased. CKD diagnosed regardless of other findings if persistent ≥ 3 months.
- G3b — eGFR 30–44: moderately to severely decreased. Risk of cardiovascular events and progression rises sharply; nephrology consultation recommended.
- G4 — eGFR 15–29: severely decreased. Mandatory nephrology involvement; patient education on dialysis modalities and transplant; vascular access planning if hemodialysis is anticipated.
- G5 — eGFR < 15: kidney failure. Dialysis or transplant evaluation; symptomatic uremia is common.
Combined G/A Staging
KDIGO recommends combining G stage with A stage (urine ACR) because albuminuria predicts cardiovascular events and progression independently of eGFR:
- A1: ACR < 30 mg/g (normal to mildly increased)
- A2: ACR 30–300 mg/g (moderately increased; formerly "microalbuminuria")
- A3: ACR > 300 mg/g (severely increased; formerly "macroalbuminuria")
The combined stage (e.g., G3a A2) maps onto risk categories: green (low risk), yellow (moderate), orange (high), red (very high). A patient with eGFR 65 (G2) and ACR 250 (A2) has higher cardiovascular and progression risk than a patient with eGFR 50 (G3a) and ACR 10 (A1).
Where eGFR Misleads
Because eGFR is calculated from creatinine, every limitation of creatinine carries through. The most common pitfalls:
- Extremes of muscle mass — eGFR overestimates GFR in frail, sarcopenic, or amputee patients (creatinine is low because of low muscle, not good filtration). It underestimates in heavily muscled patients (creatinine is high because of high muscle). Use cystatin C-based eGFR in either case.
- Acute kidney injury — eGFR formulas assume steady-state creatinine. During AKI, creatinine is rising rapidly, so eGFR computed from a single creatinine value overestimates current GFR.
- Pregnancy — physiologic hyperfiltration; standard eGFR formulas underestimate true GFR. Pregnancy-specific equations exist but are seldom used clinically.
- Drug-induced creatinine bumps — cimetidine, trimethoprim, fenofibrate, cobicistat, dolutegravir all raise serum creatinine without changing GFR; eGFR will appear to drop.
- Children — CKD-EPI is for adults; pediatric nephrology uses the Bedside Schwartz formula.
- Borderline ranges — the difference between an eGFR of 58 and 62 is within the equation's confidence interval. Trends over months matter more than single readings near the cut-off.
Cystatin C eGFR and Combined Equations
The 2021 CKD-EPI race-free cystatin C equation gives an eGFR independent of muscle mass. The 2021 CKD-EPI creatinine + cystatin C combined equation outperforms either alone in research validation studies. KDIGO 2024 guidelines recommend combined-equation eGFR when the creatinine-only result seems implausible for the patient's body composition or when an early CKD diagnosis would change management. See the Cystatin C page for a deeper walk-through.
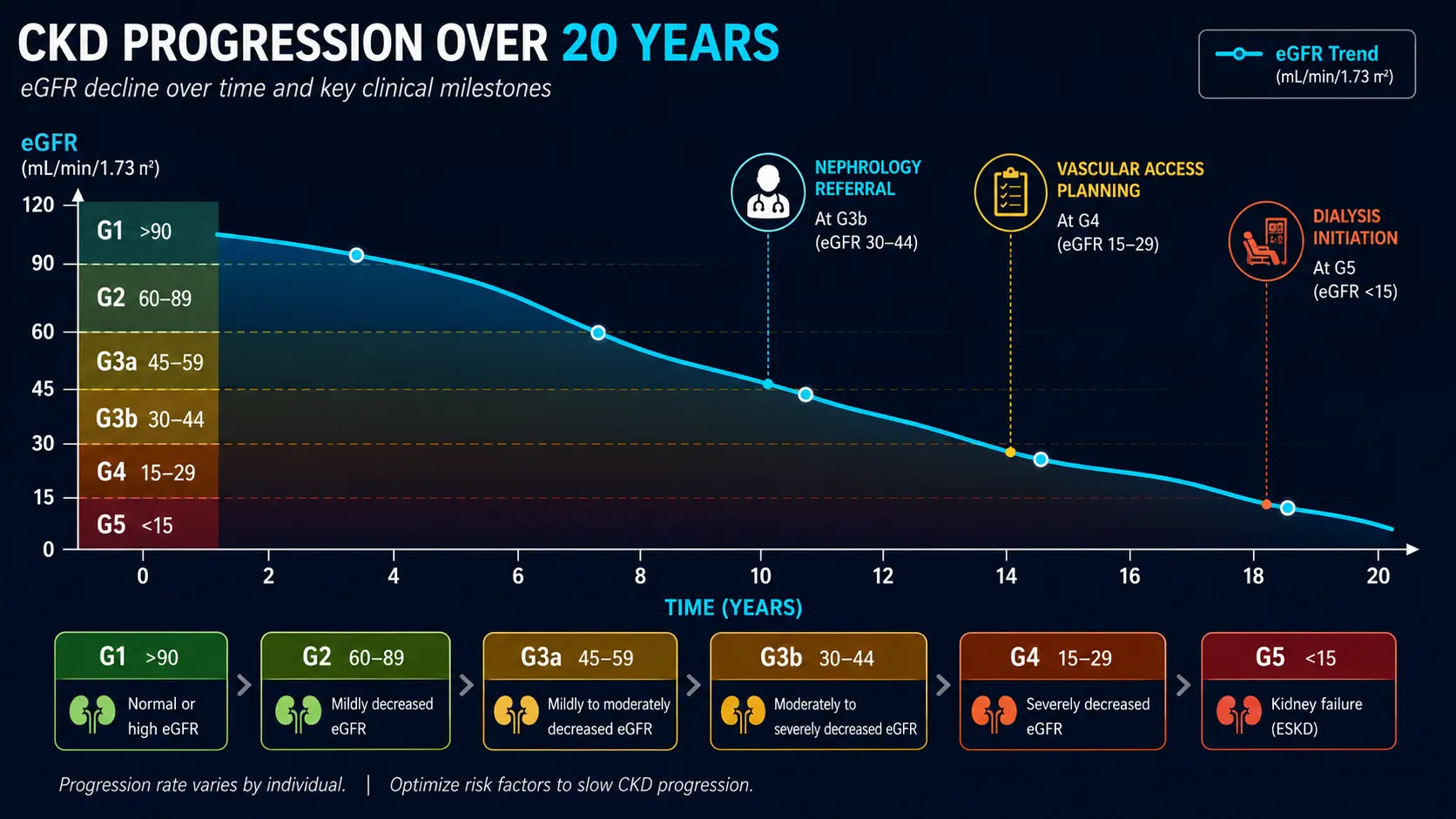
Trajectory Matters More Than Snapshots
A single eGFR is a snapshot. Two trajectories tell two completely different stories:
- Stable CKD — eGFR around 50 for 5 years. Low risk of dialysis. Manage cardiovascular risk, treat blood pressure, keep blood sugar in range.
- Rapidly progressive CKD — eGFR has dropped from 75 to 50 in 18 months. Mandatory nephrology referral; rule out reversible causes (obstruction, drugs, autoimmune disease, untreated hypertension).
A loss of more than 5 mL/min/1.73 m² per year is "rapid progression" and warrants intensive workup. The slope, not any single value, drives prognosis.
What to Do at Each Stage
G1–G2 (eGFR ≥ 60): Annual screening if at risk (diabetes, hypertension, family history, NSAIDs, lithium). Treat blood pressure to < 130/80, optimize HbA1c, avoid chronic NSAIDs, hydrate around contrast.
G3a (eGFR 45–59): Confirm with a repeat in 3 months (CKD requires persistence). Add ACE inhibitor or ARB if proteinuric or hypertensive. Add SGLT2 inhibitor if diabetic. Annual check of CBC (anemia of CKD), calcium/phosphate/PTH, and vitamin D.
G3b (eGFR 30–44): Nephrology consult. Avoid contrast where possible; dose-adjust medications. Active management of bone-mineral disease (phosphate binders if needed). Monitor potassium tightly.
G4 (eGFR 15–29): Multidisciplinary CKD clinic. Vascular access planning (hemodialysis fistula if > 6 months anticipated). Transplant evaluation. Dietary potassium and phosphate restriction. Anemia management (iron, ESA).
G5 (eGFR < 15): Dialysis initiation when symptomatic or when biochemical/fluid issues become unmanageable. Pre-emptive transplant if feasible.
For supportive measures across all stages: anti-inflammatory diet, blood sugar protocols, magnesium, and reviewing the medication list at every visit are the highest-leverage habits.
Research Papers and References
- 2021 race-free CKD-EPI equation — PubMed search
- KDIGO CKD staging guidelines — PubMed search
- eGFR slope and CKD progression — PubMed search
- Cystatin C combined eGFR — PubMed search
- Combined G/A staging and outcomes — PubMed search
- SGLT2 inhibitors and eGFR protection — PubMed search
- ACE inhibitors and CKD progression — PubMed search
External Authoritative Resources
- National Kidney Foundation — eGFR Calculator
- KDIGO CKD Evaluation and Management Guideline
- MedlinePlus — GFR Test
Connections
- Kidney Nephron — interactive animation
- Understanding Your eGFR & CKD Stage
- Cystatin C
- Creatinine
- BUN
- Kidney Function Tests
- Comprehensive Metabolic Panel
- Urinalysis
- Kidney Disease
- Acute Kidney Injury
- Hypertension
- Diabetes
- Anemia
- Magnesium
- Potassium
- Anti-Inflammatory Diet
- Blood Sugar
- Phosphorus
- Gout
- Hyperparathyroidism