Phosphorus for Bone Mineralization
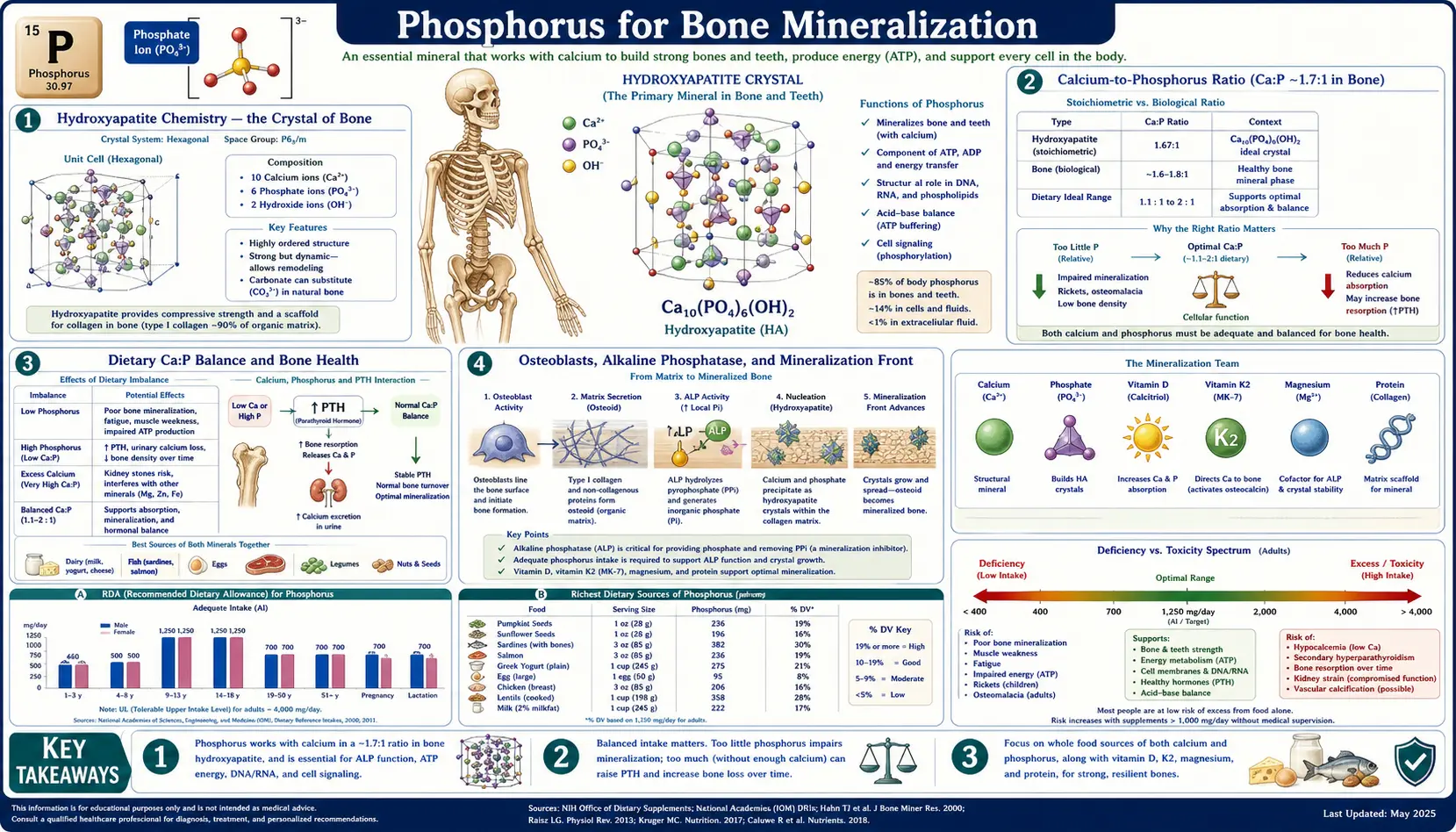
Approximately 85 percent of the body's total phosphorus is locked into the mineral crystal of bone and tooth enamel. The crystal is hydroxyapatite, Ca10(PO4)6(OH)2, a calcium-phosphate lattice that accounts for roughly 65 percent of bone mass and gives bone its compressive strength. Bone is not a static reservoir of these minerals; it is continuously remodeled by osteoblasts depositing new hydroxyapatite and osteoclasts dissolving old crystal, with the entire skeleton turning over once every roughly ten years in adulthood. The dietary calcium-to-phosphorus ratio, the hormonal axis of parathyroid hormone (PTH) and fibroblast growth factor 23 (FGF23), and active vitamin D (calcitriol) together regulate every step. This deep-dive walks through the chemistry of hydroxyapatite, the cellular machinery of mineralization, the genetics of inherited rickets, and the renal osteodystrophy of chronic kidney disease — the largest preventable cause of skeletal failure in the developed world.
Table of Contents
- Hydroxyapatite Chemistry — the Crystal of Bone
- The Calcium-to-Phosphorus Ratio (Ca:P ~ 1.7:1 in Bone)
- Dietary Ca:P Balance and Bone Health
- Osteoblasts, Alkaline Phosphatase, and the Mineralization Front
- The PTH — FGF23 — Vitamin D Hormonal Axis
- Tooth Enamel and Fluorapatite
- Hypophosphatemic Rickets — XLH, ADHR, and Tumor-Induced Osteomalacia
- Renal Osteodystrophy and CKD-MBD
- The Hidden Phosphate Additives Problem
- Clinical Applications and Monitoring
- Key Research Papers
- Connections
- Featured Videos
Hydroxyapatite Chemistry — the Crystal of Bone
Hydroxyapatite is the principal mineral of vertebrate skeletons. Its empirical formula is Ca10(PO4)6(OH)2 — ten calcium ions, six phosphate groups, and two hydroxide ions arranged in a hexagonal crystal lattice. By weight, the crystal is roughly 40 percent calcium, 18 percent phosphorus, 4 percent oxygen as hydroxide, and the remainder bridging oxygen in the phosphate groups. Phosphate accounts for approximately 50 percent of bone mineral mass and the entire crystal is approximately 65 percent of bone tissue mass — the remainder being primarily collagen type I, which forms the organic scaffold on which the crystal is deposited.
The lattice is unusually accommodating to substitutions. Strontium, magnesium, lead, and other divalent cations can substitute for calcium. Fluoride can substitute for hydroxide (producing fluorapatite, which is harder and more acid-resistant than hydroxyapatite; this is the basis of the cariostatic effect of dietary and topical fluoride on tooth enamel). Carbonate ions can substitute for phosphate (producing carbonate apatite, the form that predominates in living bone and is more soluble than pure hydroxyapatite, giving bone the ability to release calcium and phosphate into circulation during periods of dietary deficiency).
The crystals themselves are nanoscale — roughly 50 nm long, 25 nm wide, and 2 to 4 nm thick — embedded in and aligned with the collagen fibrils of the bone matrix. The huge surface area to volume ratio of these tiny crystals is what allows bone to participate in mineral homeostasis on a daily basis. Roughly 1 percent of bone mineral is exchangeable with the extracellular fluid at any time — enough to buffer transient swings in serum calcium or phosphate — while the bulk of the crystal forms the structural mass that gives bone its compressive strength.
The Calcium-to-Phosphorus Ratio (Ca:P ~ 1.7:1 in Bone)
By moles, the calcium-to-phosphorus stoichiometry of pure hydroxyapatite is 10:6, or approximately 1.67:1. By mass, the ratio is approximately 2.15:1 (since calcium's atomic mass of 40 is greater than phosphorus's 31). The molar ratio of 1.67:1 is the closest thing biology has to a fixed structural requirement for the relative amounts of calcium and phosphorus deposited into mineralized bone.
Whole-body, the picture is similar. An adult contains roughly 1,000–1,200 grams of calcium (99 percent in bone) and roughly 600–700 grams of phosphorus (85 percent in bone). The whole-body Ca:P mass ratio is therefore approximately 1.7:1, very close to the molar ratio of the underlying hydroxyapatite.
The clinical and dietary literature historically focused on the dietary Ca:P ratio as a determinant of bone health, with concern that a low dietary Ca:P ratio (excess phosphorus relative to calcium) might drive secondary hyperparathyroidism, increase bone resorption, and accelerate bone loss. The mechanism: high dietary phosphate slightly raises serum phosphate, which complexes with serum calcium and lowers ionized calcium, which triggers PTH secretion, which mobilizes calcium and phosphate from bone. Whether this mechanism actually translates to net skeletal harm at modest dietary imbalances in healthy adults with normal kidney function has been debated for decades; modern consensus is that the effect is small or absent in healthy people with adequate calcium intake, but becomes clinically meaningful at extremes (very high phosphate from processed food in adults with marginal calcium intake) and in any patient with impaired kidney function.
Dietary Ca:P Balance and Bone Health
The dietary recommended intakes (DRIs) for adults are 1,000 mg/day of calcium and 700 mg/day of phosphorus — a dietary Ca:P mass ratio of approximately 1.4:1. The typical Western diet delivers approximately 600–1,000 mg of calcium (often below the recommendation) and 1,200–1,800 mg of phosphorus (well above the recommendation), giving a dietary Ca:P ratio that frequently runs 0.4:1 to 0.7:1 — substantially inverted relative to the structural ratio in bone.
The reasons for the inversion are dietary. Phosphorus is abundant in almost every protein-rich food (meat, fish, dairy, eggs, legumes, nuts, whole grains all contribute), in addition to the inorganic phosphate added to processed food and soft drinks as a stabilizer, preservative, and leavening agent. Calcium, by contrast, is concentrated in only a few food groups — dairy products, calcium-set tofu, leafy greens (where bioavailability is reduced by oxalate in spinach and other high-oxalate foods), small bone-in fish (sardines, canned salmon), and fortified foods. Adults who skip dairy without deliberate calcium replacement frequently fall below adequate calcium intake while easily meeting (or exceeding) phosphorus intake.
For most healthy adults with normal kidney function, the practical implication is modest: aim to meet the calcium DRI (1,000–1,200 mg/day depending on age and sex), don't obsess about phosphorus restriction, but do limit processed-food inorganic phosphate additives (see the additives section below) and dark soft drinks. For older adults concerned about bone density, see our Osteoporosis page; for the role of vitamin D in calcium absorption, see our Vitamin D3 page; for vitamin K2's role in directing calcium into bone rather than soft tissue, see our Vitamin K page.
Osteoblasts, Alkaline Phosphatase, and the Mineralization Front
Bone mineralization is an active, regulated cellular process, not a passive precipitation. The cells responsible are osteoblasts — bone-forming cells derived from mesenchymal stem cells in the periosteum and bone marrow stroma. Osteoblasts secrete the unmineralized organic matrix of bone (called osteoid), which consists primarily of type I collagen plus a small amount of non-collagenous proteins (osteocalcin, osteonectin, osteopontin, bone sialoprotein). The newly deposited osteoid is then mineralized over the following days to weeks by the controlled deposition of hydroxyapatite crystals in and around the collagen fibrils.
The biochemistry of mineralization centers on a single enzyme: tissue-nonspecific alkaline phosphatase (TNAP), anchored to the surface of osteoblasts and the membrane vesicles they bud off (matrix vesicles, the primary nucleation sites for new crystals). TNAP cleaves pyrophosphate (PPi), a potent inhibitor of hydroxyapatite crystal formation, into two molecules of inorganic phosphate (Pi). The reaction does two things at once: it removes the inhibitor, and it increases the local concentration of Pi available for incorporation into new crystal. The crystals nucleate on calcium-phosphate-binding proteins anchored to collagen and grow outward into the matrix.
Genetic loss of TNAP function causes hypophosphatasia, a rare autosomal disorder in which pyrophosphate accumulates, hydroxyapatite cannot form normally, and the patient develops a clinical picture indistinguishable from rickets despite normal calcium, phosphate, and vitamin D status. The disorder demonstrates the central role of phosphorus chemistry in mineralization — even with all the substrate present, without the enzyme to remove the inhibitor, no crystal can form.
Osteoclasts, the bone-resorbing cells derived from the monocyte/macrophage lineage, perform the opposite operation. They acidify a small extracellular compartment (the resorption pit or sealed zone) to pH 4.5, dissolving the hydroxyapatite crystal back into calcium and phosphate ions and releasing collagen-degrading enzymes (cathepsin K, matrix metalloproteinases). The released calcium and phosphate re-enter circulation, providing the largest minute-to-minute source of these minerals for any need elsewhere in the body. The balance between osteoblast deposition and osteoclast resorption is what determines whether bone mass is gained, maintained, or lost over time — the basis of all the bone-density pharmacology used in osteoporosis treatment.
The PTH — FGF23 — Vitamin D Hormonal Axis
Three hormones do the bulk of phosphate regulation:
- Parathyroid hormone (PTH) — secreted by the parathyroid glands in response to low serum ionized calcium. PTH raises serum calcium (by mobilizing it from bone, increasing renal reabsorption, and stimulating active vitamin D synthesis) and lowers serum phosphate (by promoting urinary phosphate excretion through internalization of the proximal-tubule sodium-phosphate cotransporters NaPi-IIa and NaPi-IIc).
- Fibroblast growth factor 23 (FGF23) — secreted by osteocytes (terminally differentiated osteoblasts buried inside the mineralized matrix) in response to high serum phosphate and high active vitamin D. FGF23 acts on the kidney through the FGFR1c receptor and its obligate co-receptor alpha-Klotho to suppress renal phosphate reabsorption (driving phosphate into the urine) and to suppress 1-alpha-hydroxylase, the enzyme that activates vitamin D in the kidney. The net effect is to lower serum phosphate and to limit further intestinal phosphate absorption.
- Active vitamin D (1,25-dihydroxyvitamin D, calcitriol) — the active hormonal form of vitamin D, synthesized in the proximal renal tubule from 25-hydroxyvitamin D by 1-alpha-hydroxylase under PTH stimulation. Calcitriol increases intestinal absorption of both calcium and phosphate, increases renal calcium reabsorption (modestly), and feeds back to suppress PTH secretion.
The integration works like this: when serum calcium falls, PTH rises, mobilizes calcium from bone, increases renal calcium reabsorption, stimulates active vitamin D synthesis, and dumps phosphate into the urine to prevent serum phosphate from rising (which would otherwise complex with the calcium and defeat the purpose). When serum phosphate rises (from a large meal, from cellular catabolism, from impaired renal clearance), FGF23 rises, suppresses renal phosphate reabsorption (dumping phosphate into urine), and suppresses active vitamin D synthesis (limiting further intestinal absorption). The system is elegant, fast (PTH responds within minutes), and quantitatively powerful (renal phosphate reabsorption can swing from 90 percent reabsorbed under conservation conditions to less than 30 percent reabsorbed under high-FGF23 phosphaturic conditions).
When the system fails — either through gland dysfunction (hyperparathyroidism, hypoparathyroidism) or through end-organ failure (renal failure with loss of phosphate clearance and impaired calcitriol synthesis) — the consequences for bone are profound. For more on parathyroid pathology, see our Hyperparathyroidism page.
Tooth Enamel and Fluorapatite
Tooth enamel is the hardest tissue in the human body. It is approximately 96 percent mineral by weight (versus 65 percent for bone), with the remaining 4 percent water and organic matrix (proteins called enamelins and amelogenins, plus a small amount of lipid). The mineral is a particularly dense and well-ordered form of hydroxyapatite, organized into long enamel prisms that run perpendicular to the tooth surface and give enamel its strength.
Fluoride is the single most important environmental modifier of enamel chemistry. When fluoride is present during enamel formation (early childhood) or during demineralization-remineralization cycles in the mouth, fluoride substitutes for hydroxide in the apatite lattice, producing fluorapatite, Ca10(PO4)6F2. Fluorapatite is harder than hydroxyapatite, more resistant to acid demineralization (the pKa of dissolution shifts from approximately 5.5 for hydroxyapatite to approximately 4.5 for fluorapatite), and remineralizes faster from oral calcium and phosphate. The community-water-fluoridation public-health intervention is built on this chemistry — trace fluoride in drinking water shifts the demineralization-remineralization balance in favor of remineralization, reducing dental caries by approximately 25 percent at the population level.
Phosphate supply matters for enamel just as it does for bone. Severe hypophosphatemic rickets (see next section) produces enamel hypoplasia and increased caries susceptibility, and adults with chronic hypophosphatemia or severe vitamin D deficiency in childhood often carry permanent enamel defects.
Hypophosphatemic Rickets — XLH, ADHR, and Tumor-Induced Osteomalacia
Rickets is the clinical syndrome of impaired mineralization of the growth plate in children, producing bowed long bones, frontal bossing, rachitic rosary at the costochondral junctions, and growth retardation. Osteomalacia is the same mineralization failure in the mature skeleton of adults, producing diffuse bone pain, fractures, and proximal muscle weakness. Both syndromes can be caused by vitamin D deficiency (the classic "nutritional rickets" that drove the original cod liver oil intervention), by calcium deficiency, or by phosphate deficiency — and the phosphate-driven forms are the ones least well-served by vitamin D treatment alone.
The most important inherited phosphate-wasting disorders are all driven by excess FGF23 signaling:
- X-linked hypophosphatemia (XLH) — the most common inherited form, caused by loss-of-function mutations in PHEX, an endopeptidase normally expressed by osteocytes and osteoblasts that limits FGF23 activity. Without PHEX, FGF23 rises, the kidney wastes phosphate, serum phosphate is chronically low, and rickets develops. Historical treatment was high-dose oral phosphate plus active vitamin D, with limited success and significant treatment burden. Burosumab (a humanized monoclonal antibody against FGF23) became the preferred first-line therapy in 2018 and dramatically improved skeletal outcomes.
- Autosomal dominant hypophosphatemic rickets (ADHR) — caused by gain-of-function mutations in FGF23 itself that protect the hormone from proteolytic cleavage, prolonging its activity. The same end result: phosphaturia, low serum phosphate, rickets.
- Tumor-induced osteomalacia (TIO) — an acquired adult phosphate-wasting disorder driven by ectopic FGF23 production from a usually small, hard-to-find mesenchymal tumor (typically benign). The clinical picture is severe progressive bone pain, fractures, and muscle weakness in a previously well adult, with markedly elevated serum FGF23. Surgical resection of the tumor (when it can be localized, sometimes requiring 68-Ga-DOTATATE PET imaging) produces complete cure.
The pattern across all three: too much FGF23, too little serum phosphate, mineralization failure. Vitamin D treatment alone is insufficient or worsens hypercalciuria; the phosphate has to be restored.
Renal Osteodystrophy and CKD-MBD
Chronic kidney disease produces a complex bone and mineral disorder now called CKD-MBD (chronic kidney disease – mineral and bone disorder), with renal osteodystrophy as its skeletal manifestation. The pathophysiology starts as soon as the glomerular filtration rate (eGFR) falls below approximately 60 mL/min/1.73m2:
- Phosphate retention — impaired renal phosphate excretion causes serum phosphate to rise. Initially, FGF23 rises to compensate (driving the remaining nephrons to excrete more phosphate per unit filtered), but eventually the compensation fails and frank hyperphosphatemia develops.
- FGF23-driven suppression of active vitamin D — the chronically elevated FGF23 suppresses 1-alpha-hydroxylase in the proximal tubule, lowering 1,25-dihydroxyvitamin D and reducing intestinal calcium absorption.
- Hypocalcemia and secondary hyperparathyroidism — the low active vitamin D plus the high phosphate (which complexes with calcium) drops ionized calcium, triggering massive PTH secretion. Over years, the parathyroid glands hypertrophy, develop nodular hyperplasia, and become semi-autonomous (tertiary hyperparathyroidism), maintaining elevated PTH even after the original stimulus is corrected.
- Bone disease — the chronic high PTH drives a high-turnover bone disease (osteitis fibrosa cystica) with subperiosteal resorption, brown tumors, and increased fracture risk. Some patients develop the opposite picture of adynamic bone disease (low turnover from over-suppression of PTH by aggressive treatment), which is also fragility-prone. Either way, bone density falls and fracture risk rises.
- Vascular calcification — arguably the most lethal consequence. The chronic high serum phosphate, often combined with high calcium from supplementation and elevated PTH, drives massive deposition of hydroxyapatite in the medial layer of arteries (Mönckeberg sclerosis), accelerating cardiovascular disease and contributing substantially to the excess cardiovascular mortality of CKD patients on dialysis.
Modern management of CKD-MBD requires aggressive control of serum phosphate (dietary restriction plus oral phosphate binders — calcium acetate, sevelamer, lanthanum carbonate, ferric citrate), active vitamin D analog supplementation (calcitriol, paricalcitol), and PTH-lowering therapy (calcimimetics like cinacalcet that increase the calcium sensitivity of the parathyroid gland). For more on the underlying renal disease, see our Kidney Disease page.
The Hidden Phosphate Additives Problem
Warning — hidden phosphate additives in processed food. Inorganic phosphate salts (sodium phosphate, potassium phosphate, calcium phosphate, polyphosphates, hexametaphosphate, pyrophosphate) are added to a huge range of processed foods as preservatives, emulsifiers, leavening agents, color stabilizers, and moisture binders. The FDA classifies most as GRAS (generally recognized as safe) and the amounts added are not always declared in a way the consumer can see. Crucially, inorganic phosphate additives are absorbed at roughly 90 percent efficiency, compared with roughly 60 percent for organic phosphate naturally present in unprocessed food. Common offenders include processed meats and deli meats, processed cheeses and cheese-product spreads, dark cola drinks, baking powder, instant pudding mixes, non-dairy creamers, and many bottled and canned beverages.
For healthy adults with normal kidney function, modest additive intake is unlikely to cause acute harm but is associated in epidemiologic studies with vascular calcification, endothelial dysfunction, and elevated FGF23 over time. For adults with reduced kidney function — even early CKD that may not yet have been diagnosed — the additive burden is a major driver of the CKD-MBD cascade described above. The practical advice for any patient with CKD, hypertension, diabetes, or a strong family history of any of these is to read ingredient lists for any added "phosphate" or "phosphoric acid" and to favor whole foods.
Dark cola drinks are a particular cardiovascular and bone concern. Cola contains phosphoric acid as the acidulant that gives it its tart taste, contributing roughly 30 to 40 mg of inorganic phosphate per 12-oz can. Multiple cohort studies have linked heavy cola consumption to lower bone mineral density in adolescent girls and adult women, the mechanism most likely being a combination of the phosphate load, the cola displacing milk in the diet, and the caffeine contributing modest urinary calcium loss.
Clinical Applications and Monitoring
- Healthy adults — meet the calcium DRI (1,000–1,200 mg/day depending on age and sex), get adequate vitamin D, avoid excessive phosphate additives. No routine monitoring needed.
- Postmenopausal women and older adults at fracture risk — bone mineral density (DXA scan), vitamin D level, ensure adequate calcium and protein intake. Phosphorus is rarely the limiting nutrient.
- Vegan / dairy-free diets — deliberate calcium supplementation, vitamin D level monitoring, and vitamin K2 attention. Phosphorus is rarely deficient on plant-based diets.
- CKD stages 3–5 — serum phosphate, calcium, PTH, 25-hydroxyvitamin D, and (when indicated) FGF23 monitored periodically; dietary phosphate restriction; phosphate binders; active vitamin D analogs; calcimimetics in tertiary hyperparathyroidism.
- Suspected rickets or osteomalacia — serum calcium, phosphate, alkaline phosphatase, 25-OH-vitamin D, 1,25-OH2-vitamin D, PTH, and urinary phosphate. Low phosphate with inappropriately normal or elevated urinary phosphate excretion points to a phosphate-wasting syndrome (XLH, TIO); send for FGF23 if suspected.
- Suspected hypophosphatasia — strikingly low alkaline phosphatase in a patient with a rickets-like picture; genetic testing for ALPL mutations.
- Dental health — community water fluoridation, fluoride toothpaste, and dietary calcium and phosphorus all contribute. Children with dietary phosphate deficiency (rare in developed countries except in malabsorption syndromes) show enamel hypoplasia.
For laboratory interpretation, the serum phosphate is exquisitely time-of-day sensitive (lower in the morning, higher after carbohydrate-rich meals because of cellular uptake), so consistent fasting morning timing matters for serial monitoring. For interpretation of kidney function generally, see our eGFR page.
Key Research Papers
- Boskey AL (2013). Bone composition: relationship to bone fragility and antiosteoporotic drug effects. BoneKEy Reports. — PubMed
- Murshed M (2018). Mechanism of bone mineralization. Cold Spring Harbor Perspectives in Medicine. — PubMed
- Whyte MP (2010). Physiological role of alkaline phosphatase explored in hypophosphatasia. Annals of the NY Academy of Sciences. — PubMed
- Quarles LD (2012). Skeletal secretion of FGF-23 regulates phosphate and vitamin D metabolism. Nature Reviews Endocrinology. — PubMed
- Carpenter TO et al. (2018). Burosumab therapy in children with X-linked hypophosphatemia. NEJM. — PubMed
- Florenzano P et al. (2017). Tumor-induced osteomalacia. Calcified Tissue International. — PubMed
- KDIGO Clinical Practice Guideline for CKD-MBD (2017 Update). — PubMed
- Moe SM et al. (2006). Definition and classification of renal osteodystrophy and chronic kidney disease-mineral and bone disorder (CKD-MBD). Kidney International. — PubMed
- Calvo MS, Uribarri J (2013). Public health impact of dietary phosphorus excess on bone and cardiovascular health in the general population. American Journal of Clinical Nutrition. — PubMed
- Tucker KL et al. (2006). Colas, but not other carbonated beverages, are associated with low bone mineral density in older women: The Framingham Osteoporosis Study. American Journal of Clinical Nutrition. — PubMed
- Block GA et al. (2004). Mineral metabolism, mortality, and morbidity in maintenance hemodialysis. JASN. — PubMed
- Razzaque MS (2009). The FGF23-Klotho axis: endocrine regulation of phosphate homeostasis. Nature Reviews Endocrinology. — PubMed
PubMed Topic Searches
- PubMed: Hydroxyapatite and bone mineralization
- PubMed: Calcium-phosphorus ratio and bone
- PubMed: FGF23 phosphate regulation
- PubMed: CKD-MBD and renal osteodystrophy
- PubMed: XLH and burosumab
Connections
- Phosphorus Overview
- Phosphorus Benefits Hub
- Phosphorus for Energy Production
- Phosphorus for Cell Membranes
- Phosphorus for Acid-Base Balance
- Calcium
- Calcium and Bone Health
- Magnesium
- Vitamin D3
- Vitamin K (K2 for Bone)
- Osteoporosis
- Hyperparathyroidism
- Kidney Disease
- Cardiovascular Disease
- eGFR
- Collagen
- Eggs
- All Minerals