Manganese — Benefits Deep Dive
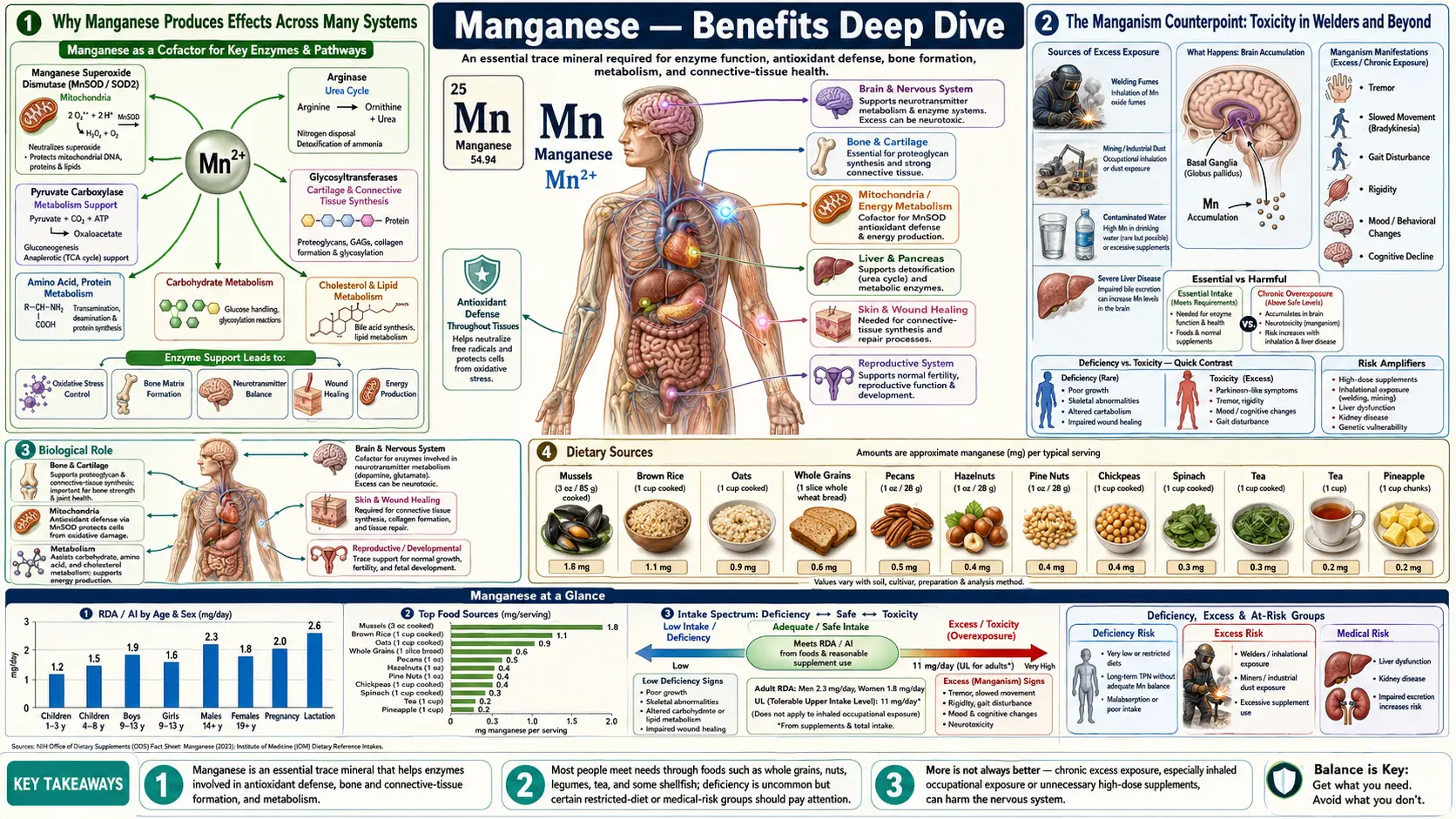
Manganese is the quiet workhorse of trace mineral biochemistry. The human body contains only 10-20 milligrams of it, yet it sits at the active site of four enzymes that are absolutely essential to life — the mitochondrial antioxidant MnSOD, the urea-cycle terminator arginase, the gluconeogenic gateway pyruvate carboxylase, and the brain's glutamate-recycling glutamine synthetase. Add in prolidase (collagen recycling) and the entire family of glycosyltransferases (proteoglycan assembly), and a single 2-milligram-per-day mineral turns out to be the cofactor for systems as diverse as mitochondrial defense, ammonia disposal, blood glucose regulation, neurotransmitter recycling, collagen turnover, and bone matrix assembly. Four benefit pages below explore the conditions where manganese produces the largest clinical effect — skeletal formation, antioxidant defense at the SOD2 level, wound healing through prolidase and glycosyltransferase action, and glucose metabolism through gluconeogenic enzyme support — and the counterpoint of manganism, the Parkinsonian neurotoxicity that defines the upper boundary of safe intake.
Deep-Dive Articles
Bone Formation
Manganese as the cofactor for glycosyltransferases that build chondroitin sulfate, keratan sulfate, and aggrecan in bone matrix; prolidase-mediated collagen recycling; MnSOD protection of osteoblasts; the Strause-Saltman 1994 trial showing trace-mineral plus calcium reduced postmenopausal spinal bone loss; perosis in poultry as the original deficiency syndrome; manganism as the upper safety boundary.
Antioxidant Mn-SOD (SOD2)
The mitochondrial antioxidant defender. Superoxide-to-hydrogen-peroxide dismutation chemistry at near-diffusion-limited rate. SOD2 knockout mouse mortality (8-day median lifespan from dilated cardiomyopathy and metabolic acidosis). The Val16Ala (rs4880) polymorphism and elevated risk of cardiomyopathy, doxorubicin cardiotoxicity, diabetic complications, and neurodegeneration. SIRT3 regulation via lysine acetylation, the link to caloric restriction and NAD+ status, and the mitochondrial theory of aging.
Wound Healing
Manganese-activated prolidase as the dipeptidase that recycles proline from degraded collagen for new collagen synthesis — the inherited disorder of prolidase deficiency causes severe non-healing skin ulcers, demonstrating the enzyme's essential role. Glycosyltransferase-built proteoglycan ground substance for fibroblast and keratinocyte migration. Chondrocyte function in cartilage repair. MnSOD containment of the inflammatory-phase oxidative burst. Application to diabetic foot ulcers, burns, surgical recovery, and pressure ulcers.
Blood Sugar & Glucose Metabolism
Manganese-dependent gluconeogenic enzymes pyruvate carboxylase (the entry point) and phosphoenolpyruvate carboxykinase (PEPCK). Manganese deficiency and impaired insulin response from human and rodent studies. The U-shaped relationship between blood manganese and type 2 diabetes risk (both low and high are bad). Manganese-magnesium interplay in glucose homeostasis. MnSOD and the Brownlee mitochondrial-superoxide model of diabetic complications.
Table of Contents
- Deep-Dive Articles
- Why Manganese Produces Effects Across Many Systems
- The Manganism Counterpoint: Toxicity in Welders and Beyond
- Research Papers: Bone Formation & Connective Tissue
- Research Papers: MnSOD Antioxidant Defense
- Research Papers: Wound Healing & Prolidase
- Research Papers: Blood Sugar & Gluconeogenesis
- Research Papers: Cross-Cutting (Toxicity, Status, Homeostasis)
- External Authoritative Resources
- Connections
- Featured Videos
Why Manganese Produces Effects Across Many Systems
Most trace minerals serve as cofactors for one or a few enzymes. Manganese is unusual because it is the active-site metal for an unusually diverse set of metalloenzymes, and the activating cofactor for a whole family of glycosyltransferases. The biochemistry maps onto five different physiologic systems, each producing a distinct category of clinical effect.
- Mitochondrial antioxidant defense (MnSOD / SOD2) — manganese is the active-site metal of the mitochondrial superoxide dismutase, the single most critical enzyme defending against the reactive oxygen species generated by oxidative phosphorylation. SOD2 knockout is neonatally lethal. The Val16Ala polymorphism reducing MnSOD mitochondrial import is associated with elevated risk of cardiomyopathy, diabetic complications, and neurodegeneration. See the antioxidant deep-dive.
- Urea cycle (arginase) — arginase is a manganese-containing metalloenzyme that catalyzes the final step of urea synthesis, hydrolyzing arginine to ornithine and urea. This is the body's principal nitrogen-disposal pathway. Inadequate manganese impairs ammonia detoxification, particularly during high-protein intake or amino acid catabolism.
- Gluconeogenesis (pyruvate carboxylase, PEPCK) — two of the four committed gluconeogenic enzymes are manganese-dependent: pyruvate carboxylase (entry point) and phosphoenolpyruvate carboxykinase (second step). These enzymes also serve TCA cycle anaplerosis, replenishing oxaloacetate that is drawn off for biosynthesis. Manganese deficiency impairs both glucose synthesis during fasting and oxidative ATP production. See the blood-sugar deep-dive.
- Neurotransmitter recycling (glutamine synthetase) — glutamine synthetase in astrocytes converts glutamate to glutamine for re-export to neurons, sustaining the glutamate-glutamine cycle essential for excitatory neurotransmission. The enzyme is manganese-dependent. Disruption (by either deficiency or, paradoxically, toxic excess) contributes to neurologic dysfunction.
- Connective tissue (prolidase + glycosyltransferases) — manganese activates prolidase for collagen recycling and the entire family of glycosyltransferases for proteoglycan assembly. These enzymes are critical for bone matrix, cartilage, skin, and wound healing. See the bone-formation and wound-healing deep-dives.
The therapeutic complication is that manganese has an unusually narrow therapeutic window. Inadequate intake produces measurable but rarely dramatic dysfunction across the five systems above. Excessive intake (especially inhalational exposure) produces dramatic Parkinsonian neurodegeneration. Most healthy adults consuming a varied diet are well within the therapeutic range and require no supplementation. Targeted supplementation in the 1-5 mg/day range is appropriate for specific situations (multi-mineral bone formulas, post-bariatric surgery, malabsorption syndromes). Aggressive supplementation beyond 11 mg/day from all sources is not warranted and may be harmful.
The Manganism Counterpoint: Toxicity in Welders and Beyond
No discussion of manganese benefits is complete without the counterpoint: manganese is a known neurotoxin, and chronic excess exposure produces a serious, often progressive, Parkinsonian disease called manganism. The condition was first described in 1837 by James Couper in workers grinding manganese dioxide and remains an active occupational health concern in the modern era.
- Occupational exposure populations — welders (especially MIG and TIG welding of manganese-containing steels), miners, steel workers, ferromanganese smelter workers, dry-cell battery manufacturers. The CDC and OSHA monitor occupational manganese exposure; permissible exposure limits are being progressively tightened as the evidence accumulates.
- Clinical syndrome — manganism develops insidiously over months to years of chronic inhalational exposure. Early symptoms include irritability, emotional lability, anorexia, and headache. Progression leads to bradykinesia, dystonia, postural instability, gait disorder (with characteristic "cock-walk"), and dysarthria. Later stages produce frank parkinsonism with rigidity, tremor, and cognitive decline. Unlike Parkinson's disease, manganism is largely unresponsive to levodopa therapy because the lesion is post-synaptic in the basal ganglia rather than the dopaminergic neuron loss of Parkinson's.
- Pathology — manganese accumulates selectively in the globus pallidus and other basal ganglia structures. The deposition is visible on T1-weighted brain MRI as hyperintensity in the globus pallidus, a finding useful for both diagnosis and detecting subclinical exposure in at-risk workers.
- Routes of high-risk exposure — inhalation (the dominant route, because olfactory uptake bypasses biliary excretion); contaminated drinking water (well water with manganese above EPA recommendations); long-term parenteral nutrition with manganese-containing formulas; hepatic insufficiency (cirrhosis or biliary obstruction impairs biliary excretion).
- Dietary intake is generally not a concern — the gastrointestinal absorption of manganese from food is tightly regulated (only 1-5% of dietary manganese is absorbed in adults with normal status), and the biliary excretion route handles any excess. Even relatively high dietary intake (10-15 mg/day from food) does not produce manganism in healthy individuals.
- Children are more vulnerable — infants and children absorb manganese at higher fractional rates and have less developed biliary excretion. Infant formulas (especially soy-based) provide much higher manganese than breast milk, and concerns have been raised about possible neurodevelopmental effects, though clinical evidence is limited.
- Treatment — primary intervention is removal from exposure. Chelation with EDTA or CaNa2EDTA has been used acutely but reverses symptoms only partially. Levodopa is largely ineffective. The neurologic damage tends to be permanent once established.
The clinical takeaway is to honor the therapeutic window. Dietary manganese from whole foods is safe and necessary. Targeted supplementation in the 1-5 mg/day range for specific indications is reasonable. Aggressive supplementation, supplementation in patients with liver disease, and any situation involving inhalational exposure deserve careful evaluation.
Research Papers: Bone Formation & Connective Tissue
- Strause L, Saltman P, Smith KT et al. (1994). Spinal bone loss in postmenopausal women supplemented with calcium and trace minerals. Journal of Nutrition 124(7):1060-1064. — PubMed
- Saltman PD, Strause LG (1993). The role of trace minerals in osteoporosis. Journal of the American College of Nutrition 12(4):384-389. — PubMed
- Leach RM Jr (1971). Role of manganese in mucopolysaccharide metabolism. Federation Proceedings. — PubMed
- Leach RM, Muenster AM, Wien EM (1969). Studies on the role of manganese in bone formation: chondroitin sulfate synthesis in chick epiphyseal cartilage. Archives of Biochemistry and Biophysics. — PubMed
- Hurley LS, Keen CL (1987). Manganese. In: Trace Elements in Human and Animal Nutrition. — PubMed
- Palacios C (2006). The role of nutrients in bone health, from A to Z. Critical Reviews in Food Science and Nutrition. — PubMed
- Norris LC, Heuser GF (1936). The role of manganese in poultry nutrition (perosis). Cornell University Agricultural Experiment Station. — PubMed
- Freeland-Graves JH, Lin PH (1991). Plasma uptake of manganese affected by oral loads. Journal of the American College of Nutrition. — PubMed
- Hurley LS (1981). Teratogenic aspects of manganese, zinc, and copper nutrition. Physiological Reviews. — PubMed
- Aschner JL, Aschner M (2005). Nutritional aspects of manganese homeostasis. Molecular Aspects of Medicine. — PubMed
Research Papers: MnSOD Antioxidant Defense
- Li Y et al. (1995). Dilated cardiomyopathy and neonatal lethality in mutant mice lacking manganese superoxide dismutase. Nature Genetics. — PubMed
- Lebovitz RM et al. (1996). Neurodegeneration, myocardial injury, and perinatal death in mitochondrial superoxide dismutase-deficient mice. PNAS. — PubMed
- Sutton A et al. (2003). The Ala16Val genetic dimorphism modulates the import of human MnSOD into rat liver mitochondria. Pharmacogenetics. — PubMed
- Qiu X et al. (2010). Calorie restriction reduces oxidative stress by SIRT3-mediated SOD2 activation. Cell Metabolism. — PubMed
- Tao R et al. (2010). Sirt3-mediated deacetylation of lysine 122 regulates MnSOD activity. Molecular Cell. — PubMed
- Bresciani G et al. (2015). Manganese superoxide dismutase and oxidative stress modulation. Advances in Clinical Chemistry. — PubMed
- Bag A, Bag N (2008). MnSOD target sequence polymorphism and cancer risk. Cancer Epidemiol Biomarkers Prev. — PubMed
- Wang Y et al. (2017). Superoxide dismutases: dual roles in controlling ROS damage and regulating ROS signaling. Journal of Cell Biology. — PubMed
- Harman D (1956). Aging: a theory based on free radical and radiation chemistry. Journal of Gerontology. — PubMed
- Mohammedi K et al. (2015). MnSOD polymorphisms and risk of nephropathy in type 1 diabetes. Free Radic Biol Med. — PubMed
Research Papers: Wound Healing & Prolidase
- Lupi A, Tenni R, Rossi A, Cetta G, Forlino A (2008). Human prolidase and prolidase deficiency. Amino Acids. — PubMed
- Kitchener RL, Grunden AM (2012). Prolidase function in proline metabolism and its medical applications. Journal of Applied Microbiology. — PubMed
- Phang JM, Liu W (2012). Proline metabolism and cancer. Frontiers in Bioscience. — PubMed
- Heyland DK et al. (2005). Antioxidant nutrients in the critically ill: systematic review. Intensive Care Medicine. — PubMed
- Berger MM, Shenkin A (2007). Trace element requirements in critically ill burned patients. Journal of Trace Elements in Medicine and Biology. — PubMed
- Stechmiller JK (2010). Understanding the role of nutrition and wound healing. Nutrition in Clinical Practice. — PubMed
- Posthauer ME et al. (2015). Pressure ulcer nutrition: NPUAP/EPUAP/PPPIA white paper. Advances in Skin & Wound Care. — PubMed
- Powell GF, Maniscalco RM (1976). Bound hydroxyproline excretion in prolidase deficiency. Metabolism. — PubMed
- Reiber GE et al. (1999). Causal pathways for diabetic foot ulcers. Diabetes Care. — PubMed
- Lupi A et al. (2008). Recombinant human prolidase expression systems. Biotechnology and Applied Biochemistry. — PubMed
Research Papers: Blood Sugar & Gluconeogenesis
- Brownlee M (2005). The pathobiology of diabetic complications: a unifying mechanism. Diabetes. — PubMed
- Koh ES et al. (2014). Serum manganese and risk of metabolic syndrome and type 2 diabetes in Korean adults. Biological Trace Element Research. — PubMed
- Du S et al. (2020). Association between blood manganese and type 2 diabetes: meta-analysis. Journal of Trace Elements in Medicine and Biology. — PubMed
- Walter RM et al. (1991). Copper, zinc, manganese, magnesium status and diabetic complications. Diabetes Care. — PubMed
- Hambidge KM et al. (1986). Trace elements including manganese deficiency. Trace Elements in Human and Animal Nutrition. — PubMed
- Yang BY et al. (2020). Dietary manganese intake and diabetes/prediabetes in Chinese adults. Frontiers in Nutrition. — PubMed
- Jomova K, Valko M (2011). Advances in metal-induced oxidative stress and human disease. Toxicology. — PubMed
- Liu L et al. (2017). Blood and urinary manganese in type 2 diabetes. Journal of Diabetes. — PubMed
- Rorsman P, Ashcroft FM (2018). Pancreatic beta-cell electrical activity and insulin secretion. Physiological Reviews. — PubMed
- Burch HB et al. (1975). Pyruvate carboxylase deficiency clinical syndrome. Journal of Pediatrics. — PubMed
Research Papers: Cross-Cutting (Toxicity, Status, Homeostasis)
- Aschner JL, Aschner M (2005). Nutritional aspects of manganese homeostasis. Molecular Aspects of Medicine. — PubMed
- Horning KJ, Caito SW, Tipps KG, Bowman AB, Aschner M (2015). Manganese is essential for neuronal health. Annual Review of Nutrition. — PubMed
- Finley JW, Davis CD (1999). Manganese deficiency and toxicity: cause for concern? BioFactors. — PubMed
- Couper J (1837). Sur les effets du peroxide de manganese (first description of manganism). Journal de Chimie Médicale. — PubMed
- Olanow CW (2004). Manganese-induced parkinsonism and Parkinson's disease. Annals of the New York Academy of Sciences. — PubMed
- Lucchini RG, Martin CJ, Doney BC (2009). From manganism to manganese-induced parkinsonism: a conceptual model. NeuroMolecular Medicine. — PubMed
- Bowman AB et al. (2011). Role of manganese in neurodegenerative diseases. Journal of Trace Elements in Medicine and Biology. — PubMed
- Roth JA (2006). Homeostatic and toxic mechanisms regulating manganese uptake, retention, and elimination. Biological Research. — PubMed
- Greger JL (1999). Nutrition versus toxicology of manganese in humans. Neurotoxicology. — PubMed
- Institute of Medicine (2001). Dietary Reference Intakes for vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc. National Academy Press. — PubMed
External Authoritative Resources
- Linus Pauling Institute — Manganese Micronutrient Information Center — the most authoritative open-access scientific review of manganese biology, regularly updated
- NIH Office of Dietary Supplements — Manganese Fact Sheet (Health Professionals)
- ATSDR — Toxicological Profile for Manganese (CDC document on occupational and environmental exposure)
- OSHA — Manganese Compounds occupational exposure guidance
- MedlinePlus — Manganese
- PubMed — All research on manganese in human nutrition
Connections
- Manganese (Main Page)
- Manganese for Bone Formation
- Manganese MnSOD Antioxidant Defense
- Manganese for Wound Healing
- Manganese for Blood Sugar
- All Minerals
- Magnesium
- Calcium
- Calcium and Bone Health
- Zinc
- Copper
- Selenium
- Chromium
- Boron
- Silicon
- Phosphorus
- Vitamin D3
- Vitamin K2
- Vitamin C
- Osteoporosis
- Arthritis
- Parkinson's Disease
- Type 2 Diabetes
- Metabolic Syndrome
- Collagen
- Proline
- Oxidative Stress
- Copper-Iron Dysregulation
- Spinach
- Brown Rice