Manganese for Antioxidant Defense (MnSOD/SOD2)
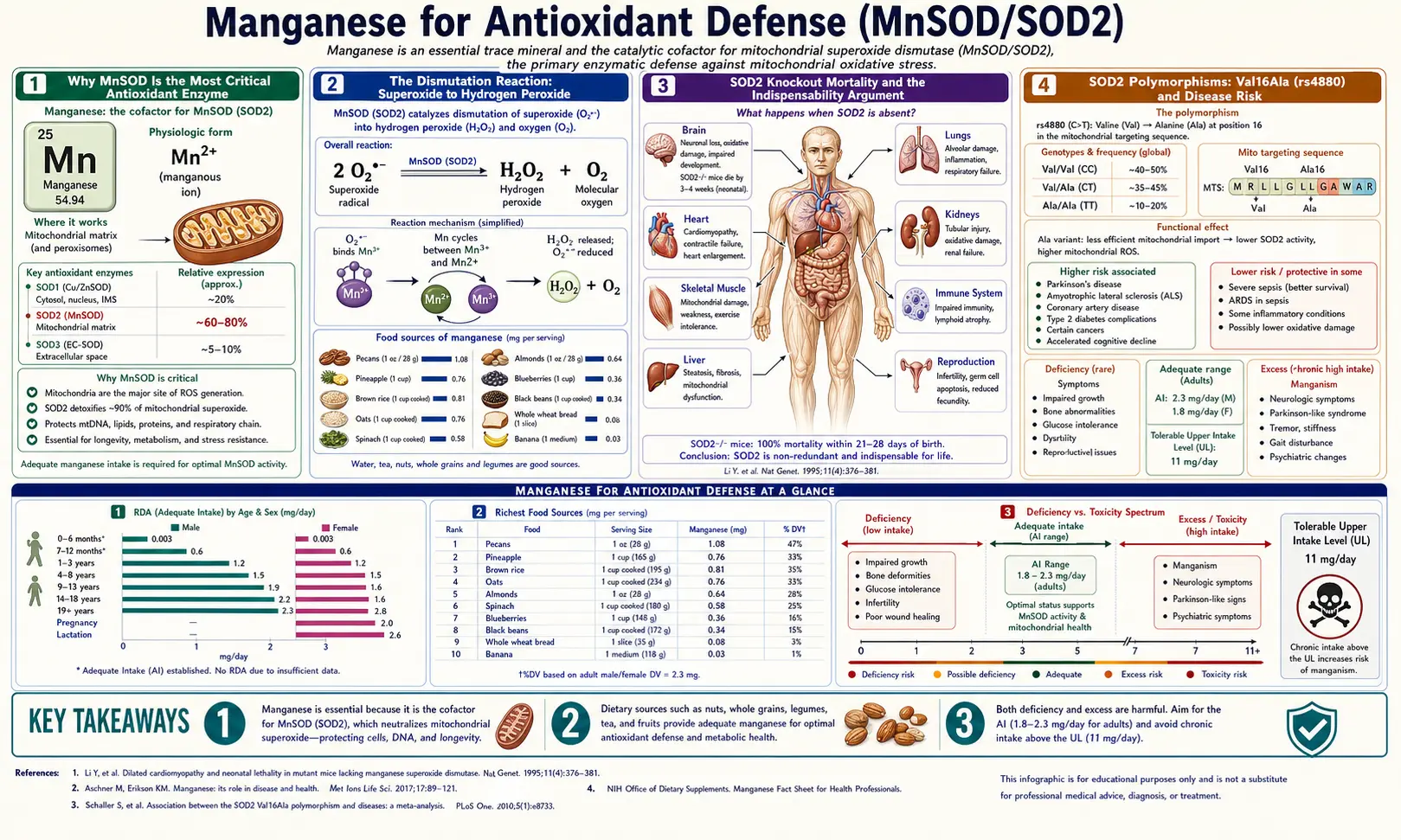
Manganese superoxide dismutase (MnSOD, also called SOD2) is the single most important antioxidant enzyme in the human body. Located exclusively in the mitochondrial matrix where 90% of cellular reactive oxygen species are generated, MnSOD catalyzes the dismutation of superoxide radicals into hydrogen peroxide and oxygen — the first and most critical step in mitochondrial antioxidant defense. The enzyme's importance is most starkly demonstrated by genetic knockout: SOD2-null mice die within 1-3 weeks of birth from dilated cardiomyopathy, neurodegeneration, and metabolic acidosis. Common human polymorphisms (notably Val16Ala, also called rs4880) that reduce MnSOD mitochondrial targeting are linked to elevated risk of cardiomyopathy, neurodegeneration, several cancers, and accelerated aging. Adequate manganese is the dietary input that keeps this critical defense system running.
Table of Contents
- Why MnSOD Is the Most Critical Antioxidant Enzyme
- The Dismutation Reaction: Superoxide to Hydrogen Peroxide
- SOD2 Knockout Mortality and the Indispensability Argument
- SOD2 Polymorphisms: Val16Ala (rs4880) and Disease Risk
- SIRT3 Regulation of MnSOD Activity (Acetylation Code)
- Oxidative Stress in Aging and the Mitochondrial Theory
- Disease Associations: Cancer, Neurodegeneration, Cardiomyopathy
- Assessing MnSOD Activity and Manganese Status
- Practical Interventions: Diet, Lifestyle, Drug Considerations
- Key Research Papers
- Connections
- Featured Videos
Why MnSOD Is the Most Critical Antioxidant Enzyme
The cell contains a layered antioxidant defense system. The first tier consists of three superoxide dismutases — SOD1 (CuZnSOD) in cytoplasm, SOD2 (MnSOD) in mitochondrial matrix, and SOD3 (extracellular CuZnSOD) in the extracellular space. The second tier consists of catalase (peroxisomes) and the glutathione peroxidase / glutathione reductase system. The third tier includes small-molecule antioxidants like ascorbate (vitamin C), alpha-tocopherol (vitamin E), glutathione, and ubiquinol (coenzyme Q10).
Of all these defenders, MnSOD has the strongest claim to being most critical for these reasons:
- Location — mitochondria generate the overwhelming majority (estimates range from 80–95%) of cellular reactive oxygen species. Electron leakage from complexes I and III of the electron transport chain produces superoxide directly into the mitochondrial matrix, and MnSOD is the only superoxide dismutase positioned to intercept it there.
- Substrate — superoxide is the parent reactive oxygen species. Most other ROS (hydrogen peroxide, hydroxyl radical, peroxynitrite) are downstream products. Stopping the cascade at superoxide is more efficient than mopping up the downstream radicals afterward.
- Knockout phenotype — SOD2-null mice die within 1-3 weeks of birth. SOD1-null mice live normally with only modest motor deficits late in life. SOD3-null mice are viable. The differential phenotype is dramatic evidence of MnSOD's unique indispensability.
- Conservation — MnSOD is one of the most evolutionarily ancient enzymes in life, present in essentially all aerobic organisms from bacteria to humans, with the active-site manganese and overall protein fold conserved across two billion years.
This is why manganese, despite being needed only at trace levels, is non-negotiable. The body has no substitute for MnSOD at its post.
The Dismutation Reaction: Superoxide to Hydrogen Peroxide
The MnSOD-catalyzed reaction is a two-step dismutation in which two superoxide radicals are converted to one molecule of hydrogen peroxide and one molecule of molecular oxygen:
Step 1: Mn(III) + O2·− → Mn(II) + O2
Step 2: Mn(II) + O2·− + 2H+ → Mn(III) + H2O2
Net: 2 O2·− + 2H+ → H2O2 + O2
The reaction is essentially diffusion-limited, meaning it proceeds as fast as the superoxide substrate can encounter the enzyme — one of the fastest known enzymatic reactions, with a turnover rate of approximately 109 per second. This extraordinary speed is necessary because superoxide, while a relatively mild radical itself, rapidly reacts with nitric oxide to produce peroxynitrite (an extremely damaging species) and with iron-sulfur clusters in enzymes like aconitase to inactivate them and release reactive iron.
The hydrogen peroxide product is then converted to water by glutathione peroxidase (using glutathione as electron donor) or by catalase in peroxisomes. If either downstream enzyme is impaired (low glutathione, low selenium, low catalase), hydrogen peroxide accumulates and can be converted via Fenton chemistry to hydroxyl radical, the most damaging ROS species. This is why MnSOD never functions in isolation — it is the entry point of an integrated relay.
Each MnSOD subunit contains one manganese ion at its active site, coordinated by three histidines, one aspartate, and one water molecule. The manganese cycles between Mn(III) and Mn(II) oxidation states during catalysis. The mature human MnSOD is a homotetramer (four identical subunits), with each subunit carrying one manganese ion, giving the assembled enzyme four active sites.
SOD2 Knockout Mortality and the Indispensability Argument
The most direct evidence for MnSOD's critical role comes from genetic knockout experiments in mice. The original SOD2-null mouse was reported by Li and colleagues in Nature Genetics in 1995, with two independent confirmations from other groups within a few years.
The phenotype is severe and rapid:
- Mean lifespan: 8 days (depending on strain, range 1-21 days)
- Dilated cardiomyopathy — the heart, with its high mitochondrial density and continuous workload, is the first organ to fail. Histology shows myocyte vacuolization and contraction-band necrosis.
- Hepatic steatosis with mitochondrial damage — the liver shows fat accumulation and severely impaired mitochondrial respiration
- Metabolic acidosis — defective TCA cycle function (because superoxide inactivates aconitase) blocks oxidative ATP synthesis, forcing reliance on anaerobic glycolysis with lactate accumulation
- Neurodegeneration — spongiform encephalopathy with neuronal vacuolization, particularly in the basal ganglia and cerebellum
- Antioxidant rescue — treatment with manganese porphyrin SOD mimetics (MnTBAP and related compounds) partially rescues the phenotype, extending median lifespan to 16-19 days and reducing the cardiomyopathy. This pharmacologic rescue confirms that the lethal lesion is specifically loss of dismutase activity, not some other unrelated function of the SOD2 protein.
The heterozygous knockout (SOD2+/-, one functional copy) is viable and externally normal but shows increased mitochondrial DNA damage, accelerated cellular senescence in cultured fibroblasts, increased incidence of lymphoma with age, and reduced exercise capacity. This phenotype mirrors what is seen in humans with the lower-activity Ala16 allele of the Val16Ala polymorphism, discussed below.
SOD2 Polymorphisms: Val16Ala (rs4880) and Disease Risk
The most-studied polymorphism in the SOD2 gene is a single-nucleotide change at position 47 (C→T) that alters codon 16 in the mitochondrial targeting sequence from valine to alanine (Val16Ala, dbSNP rs4880). The polymorphism does not affect the enzyme's catalytic activity per se, but it affects how efficiently the newly translated MnSOD precursor protein is imported into mitochondria and processed into its mature form.
- Val/Val genotype — the ancestral allele; the precursor protein folds into an alpha-helix that is efficiently recognized by the mitochondrial import machinery. The mature MnSOD reaches the mitochondrial matrix at full concentration.
- Ala/Ala genotype — the Ala16 variant disrupts the alpha-helix in the targeting sequence, reducing efficiency of mitochondrial import. The result is approximately 30–40% less mature MnSOD in the mitochondrial matrix, with a corresponding portion of the precursor protein degraded or mislocalized in the cytosol.
- Val/Ala heterozygotes — intermediate phenotype, typically around 70% of the homozygous Val/Val MnSOD activity.
Population frequencies vary by ancestry: in European populations, Val and Ala alleles are roughly balanced (each about 50%); in East Asian populations, the Val allele is more common (about 85%); in African populations, the Ala allele predominates.
Epidemiologic associations of the Ala/Ala (lower-activity) genotype have included:
- Idiopathic cardiomyopathy — elevated risk of dilated cardiomyopathy and earlier onset of heart failure
- Doxorubicin cardiotoxicity — oncology patients with the Ala/Ala genotype have significantly higher risk of cardiotoxicity from anthracycline chemotherapy, which acts in part through mitochondrial superoxide generation
- Diabetic complications — elevated risk of nephropathy and retinopathy in type 1 and type 2 diabetes, attributed to greater mitochondrial oxidative damage from hyperglycemia
- Several cancers — mixed and contested literature, with some studies suggesting elevated risk of breast, prostate, and lung cancer in Ala/Ala carriers, though others have not replicated
- Neurodegenerative disease — modest but consistent associations with Parkinson's disease and amyotrophic lateral sclerosis risk
- Longevity — Val/Val homozygotes are overrepresented in centenarian populations in some cohorts, consistent with a small but cumulative protective effect across the lifespan
The Ala/Ala genotype is not a disease in itself, but it is a "loaded gun" — individuals carrying it are more vulnerable to any insult that increases mitochondrial superoxide production (chemotherapy, hyperglycemia, ischemia-reperfusion, prolonged inflammation). Genetic testing for rs4880 is widely available through consumer genomics platforms, and the Val/Ala status is one of the more actionable single-nucleotide variants for personalizing antioxidant strategy.
SIRT3 Regulation of MnSOD Activity (Acetylation Code)
One of the most important regulatory discoveries of the past decade has been that MnSOD activity is controlled post-translationally by acetylation, and the principal deacetylase is SIRT3 — the mitochondrial member of the sirtuin family of NAD+-dependent deacetylases.
MnSOD can be acetylated at lysines 53, 68, and 122. Acetylation at these sites reduces enzymatic activity. SIRT3 removes the acetyl groups, restoring full activity. The result is that MnSOD function is dynamically linked to cellular NAD+ status:
- High NAD+ (fasting, caloric restriction, exercise) — SIRT3 is highly active, MnSOD is largely deacetylated and at maximum activity, mitochondrial antioxidant defense is upregulated
- Low NAD+ (overfeeding, sedentary lifestyle, aging) — SIRT3 activity falls, MnSOD becomes increasingly acetylated, antioxidant defense capacity drops at exactly the time when oxidative challenge is rising
This regulatory circuit ties MnSOD to the broader sirtuin-NAD+-mitohormesis network that underlies many of the documented benefits of caloric restriction, intermittent fasting, and aerobic exercise. The interventions that boost SIRT3 activity (caloric restriction, exercise, NAD+ precursor supplementation like nicotinamide riboside or nicotinamide mononucleotide) all converge on enhanced MnSOD function as one of their downstream effects.
For the broader mitochondrial-antioxidant context, see our Oxidative Stress page and the discussion of mitohormesis interventions.
Oxidative Stress in Aging and the Mitochondrial Theory
The mitochondrial free radical theory of aging, first proposed by Denham Harman in 1956 and refined over the following decades, holds that cumulative oxidative damage to mitochondrial DNA, proteins, and membranes is a primary driver of cellular aging. MnSOD is the central enzyme that determines how much of this damage accumulates over a lifetime.
Lines of evidence supporting MnSOD's role in aging:
- SOD2 expression declines with age in most tissues studied (heart, brain, kidney), and the decline is more pronounced in tissues that show greatest age-related dysfunction
- SIRT3 expression also declines with age, doubling the hit on MnSOD activity (less enzyme, and what enzyme remains is less active because of acetylation accumulation)
- SOD2 overexpression in flies and worms extends lifespan — in Drosophila, MnSOD overexpression specifically in the nervous system extends lifespan by 30-50%
- Mitochondrially targeted antioxidants extend lifespan — compounds like MitoQ and SS-31 that concentrate in the mitochondrial matrix extend healthspan in animal models, supporting the broader paradigm
- Centenarians show preserved MnSOD function — comparative studies of centenarians vs population norms have found higher MnSOD activity in centenarian fibroblasts and lymphocytes, even after accounting for genotype
- Mitochondrial heteroplasmy — mitochondrial DNA damage accumulates with age, and tissues with high MnSOD activity show slower accumulation
The therapeutic implication is that anything supporting MnSOD function (adequate manganese, SIRT3 activation, NAD+ adequacy, regular aerobic exercise, periodic caloric restriction) should have additive benefit. None of these is a magic bullet individually, but they converge on the same mitochondrial defense system.
Disease Associations: Cancer, Neurodegeneration, Cardiomyopathy
Reduced MnSOD function (whether genetic, regulatory, or nutritional) has been linked to several major disease categories:
- Cancer — the MnSOD-cancer relationship is complex. In many cancers, MnSOD is paradoxically upregulated as the tumor adapts to its high metabolic and oxidative load, and high tumor MnSOD expression correlates with chemotherapy resistance and poor prognosis. In the surrounding stroma and normal tissues, however, low MnSOD activity is permissive for initial transformation. The therapeutic implication is bidirectional: support MnSOD in normal tissues for chemoprevention; inhibit it in established tumors for sensitization. Several MnSOD-targeting drugs are in development as cancer adjuvants.
- Cardiomyopathy and heart failure — the heart has among the highest mitochondrial density of any tissue, and MnSOD is essential for myocyte survival. SOD2 polymorphisms and acquired MnSOD deficiency are associated with cardiomyopathy, particularly idiopathic dilated cardiomyopathy, doxorubicin cardiotoxicity, and ischemia-reperfusion injury after myocardial infarction.
- Neurodegenerative disease — Parkinson's disease, amyotrophic lateral sclerosis, and Alzheimer's disease all show evidence of mitochondrial dysfunction and oxidative damage as core pathologic features. Reduced MnSOD activity is documented in affected brain regions in postmortem studies. Selective neuronal vulnerability (substantia nigra dopaminergic neurons in Parkinson's, motor neurons in ALS) may relate in part to differential MnSOD expression and capacity to handle endogenous oxidative stress.
- Diabetic complications — hyperglycemia accelerates mitochondrial superoxide production in vascular endothelium, retina, and renal tubular cells. The Brownlee unifying hypothesis of diabetic complications places this superoxide overproduction at the apex of the pathologic cascade leading to nephropathy, retinopathy, and neuropathy. Adequate MnSOD function would buffer this insult.
- Sepsis and critical illness — mitochondrial dysfunction is a central feature of severe sepsis. MnSOD activity is typically reduced in muscle biopsies from septic patients, contributing to the syndrome of "mitochondrial sepsis" and post-ICU weakness.
Assessing MnSOD Activity and Manganese Status
Direct measurement of MnSOD activity is technically possible but not routinely available. Practical assessment of manganese-and-MnSOD status uses several proxies:
- Whole blood manganese — the most useful single test, reflecting longer-term tissue manganese status better than serum or plasma. Reference range approximately 4-15 µg/L. Available through major reference laboratories.
- Serum manganese — less reliable than whole blood because manganese is concentrated in cells. Useful for diagnosing toxicity but limited for deficiency assessment.
- Erythrocyte SOD activity — can be measured directly from a blood draw. Reduced activity is suggestive of inadequate manganese (or copper/zinc for SOD1).
- Markers of oxidative damage — urinary 8-hydroxy-2-deoxyguanosine (8-OHdG, oxidative DNA damage marker), serum F2-isoprostanes (lipid peroxidation marker), and protein carbonyls all rise when MnSOD function is inadequate. These are sensitive but non-specific.
- SOD2 genotyping (rs4880) — available through consumer genomics services. Knowing your Val/Ala status helps personalize the case for aggressive MnSOD support.
- Functional symptoms — while not specific, fatigue, exercise intolerance, slow recovery from physical or oxidative stress, and accelerated visible aging are loosely associated with chronic suboptimal mitochondrial function and worth investigating in conjunction with the biomarkers above.
Practical Interventions: Diet, Lifestyle, Drug Considerations
- Maintain adequate dietary manganese — 1.8-2.3 mg/day from whole grains, nuts, legumes, leafy greens, and tea. Most varied diets supply this without difficulty. Supplementation in the 1-5 mg/day range is reasonable if intake is unclear; do not exceed 11 mg/day from all sources.
- Support SIRT3 activity — the regulatory partner that determines how much of your MnSOD is active. Interventions: regular aerobic exercise, intermittent caloric restriction or time-restricted eating, adequate NAD+ precursor intake (niacin, nicotinamide, or NMN/NR supplementation), and limiting overfeeding.
- Avoid the depletors — chronic alcohol abuse depletes mitochondrial NAD+, reducing SIRT3 activity. Chronic high-dose iron supplementation can compete with manganese for the DMT1 transporter and reduce manganese uptake. Sedentary lifestyle reduces mitochondrial biogenesis and MnSOD expression.
- Doxorubicin oncology patients — the SOD2 Val16Ala genotype meaningfully predicts cardiotoxicity risk. Ala/Ala patients warrant aggressive cardioprotective strategies (dexrazoxane consideration, intensive echocardiographic surveillance, judicious cumulative dose limits).
- Diabetes — the mitochondrial-superoxide-overproduction model of diabetic complications puts MnSOD support at the heart of long-term complication prevention. Excellent glycemic control reduces the substrate (superoxide) load on MnSOD.
- Neurodegenerative-risk individuals — family history of Parkinson's, ALS, or early-onset Alzheimer's may justify proactive MnSOD support through the full menu of interventions above. The evidence for any single intervention preventing these diseases is incomplete, but the mechanistic case for keeping mitochondrial defenses strong is solid.
- Athletes — chronic high-intensity training increases mitochondrial biogenesis and MnSOD expression as part of training adaptation. This is generally beneficial, but acute overtraining can transiently exceed antioxidant capacity. Adequate recovery, dietary antioxidants, and avoiding excessive antioxidant supplementation (which can blunt training adaptation) is the balanced approach.
This content is provided for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before starting any supplementation regimen.
Key Research Papers
- Li Y et al. (1995). Dilated cardiomyopathy and neonatal lethality in mutant mice lacking manganese superoxide dismutase. Nature Genetics 11(4):376-381. — PubMed
- Lebovitz RM et al. (1996). Neurodegeneration, myocardial injury, and perinatal death in mitochondrial superoxide dismutase-deficient mice. PNAS 93(18):9782-9787. — PubMed
- Sutton A et al. (2003). The Ala16Val genetic dimorphism modulates the import of human manganese superoxide dismutase into rat liver mitochondria. Pharmacogenetics 13(3):145-157. — PubMed
- Qiu X et al. (2010). Calorie restriction reduces oxidative stress by SIRT3-mediated SOD2 activation. Cell Metabolism 12(6):662-667. — PubMed
- Tao R et al. (2010). Sirt3-mediated deacetylation of evolutionarily conserved lysine 122 regulates MnSOD activity in response to stress. Molecular Cell 40(6):893-904. — PubMed
- Bresciani G et al. (2015). Manganese superoxide dismutase and oxidative stress modulation. Advances in Clinical Chemistry 68:87-130. — PubMed
- Bag A, Bag N (2008). Target sequence polymorphism of human manganese superoxide dismutase gene and its association with cancer risk: a review. Cancer Epidemiol Biomarkers Prev 17(12):3298-3305. — PubMed
- Wang Y et al. (2017). Superoxide dismutases: dual roles in controlling ROS damage and regulating ROS signaling. Journal of Cell Biology 217(6):1915-1928. — PubMed
- Pessoa Rodrigues C et al. (2021). SOD2 (Mn-SOD) and the cancer-promoting effects of mitochondrial reactive oxygen species. Cellular Signalling. — PubMed
- Harman D (1956). Aging: a theory based on free radical and radiation chemistry. Journal of Gerontology 11(3):298-300. (Original mitochondrial free radical theory of aging.) — PubMed
- Hori A et al. (2002). Association of SOD2 polymorphisms with risk of doxorubicin cardiotoxicity. Pharmacogenetics. — PubMed
- Mohammedi K et al. (2015). Manganese superoxide dismutase (SOD2) polymorphisms, plasma advanced oxidation protein products and risk of nephropathy in type 1 diabetes. Free Radic Biol Med. — PubMed
PubMed Topic Searches
- PubMed: MnSOD/SOD2 + mitochondria
- PubMed: SOD2 Val16Ala (rs4880)
- PubMed: SIRT3 deacetylation of MnSOD
- PubMed: Mitochondrial oxidative stress + aging
- PubMed: SOD + neurodegeneration
Connections
- Manganese Overview
- Manganese Benefits Hub
- Manganese for Bone Formation
- Manganese for Wound Healing
- Manganese for Blood Sugar
- Oxidative Stress
- Zinc (CuZnSOD Partner)
- Copper (CuZnSOD Partner)
- Selenium (Glutathione Peroxidase Cofactor)
- Vitamin E
- Vitamin C
- Coenzyme Q10
- Parkinson's Disease
- Cardiomyopathy
- Oncology (Cancer)
- Type 2 Diabetes
- Copper-Iron Dysregulation
- All Minerals