Hypomagnesemia (Low Magnesium): Symptoms, Causes, and Recovery
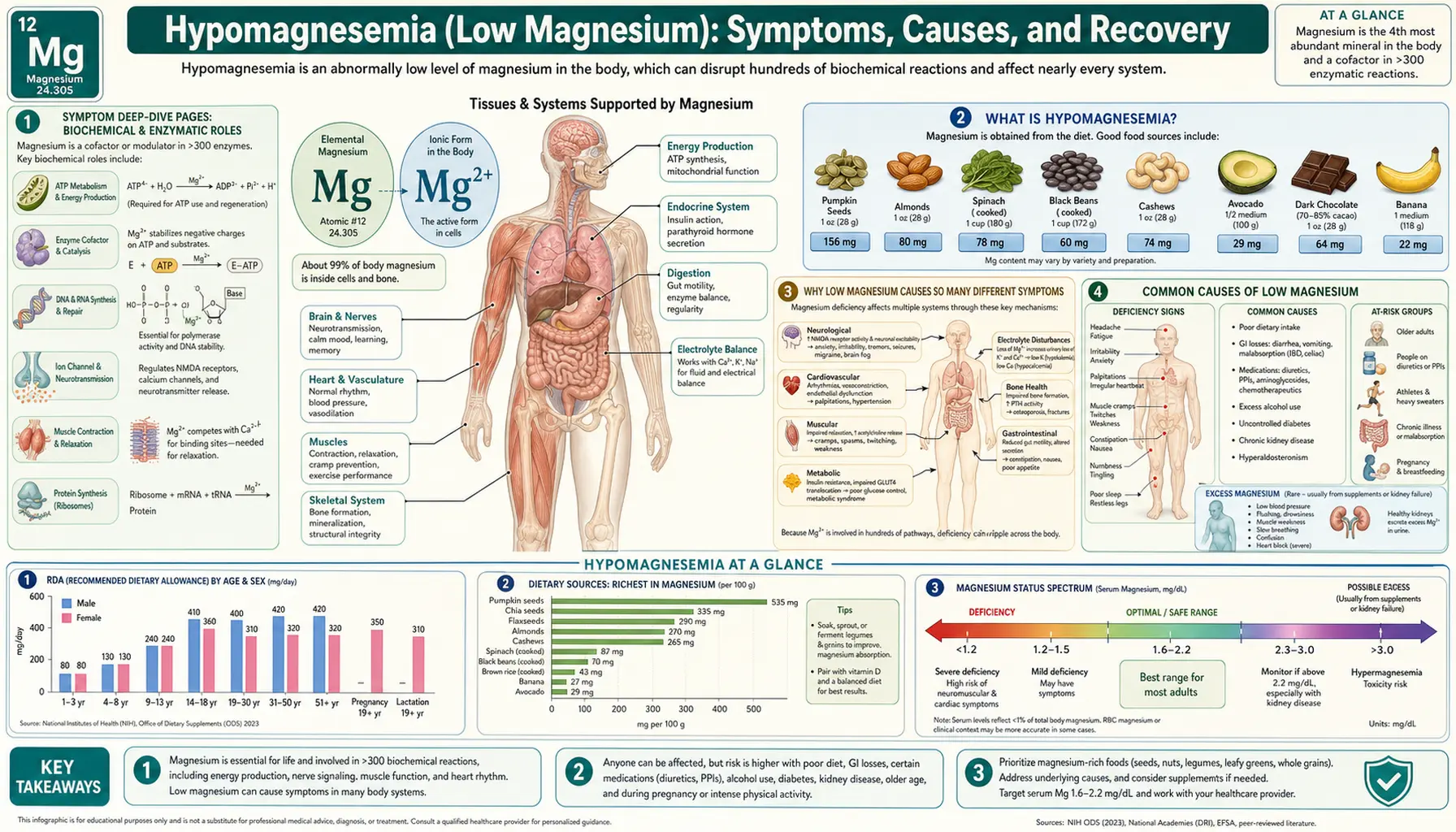
Hypomagnesemia is the medical term for low magnesium in the blood — usually a serum level below 1.7 mg/dL (about 0.7 mmol/L), where the normal range runs from roughly 1.7 to 2.2 mg/dL. It is one of the quietest of the common mineral shortages, and that is exactly what makes it tricky: muscle cramps and eyelid twitches, a fluttering or skipping heartbeat, anxiety and restless nights, and a stubborn, foggy fatigue can all trace back to the same low mineral, yet a routine blood test rarely measures it unless someone thinks to ask. The reason one shortage causes such scattered trouble is that magnesium is a quiet helper inside hundreds of the body's enzymes — it steadies the electrical charge of nerve and muscle cells, partners with calcium and potassium, and even helps your cells use their own energy currency, ATP. When it runs low, many systems feel it at once. The encouraging news is that, for most people, low magnesium is gentle to correct: more magnesium-rich whole foods, sometimes a well-chosen supplement, and almost always a look at potassium and calcium, the partner minerals that move with it. This hub explains what hypomagnesemia is, why one shortage causes so many different symptoms, what commonly drains it, and exactly how it is diagnosed and corrected — with deep-dive pages for each of the major symptoms.
Symptom Deep-Dive Pages
Muscle Cramps & Twitches
The classic calf cramps, eyelid flutters, and small muscle twitches (fasciculations) that appear when magnesium runs low — what they feel like, why under-supplied muscles become electrically jumpy, and what actually helps.
Heart Palpitations
Why low magnesium can make the heart feel like it is fluttering, pounding, or skipping beats, how it raises the risk of true arrhythmias, and when palpitations are a reason to be checked promptly.
Anxiety & Insomnia
How a shortage of this calming mineral can leave the nervous system on edge — wired, anxious, and unable to settle into sleep — and what the trials actually show about magnesium for stress and rest.
Fatigue & Headaches
Why low magnesium drains energy at the level of the cell's own batteries and is a recognized contributor to migraine and tension headaches — plus how it overlaps with other common causes of tiredness.
Interactive Visualization Magnesium — the mineral that makes ATP work Bare ATP is useless and enzymes reject it. Watch magnesium clamp the phosphates and switch it on, plug the NMDA channel, and let a cramping muscle finally let go. Launch →
Table of Contents
- Symptom Deep-Dive Pages
- What Is Hypomagnesemia?
- Why Low Magnesium Causes So Many Different Symptoms
- Common Causes of Low Magnesium
- The Potassium and Calcium Connection
- How Hypomagnesemia Is Diagnosed
- How Low Magnesium Is Corrected
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Is Hypomagnesemia?
Magnesium is a mineral your body cannot work without. It sits at the center of more than 300 enzyme reactions — the chemical steps that build proteins, run the nervous system, and let your cells use energy — and it helps keep the heartbeat steady and the muscles relaxed between contractions. Hypomagnesemia is the medical word for a blood (serum) magnesium level below about 1.7 mg/dL (roughly 0.7 mmol/L). A normal level sits between about 1.7 and 2.2 mg/dL (0.7–0.95 mmol/L), though labs vary slightly. The prefix "hypo-" means low, and "-magnesemia" simply means magnesium in the blood.
How low the number falls and how fast it dropped both shape what a person feels:
- Mild (about 1.4–1.7 mg/dL) — Often there are no symptoms at all, and the low value — if it is measured at all — turns up by chance. When symptoms do appear they are easy to dismiss: a few extra muscle twitches, an occasional night cramp, a little more anxiety or trouble falling asleep, vague tiredness. Most people would never connect these to magnesium.
- Moderate (about 1.0–1.4 mg/dL) — Now the body usually notices. Cramps and twitches become more frequent, sleep and mood can suffer, and some people feel their heart flutter or skip. Nausea and poor appetite may appear. This is the range where someone tends to seek help and where a doctor will want to investigate and treat.
- Severe (below about 1.0 mg/dL) — This can become a medical emergency. Severe deficiency can trigger muscle spasms and even tetany (sustained, painful cramping), numbness and tingling, confusion, and seizures; most dangerously, it destabilizes the heart's electrical rhythm and can provoke serious arrhythmias. People this low usually need treatment in a hospital, often with intravenous magnesium and heart monitoring.
Two facts are worth holding together. First, hypomagnesemia is common but under-recognized: it is found in a large share of hospitalized and critically ill patients, and population surveys suggest that many adults take in less magnesium than recommended, leaving them with a chronic, low-grade shortfall that researchers call subclinical magnesium deficiency. Second — and this is the crux — the blood test sees only a sliver of the body's magnesium. Only about 1% of the body's magnesium circulates in the blood; the rest is locked inside bone and cells. Because the body works hard to keep the blood level steady (even pulling magnesium out of bone to do it), a "normal" serum result can sit on top of a real whole-body deficit. That is exactly why a person can have clear symptoms of low magnesium while a single blood test looks reassuringly fine.
Why Low Magnesium Causes So Many Different Symptoms
The puzzle of hypomagnesemia is how one shortage can cause complaints as different as a leg cramp, a fluttering heartbeat, a sleepless and anxious night, and bone-deep fatigue. The answer is that magnesium is not a specialist — it is a quiet, behind-the-scenes helper that hundreds of the body's machines depend on. Restore it and the scattered symptoms tend to ease together; let it fall and they tend to appear together.
Here is the core idea in plain language. Magnesium does two jobs that explain almost everything on the symptom list. First, it is the body's natural "calm-down" mineral for nerve and muscle cells. Calcium is the signal that makes a muscle contract and a nerve fire; magnesium is the brake that lets them relax and reset afterward. The two work as a push-and-pull pair. When magnesium runs low, that brake weakens: cells become over-excitable, firing too easily and relaxing too slowly. Picture a guitar string tuned too tight — it twangs at the slightest touch. That is why low magnesium shows up as twitching muscles, painful cramps, jitteriness, anxiety, and a nervous system that will not switch off at night.
Second, magnesium is the partner your cells need to actually use their energy. The body's energy currency, ATP, is biologically active only when it is bound to magnesium — chemists literally write it as Mg-ATP. So magnesium sits at the heart of how every cell powers itself, which is part of why a shortage so often feels like a flat, foggy fatigue rather than any one dramatic symptom.
Because the same mineral sits behind so many functions, a single low level ripples outward across many systems at once:
- Skeletal muscle — the voluntary muscles become over-excitable and slow to relax, producing twitches, eyelid flutters, and painful cramps. (Deep dive: Muscle Cramps & Twitches.) See also the physiology on Magnesium and Muscle Function.
- The heart — cardiac muscle is the most electrically sensitive tissue of all, and magnesium helps stabilize the rhythm between beats. Low magnesium can produce a fluttering or skipping sensation and, in deeper deficiency, true arrhythmias. (Deep dive: Heart Palpitations.) See Magnesium and Heart Health and Arrhythmia.
- The brain and nervous system — without enough of its calming mineral, the nervous system stays on edge, which can feel like anxiety, irritability, and the inability to wind down into sleep. (Deep dive: Anxiety & Insomnia.) See Magnesium and Sleep.
- Whole-body energy and the head — because magnesium underpins how cells make and use energy, low levels frequently show up as disproportionate tiredness; magnesium is also a recognized contributor to migraine and tension headaches. (Deep dive: Fatigue & Headaches.) See Magnesium and Migraines.
This is the unifying theme to carry into the symptom pages: there is nothing mysterious about low magnesium producing a scattershot of complaints. One mineral steadies the electrical "calm" of many tissues and powers the energy in every cell, so one low level is felt in many places at once.
Common Causes of Low Magnesium
Magnesium runs low for one of three broad reasons: you are taking in too little, you are losing too much (through the gut or the kidneys), or a medication or illness is actively wasting it. In real life these often combine. Here are the causes worth knowing.
- A modern, processed diet — magnesium lives in whole, unrefined foods: leafy greens, nuts, seeds, beans, and whole grains. Refining grains and eating few plants strips most of it out, and national surveys suggest a large share of adults fall short of the recommended intake. On its own this rarely crashes the blood level in a healthy person, because the kidney conserves magnesium well — but it sets the stage, leaving little reserve when any of the losses below are added.
- Diarrhea and gut disorders — the digestive tract is a major route of loss. Prolonged diarrhea, vomiting, and conditions such as Crohn's disease, celiac disease, ulcerative colitis, or surgery that shortens the bowel all reduce how much magnesium is absorbed and increase what is lost. Chronic diarrhea is one of the classic causes of stubborn low magnesium.
- Diuretics ("water pills") — loop diuretics (such as furosemide) and thiazide diuretics (such as hydrochlorothiazide), used for high blood pressure and heart failure, make the kidneys excrete magnesium along with sodium and potassium. Because these drugs are so common, they are a leading medical cause of low magnesium — and they lower potassium at the same time, which matters greatly (see the next section).
- Proton pump inhibitors (PPIs) — long-term use of acid-reducing drugs such as omeprazole and pantoprazole can lower magnesium absorption from the gut. The link is well enough established that the U.S. FDA issued a safety warning, and observational studies tie prolonged PPI use to hypomagnesemia. If you take a PPI for years and have symptoms, it is worth checking.
- Alcohol use — regular heavy drinking depletes magnesium through several routes at once: poor diet, vomiting and diarrhea, and a direct effect that makes the kidney waste magnesium. Low magnesium is common in people with alcohol use disorder and contributes to the tremor and agitation of withdrawal.
- Poorly controlled diabetes — high blood sugar pulls extra water (and magnesium) into the urine, so people with type 2 diabetes are frequently low in magnesium — which, in turn, can worsen blood-sugar control, creating a self-reinforcing loop.
- Certain medications — beyond diuretics and PPIs, some antibiotics (aminoglycosides), antifungals, the immune-suppressant drugs used after transplants, and several chemotherapy agents (notably cisplatin) can make the kidney waste magnesium.
- Refeeding — when someone who has been starved or chronically undernourished suddenly resumes eating, a surge of insulin drives magnesium (along with potassium and phosphate) rapidly into cells, and blood levels can fall sharply within hours. This "refeeding syndrome" is dangerous and is why hospitals reintroduce nutrition slowly and watch these minerals closely.
- Inherited kidney disorders — less common genetic conditions, such as Gitelman syndrome and several named tubular disorders, cause the kidney to leak magnesium continuously. These deserve a specialist's attention when low magnesium is persistent and unexplained, especially in younger people.
A practical note: these causes stack. An older adult eating a refined diet, taking a thiazide diuretic and a daily PPI, who then has a bout of diarrhea, can become quite low from the sum of several modest pushes in the same direction.
The Potassium and Calcium Connection
Magnesium almost never travels alone. If you remember one thing beyond the basics, make it this: low magnesium drags potassium and calcium down with it, and you often cannot fix those two until you fix the magnesium first. This is why any careful work-up for low magnesium also checks potassium and calcium, and why magnesium is the mineral that quietly explains a lot of otherwise puzzling lab results.
Magnesium and potassium. The link is elegant. Inside the kidney's tubules sit potassium channels (called ROMK channels) that control how much potassium leaves the body. Magnesium acts like a soft plug on those channels from the inside, limiting potassium loss. When magnesium runs low, that plug is removed, the channels open wider, and the kidney begins to leak potassium into the urine. The result is that low potassium (hypokalemia) becomes refractory — resistant to potassium pills — until the magnesium deficit is corrected. A patient can be given potassium again and again with the level barely budging, when the real fix was a few hundred milligrams of magnesium. The two minerals are also depleted by the same causes — diuretics, diarrhea, alcohol, poor diet — so finding one low makes the other likely.
Magnesium and calcium. Magnesium is also required for the body to manage calcium. The gland that controls calcium (the parathyroid) needs magnesium to release its hormone and to let that hormone work. When magnesium falls low enough, parathyroid hormone is blunted, and blood calcium can drop too — producing low calcium (hypocalcemia) that, like the potassium problem, will not respond to calcium alone until magnesium is restored. This is one reason severe magnesium deficiency can cause tetany and tingling: low magnesium and the low calcium it drags down both make nerves and muscles over-excitable. Researchers have also examined how magnesium status interacts with vitamin D, since magnesium is needed for the body to activate vitamin D as well.
The practical takeaways:
- When potassium or calcium is unexpectedly low — or refuses to come up with replacement — magnesium should be checked and corrected, not as an afterthought but as the key that unlocks the others.
- Replacing magnesium can, by itself, allow the kidney to start retaining potassium again and the parathyroid to manage calcium again, sometimes raising both with little additional supplementation.
- Because the three minerals move together and amplify one another's symptoms, "fix magnesium first" is a sound rule of thumb in this trio.
For more on the partner minerals, see the Potassium and Calcium overviews, the low-potassium hub, and the Magnesium Replenishment page.
How Hypomagnesemia Is Diagnosed
The catch with diagnosing low magnesium is that it is often not measured. Magnesium is not part of the standard basic metabolic panel or comprehensive metabolic panel (CMP) — the routine bloodwork that automatically reports sodium, potassium, calcium, and kidney function. A serum magnesium has to be specifically ordered. So the first and most important step is simply for someone (you or your doctor) to think of it and ask for the test, especially in the situations that make it likely: taking a diuretic or a long-term PPI, heavy alcohol use, chronic diarrhea or gut disease, poorly controlled diabetes, or unexplained low potassium or calcium. (For what the standard panel does and does not cover, see the Comprehensive Metabolic Panel page.)
When magnesium is checked, a doctor may use several tools, each with a known limitation:
- Serum (blood) magnesium — the standard, inexpensive test, and the one used to diagnose hypomagnesemia. Its great limitation, covered above, is that it reflects only the roughly 1% of body magnesium in the blood; because the body defends the blood level, serum magnesium can read normal while the cells and bones are depleted. A low serum result is meaningful, but a normal one does not fully rule out a deficit in someone with clear symptoms and a strong reason to be low.
- Potassium and calcium — checked alongside magnesium for the reasons in the section above. Finding low potassium or low calcium that will not correct is itself a clue to look for — and treat — low magnesium.
- Urine magnesium — a urine test (a spot sample or a 24-hour collection, sometimes expressed as a fractional excretion) helps answer where the magnesium is going. A high amount in the urine points to a kidney or drug cause (diuretics, certain medications, inherited tubular disorders), while a low amount points toward poor intake or losses from the gut. This single test often cracks an otherwise puzzling case.
- An electrocardiogram (ECG / EKG) — a quick, painless tracing of the heart's electrical activity. Because severe magnesium deficiency destabilizes the heart's rhythm (and because it so often comes packaged with low potassium and calcium), an ECG may be done when the level is low and symptoms or risk factors are present.
For everyday purposes, the most useful message is the simplest one: if the symptoms and the risk factors fit, ask whether magnesium has actually been measured — it is easy to overlook precisely because it is not on the default panel.
How Low Magnesium Is Corrected
Treatment is matched to severity, symptoms, and cause. The unifying principles are: replace magnesium at a pace that matches the danger, check and replace potassium and calcium alongside it, and address the underlying reason so it does not simply happen again.
- Mild cases — food first. When magnesium is only modestly low and there are no worrying symptoms, the kindest and most lasting fix is dietary, because magnesium-rich foods are nourishing in many other ways too. Excellent sources include leafy greens such as spinach, nuts and seeds such as almonds and pumpkin seeds, beans and lentils, whole grains, avocado, and dark chocolate. See the magnesium-rich foods page for a fuller list and practical amounts.
- Mild-to-moderate cases — oral magnesium. When food alone is not enough, oral magnesium supplements are used. The form matters for tolerability: well-absorbed organic salts such as magnesium glycinate, citrate, and malate tend to be gentler on the stomach, whereas magnesium oxide is poorly absorbed and the most likely to cause loose stools or diarrhea (the same property that makes magnesium-based products work as laxatives). Spreading the dose through the day and taking it with food reduces the laxative effect. Because so much swallowed magnesium passes into the stool, raising a true deficit can take several weeks of consistent intake.
- Severe or symptomatic cases — intravenous magnesium in hospital. When magnesium is dangerously low, or there are serious symptoms such as seizures, tetany, or arrhythmia, magnesium is given through a vein in a carefully controlled way, usually with monitoring and repeat testing. IV repletion is hospital territory, not something done at home.
- A word of caution — the kidneys set the limit. Healthy kidneys excrete excess magnesium easily, so magnesium overload from food or ordinary supplements is rare. But in people with reduced kidney function, magnesium can build up to harmful levels, so magnesium supplements (including over-the-counter magnesium-containing laxatives and antacids) should be used only with medical guidance. For what too much magnesium looks like, see the magnesium toxicity hub.
- Always: check potassium and calcium. As covered above, low magnesium drags both down and can make them resistant to replacement. Correcting magnesium is part of correcting those, not separate from it.
- Always: treat the cause. Replacing magnesium without addressing why it dropped just resets the clock. That might mean reviewing a diuretic or a long-term PPI, treating diarrhea or gut disease, addressing alcohol use, improving diabetes control, or evaluating a kidney tubular disorder.
For most people the outlook is excellent: once magnesium (and its partner minerals) are restored and the cause is handled, the cramps, palpitations, anxiety, poor sleep, fatigue, and headaches tend to ease, often within days to a few weeks.
When to Seek Care / Red Flags
Most low-magnesium symptoms are uncomfortable rather than dangerous, and a non-urgent call to your doctor — asking specifically for a magnesium level along with potassium and calcium — is the right step for ongoing cramps, twitches, anxiety, poor sleep, or fatigue, especially if you take a water pill or a long-term acid-reducer, drink heavily, or have a gut condition. But certain symptoms mean magnesium (and the minerals it pulls down with it) may be dangerously low and the heart or brain could be at risk. Seek emergency care right away if you have any of the following:
- A seizure or convulsion — new seizures, or any seizure in someone known to be at risk for low magnesium, are an emergency.
- Palpitations with faintness — a racing, pounding, or irregular heartbeat, especially with lightheadedness, near-fainting, or fainting, which can signal a dangerous rhythm.
- Severe muscle spasms or tetany — sustained, painful cramping, or cramping of the hands and face, sometimes with numbness and tingling around the mouth and fingers.
- Confusion or marked changes in alertness — new disorientation, agitation, or difficulty staying awake.
- Inability to keep fluids down — persistent vomiting or diarrhea so that you cannot eat or drink, which both deepens the deficiency and points to dehydration.
People at higher risk — those on diuretics or long-term PPIs, with heart disease, with kidney problems, with significant alcohol use, or recovering from starvation — should have a lower threshold for getting checked, because in these settings even a modest shortfall can have outsized effects and rarely travels alone. When in doubt, a simple blood test (remembering that magnesium must be specifically requested) settles much of the question. For related heart-rhythm symptoms, see Heart Palpitations and Arrhythmia.
Key Research Papers
- de Baaij JHF, Hoenderop JGJ, Bindels RJM (2015). Magnesium in Man: Implications for Health and Disease. Physiological Reviews;95(1):1-46. — DOI: 10.1152/physrev.00012.2014
- Jahnen-Dechent W, Ketteler M (2012). Magnesium basics. Clinical Kidney Journal;5(Suppl 1):i3-i14. — DOI: 10.1093/ndtplus/sfr163
- Gröber U, Schmidt J, Kisters K (2015). Magnesium in Prevention and Therapy. Nutrients;7(9):8199-8226. — DOI: 10.3390/nu7095388
- Fiorentini D, Cappadone C, Farruggia G, Prata C (2021). Magnesium: Biochemistry, Nutrition, Detection, and Social Impact of Diseases Linked to Its Deficiency. Nutrients;13(4):1136. — DOI: 10.3390/nu13041136
- Ayuk J, Gittoes NJL (2014). Treatment of Hypomagnesemia. American Journal of Kidney Diseases;63(4):691-695. — DOI: 10.1053/j.ajkd.2013.07.025
- Rosanoff A, Weaver CM, Rude RK (2012). Suboptimal magnesium status in the United States: are the health consequences underestimated? Nutrition Reviews;70(3):153-164. — DOI: 10.1111/j.1753-4887.2011.00465.x
- Rosanoff A, Dai Q, Shapses SA (2016). Essential Nutrient Interactions: Does Low or Suboptimal Magnesium Status Interact with Vitamin D and/or Calcium Status? Advances in Nutrition;7(1):25-43. — DOI: 10.3945/an.115.008631
- DiNicolantonio JJ, O'Keefe JH, Wilson W (2018). Subclinical magnesium deficiency: a principal driver of cardiovascular disease and a public health crisis. Open Heart;5(1):e000668. — DOI: 10.1136/openhrt-2017-000668
- Garrison SR, Korownyk CS, Kolber MR, Allan GM, et al. (2020). Magnesium for skeletal muscle cramps. Cochrane Database of Systematic Reviews;(9):CD009402. — DOI: 10.1002/14651858.CD009402.pub3
- Boyle NB, Lawton C, Dye L (2017). The Effects of Magnesium Supplementation on Subjective Anxiety and Stress — A Systematic Review. Nutrients;9(5):429. — DOI: 10.3390/nu9050429
- Mah J, Pitre T (2021). Oral magnesium supplementation for insomnia in older adults: a systematic review & meta-analysis. BMC Complementary Medicine and Therapies;21(1):125. — DOI: 10.1186/s12906-021-03297-z
- Mauskop A, Varughese J (2012). Why all migraine patients should be treated with magnesium. Journal of Neural Transmission;119(5):575-579. — DOI: 10.1007/s00702-012-0790-2
- Proton pump inhibitors and hypomagnesemia (FDA safety communication; observational meta-analyses). — PubMed
PubMed Topic Searches
- PubMed — Hypomagnesemia: causes, diagnosis, and management
- PubMed — Magnesium deficiency, hypokalemia, and hypocalcemia
- PubMed — Diuretic-induced hypomagnesemia
- PubMed — Magnesium supplementation, sleep, and anxiety (trials)
- PubMed — Magnesium for migraine prophylaxis
Connections
- Magnesium: The Mineral That Makes ATP Work — interactive animation
- Hypomagnesemia: Muscle Cramps & Twitches
- Hypomagnesemia: Heart Palpitations
- Hypomagnesemia: Anxiety & Insomnia
- Hypomagnesemia: Fatigue & Headaches
- Magnesium Overview
- Magnesium Toxicity Hub
- Magnesium Benefits Hub
- Magnesium and Muscle Function
- Magnesium and Heart Health
- Magnesium and Sleep
- Magnesium and Migraines
- Magnesium-Rich Foods
- Magnesium Replenishment
- Potassium
- Hypokalemia (Low Potassium)
- Calcium
- Comprehensive Metabolic Panel
- Arrhythmia
- Heart Palpitations
- Anxiety
- Insomnia
- Migraine
- Kidney Disease
- Spinach
- Almonds
- Pumpkin Seeds