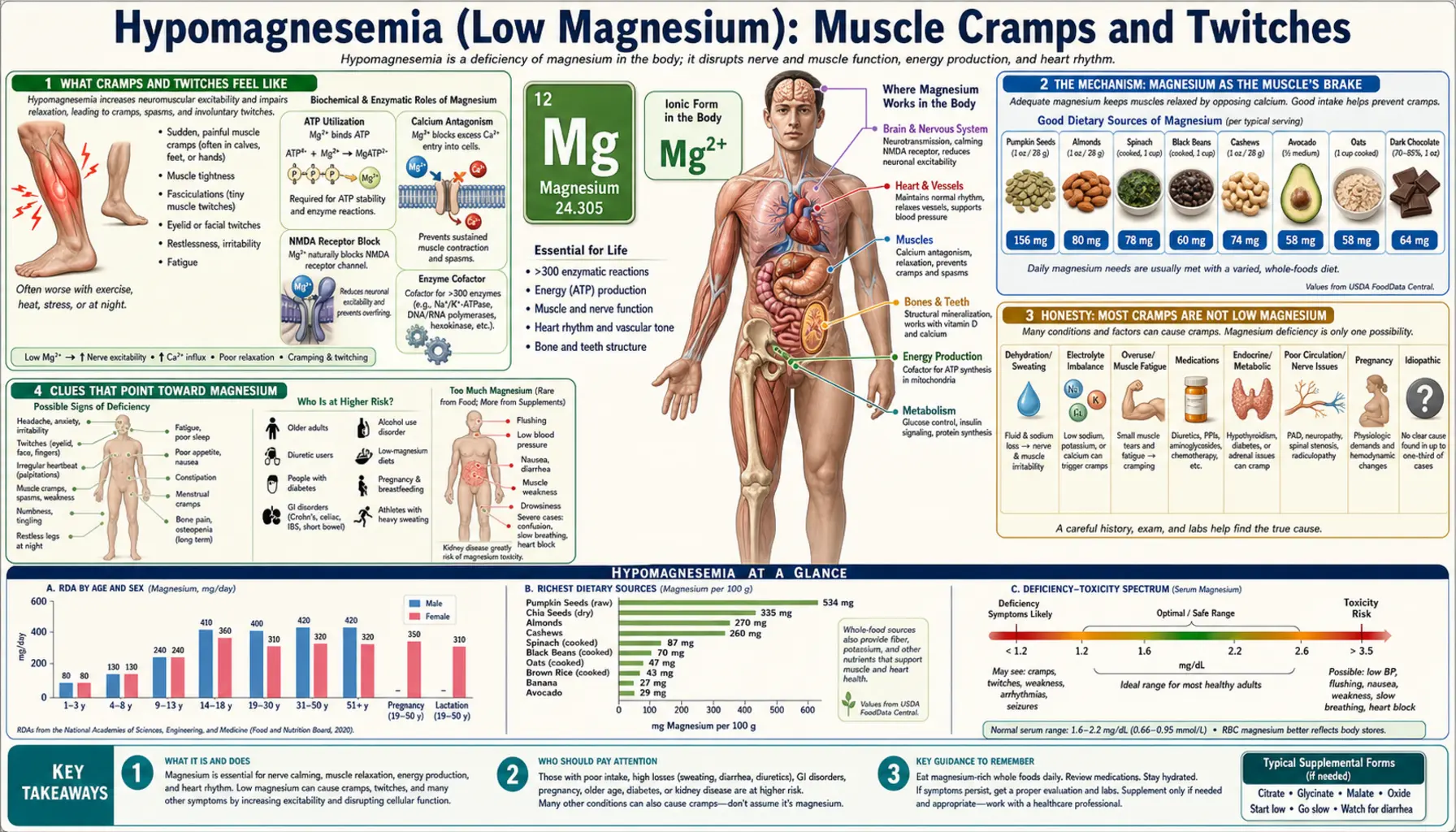
Hypomagnesemia (Low Magnesium): Muscle Cramps and Twitches
A sudden, gripping charley horse in the calf that wakes you at 2 a.m. — or a tiny muscle near your eye that flutters for days — is one of the most common reasons people start wondering about magnesium. There is real biology behind that hunch: magnesium is the mineral that keeps muscle and nerve electrically calm, and when it runs low, muscle can fire when it shouldn't. This page explains the difference between a cramp and a twitch, why low magnesium makes muscle over-excitable, the honest truth that most cramps are not caused by low magnesium, the clues that point toward magnesium specifically, and how the deficiency is tested and corrected. If you also notice a racing or skipping heartbeat with your cramps, that points beyond muscle — see heart palpitations.
Interactive Visualization Magnesium — the mineral that makes ATP work Bare ATP is useless and enzymes reject it. Watch magnesium clamp the phosphates and switch it on, plug the NMDA channel, and let a cramping muscle finally let go. Launch →
Table of Contents
- What Cramps and Twitches Feel Like
- The Mechanism: Magnesium as the Muscle's Brake
- Honesty: Most Cramps Are Not Low Magnesium
- Clues That Point Toward Magnesium
- What Drains Magnesium
- Getting Tested — and Why the Blood Test Can Mislead
- Correcting Low Magnesium Safely
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Cramps and Twitches Feel Like
“Cramps and twitches” actually covers three different experiences. They can overlap and they can all show up when magnesium is low, but they are not the same thing, and telling them apart helps you and a clinician figure out what is going on.
- A cramp (the charley horse). A sudden, painful, involuntary contraction of a whole muscle — most famously the calf, but also the foot, thigh, or hand. The muscle visibly knots, you can feel it harden, and it can last from seconds to a couple of minutes. Night-time leg cramps that yank you out of sleep are the classic version. The muscle can stay tender and “bruised-feeling” for hours afterward.
- A twitch or fasciculation. A small, fine, painless ripple or flicker under the skin — one little bundle of muscle fibers firing on its own. The eyelid is the most familiar place (the harmless “eye twitch” nearly everyone has had), but twitches also visit the calf, thigh, or thumb. They can flutter for minutes, come and go for days, and feel unnerving precisely because you can see them and can't control them.
- Tetany and tingling. At the more pronounced end, low magnesium can produce tetany — involuntary cramping spasms of the hands and feet, sometimes with tingling or a “pins-and-needles” feeling around the mouth and in the fingers. The hand may draw into a characteristic claw-like posture. This reflects nerves and muscles that have become genuinely over-excitable, and it overlaps heavily with the effects of low calcium (more on that below).
The common thread is over-excitable muscle and nerve — tissue that fires when it should be resting. A cramp is a big, sustained, painful version of that; a twitch is a tiny, brief, painless version; tetany sits at the excitable extreme. What they share is the underlying state that magnesium normally prevents. This page is about that one family of symptoms; the deeper electrical instability that shows up in the heart as a fluttering or skipping beat is covered separately on the heart palpitations page, and the wired-but-tired, sleepless feeling of low magnesium on the anxiety and insomnia page.
The Mechanism: Magnesium as the Muscle's Brake
To understand why low magnesium makes muscle twitch and cramp, it helps to know what magnesium does at the cellular level. Inside the body, magnesium is the second-most-abundant mineral inside cells, and it acts on muscle and nerve in two complementary ways — both of which are calming, braking influences.
First, magnesium gates calcium. Muscle contraction is driven by calcium: when a muscle fiber is told to contract, calcium floods into the working part of the cell, the filaments slide, and the muscle shortens. Magnesium acts as a natural calcium-channel blocker — it sits at the gates that let calcium in and pushes calcium back out, keeping resting calcium low so the muscle stays relaxed between commands. When magnesium is plentiful, calcium only surges when it is supposed to. When magnesium is scarce, those gates leak, resting calcium creeps up, and the muscle is biased toward contracting — primed to knot into a cramp.
Second, magnesium stabilizes the electrical membrane. Magnesium helps run the Na+/K+-ATPase pump, the tiny molecular pump (it physically requires magnesium-bound ATP to operate) that maintains the charged, stable resting state of every nerve and muscle membrane. A well-charged membrane sits quietly and only fires when a real signal arrives. When magnesium falls, the pump falters, the membrane becomes leaky and unstable, and nerve and muscle become hyper-excitable — they discharge spontaneously. A motor nerve ending that fires on its own makes the little bundle of fibers it controls twitch; that is a fasciculation. Magnesium also blocks the NMDA receptor on nerves, another braking action that, when lost, leaves nerves more easily triggered.
An analogy. Picture each muscle as a car idling at a stoplight, with magnesium as the brake pedal held lightly down. With enough magnesium, the car waits calmly and only moves when you press the gas (the nerve signal). Let the brake go — lose the magnesium — and the idling engine starts to creep and lurch on its own: a little lurch is a twitch, a hard lunge forward is a cramp. The accelerator (calcium) hasn't changed; what's missing is the brake that was holding everything in check. Restore magnesium and the foot is back on the brake — the muscle idles quietly again.
This is also why magnesium and calcium are so often discussed together. They are functional opposites at the muscle: calcium contracts, magnesium relaxes. Symptoms of low magnesium and symptoms of low calcium overlap heavily — both cause cramps, twitches, and tetany — and, importantly, severe magnesium deficiency actually drives calcium down too (it shuts off the parathyroid hormone that defends blood calcium), so the two can travel together.
Honesty: Most Cramps Are Not Low Magnesium
Here is the part the supplement aisle won't tell you: the great majority of ordinary muscle cramps and twitches are not caused by magnesium deficiency at all. It is the right instinct to ask about magnesium, but it would be wrong to assume a cramp proves you are deficient. Being honest about this matters, because chasing the wrong cause means the real one goes untreated.
For the most common scenario — ordinary night-time leg cramps in otherwise healthy adults — the evidence on magnesium is genuinely disappointing. A Cochrane systematic review pooling multiple randomized trials concluded that magnesium supplements are unlikely to provide meaningful benefit for idiopathic (no known cause) leg cramps in the general adult and older-adult population. People took magnesium, and on average their cramps were no better than with placebo. That is a strong, well-conducted finding, and it deserves to be stated plainly.
So what does cause most cramps and twitches? A wide and very ordinary list:
- Benign, everyday causes of twitches: too much caffeine, poor sleep, stress and anxiety, and plain muscle fatigue. The classic harmless eyelid twitch is almost always one of these — not a mineral problem.
- Exercise and dehydration: cramps during or after hard exercise are often linked to muscle overload and fatigue (and, in heavy sweaters, to sodium and fluid loss) rather than to magnesium.
- Other electrolytes: low potassium, low calcium, and low sodium all cause cramps in their own right — and they often move with magnesium, which is part of why the picture is muddled.
- Medications: diuretics (“water pills”), statins, and some asthma and blood-pressure drugs can provoke cramps.
- Medical conditions: pregnancy, peripheral artery disease, an underactive thyroid, nerve and motor-neuron disorders, liver disease, and chronic kidney disease.
- Just aging: night leg cramps become more common with age even when nothing is wrong.
There is one cramp setting where magnesium has better evidence than the rest: pregnancy-related leg cramps, where at least one randomized controlled trial found that oral magnesium reduced the frequency and intensity of cramps. Pregnancy is a special case — magnesium needs rise and stores can run low — so it is reasonable for a pregnant person to discuss magnesium with their clinician even though the general-population evidence is weak. The honest bottom line: a cramp is a clue, not a diagnosis. It is worth asking whether magnesium is low, but the answer is often no.
Clues That Point Toward Magnesium
If most cramps aren't magnesium, when should you suspect it? The tell is rarely the cramp by itself — it is the company the cramp keeps. Magnesium deficiency tends to announce itself as a cluster, and a few patterns make it much more likely:
- Cramps and twitches plus a cause that drains magnesium. This is the strongest clue. Heavy alcohol use, long-term gut problems with diarrhea or malabsorption (Crohn's, celiac, chronic diarrhea), uncontrolled diabetes, and certain long-term medications (see the next section) all waste magnesium. Cramps appearing on that background deserve a magnesium check.
- The multi-system cluster. Magnesium deficiency rarely stays in one place. Cramps and twitches arriving together with a fluttering or skipping heartbeat, a wired-but-tired anxious, sleepless feeling, or fatigue and headaches is far more suggestive than a lone calf cramp.
- Tingling and frank tetany. Tingling around the mouth or in the fingers, or hands and feet that cramp into a spasm, point toward a genuine excitability problem — and toward low magnesium and/or low calcium — rather than an ordinary charley horse.
- Potassium that won't come up. A known but stubborn low potassium level that refuses to correct despite supplements is a well-known fingerprint of hidden magnesium deficiency; the body cannot hold onto potassium properly when magnesium is low.
By contrast, an isolated eye twitch when you're stressed and under-slept, or a single calf cramp after a long hike, in a healthy person eating a normal diet, is far more likely to be benign than a sign of deficiency. The skill is reading the pattern, not the single symptom.
What Drains Magnesium
True magnesium deficiency severe enough to cause cramps and twitches usually has a reason behind it. The kidneys are good at conserving magnesium when intake is low, so a genuine deficiency typically means either it isn't getting in, it's being lost, or it's being pulled out of the body faster than normal. The usual culprits:
- Low dietary intake. Modern diets heavy in refined and processed foods are often short on magnesium; population surveys find that a substantial share of adults take in less than the recommended amount. The richest sources are whole foods — leafy greens, nuts and seeds, legumes, and whole grains — exactly the foods that get crowded out by processed ones.
- Alcohol. Chronic heavy drinking is one of the most common causes of clinically significant magnesium deficiency: alcohol both makes the kidneys dump magnesium and goes hand-in-hand with poor intake.
- Gut losses and malabsorption. Prolonged diarrhea, vomiting, and disorders such as Crohn's disease, celiac disease, and the aftermath of bowel surgery reduce how much magnesium the gut can absorb. Because most magnesium is absorbed in the small intestine, chronic diarrhea is a classic setup.
- Medications. Two groups stand out. Diuretics (loop and thiazide “water pills”) make the kidneys excrete magnesium. Proton-pump inhibitors (PPIs — long-term acid-reflux drugs such as omeprazole) can lower magnesium when taken for months to years; this is recognized enough that drug regulators have warned about it. Some chemotherapy agents and certain antibiotics also waste magnesium.
- Diabetes and kidney handling. Poorly controlled diabetes spills magnesium into the urine, and several inherited and acquired kidney conditions impair magnesium reabsorption.
- Rare inherited disorders. Genetic defects in the channels that absorb magnesium — for example mutations in the TRPM6 transporter — cause severe hypomagnesemia from infancy, often presenting with tetany and seizures precisely because magnesium (and the calcium it props up) are both low.
Identifying which of these is at work matters, because the fix differs: stopping a needless PPI, treating the gut disease, or cutting back alcohol addresses the source, whereas simply swallowing more magnesium without fixing an ongoing drain only partly helps.
Getting Tested — and Why the Blood Test Can Mislead
The standard test is a serum magnesium level — a simple, inexpensive blood draw. It is the right first step, and a clearly low result confirms deficiency. Magnesium is not included on a routine Comprehensive Metabolic Panel, so it usually has to be ordered specifically; if you are asking about cramps, ask for it by name. A clinician will often check calcium and potassium at the same time, because all three move together and low magnesium frequently drags the other two down.
But there is an honest and important limitation that patients deserve to know: a “normal” serum magnesium does not guarantee your body stores are adequate. Only about 1% of the body's magnesium is in the blood — the rest is locked inside bone and cells. The body works hard to keep the blood level in range, even pulling magnesium out of bone to do it, so the serum number can read normal while total-body magnesium is genuinely depleted. Researchers call this normomagnesemic magnesium deficiency, and it is a recognized blind spot: reviews of how magnesium status is measured conclude that the routine blood test underestimates true deficiency. The practical consequence is real: a normal serum magnesium reduces the likelihood that magnesium is your problem, but it does not entirely rule it out, especially when the clinical picture (alcohol, gut losses, diuretics, a stubborn low potassium) points strongly toward it.
When deeper assessment is needed, clinicians have other tools — a 24-hour urine magnesium (to see whether the kidneys are wasting it), a magnesium-loading/retention test in difficult cases, and an electrocardiogram (ECG) when the heart may be involved. For everyday purposes, though, the workflow is straightforward: a serum magnesium (plus calcium and potassium), read in the context of your symptoms and your risk factors.
Correcting Low Magnesium Safely
How magnesium is replaced depends on how low it is, how it's being lost, and how symptomatic you are. The guiding idea is food first for mild cases, supplements when needed, and intravenous (IV) magnesium reserved for severe or dangerous deficiency — always alongside fixing the cause.
- Food first. For mild shortfalls in an otherwise healthy person, magnesium-rich whole foods are the foundation and carry essentially no risk of overshoot. The best sources are pumpkin and chia seeds, almonds and cashews, leafy greens like spinach and Swiss chard, legumes (beans and lentils), whole grains, and dark chocolate. Building these into the diet raises magnesium gently and brings potassium and fiber along for the ride.
- Oral supplements. When diet isn't enough, oral magnesium is used. The most common practical issue is the laxative effect: poorly absorbed forms such as magnesium oxide and magnesium citrate loosen the stool (citrate and oxide are, in fact, sold as laxatives), so the dose that fixes magnesium can also cause diarrhea — which is self-defeating, since diarrhea wastes magnesium. Better-absorbed, gentler-on-the-gut forms such as magnesium glycinate (magnesium bound to the amino acid glycine) are often preferred for replacing stores; see Magnesium Replenishment for more on forms and dosing. Because oral magnesium absorption is limited and slow, correcting a real deficiency takes weeks of consistent intake, not days.
- Intravenous magnesium. Severe, symptomatic deficiency — tetany, seizures, dangerous heart rhythms — is treated in a medical setting with IV magnesium, which bypasses the gut and the slow absorption.
- Replace calcium and potassium too, and fix the cause. Because low magnesium drags down calcium and potassium, those often need correcting alongside — and the famous clinical pearl is that potassium and calcium will not stay corrected until the magnesium is fixed. Equally important is addressing why magnesium dropped: reviewing a diuretic or long-term PPI, treating gut disease, or reducing alcohol.
A genuine caution. Magnesium supplements are not risk-free for everyone. People with reduced kidney function clear magnesium poorly and can build up dangerously high levels (hypermagnesemia) from ordinary supplement doses, so anyone with kidney disease should only take magnesium under medical guidance. Magnesium can also interact with certain antibiotics and other drugs. “Natural” does not mean “take as much as you like.”
When to Seek Care / Red Flags
Most cramps and twitches are benign and can be discussed at a routine visit. But certain features mean you should be evaluated promptly — and some mean seek emergency care right away:
- Cramping spasms of the hands and feet, or tingling around the mouth and fingers (tetany). This signals genuine nerve-muscle over-excitability and possible low magnesium and/or calcium — get checked soon.
- A seizure, severe confusion, or fainting — profound magnesium (and calcium) deficiency can cause these. Call emergency services.
- Palpitations — a racing, pounding, fluttering, or skipping heartbeat — with your cramps. Low magnesium can destabilize heart rhythm and trigger dangerous arrhythmias; combined with cramps this is the pattern that needs urgent attention (see heart palpitations and heart palpitations).
- Twitching that spreads, comes with progressive weakness, muscle wasting, slurred speech, or trouble swallowing. Persistent, spreading fasciculations with weakness can point to a nerve or motor-neuron disorder rather than a mineral problem and need neurological evaluation — do not assume it is “just magnesium.”
- A single muscle — usually the calf — that is suddenly painful, swollen, warm, and red, rather than briefly cramping and then easing. That can be a blood clot (deep vein thrombosis), not a cramp, and is an emergency.
- Cramps with very dark (tea- or cola-colored) urine and severe weakness — a sign of muscle breakdown (rhabdomyolysis). Seek care promptly.
The reassuring flip side: a brief, isolated eye twitch when you're stressed and short on sleep, or an occasional night calf cramp that resolves in a minute, in an otherwise healthy person, is almost always benign. When cramps and twitches are frequent, worsening, or keep the company described above, that is the time to be seen.
Key Research Papers
- Agus ZS (1999). Hypomagnesemia. Journal of the American Society of Nephrology;10(7):1616-1622. — DOI: 10.1681/ASN.V1071616
- de Baaij JHF, Hoenderop JGJ, Bindels RJM (2015). Magnesium in Man: Implications for Health and Disease. Physiological Reviews;95(1):1-46. — DOI: 10.1152/physrev.00012.2014
- Miller TM, Layzer RB (2005). Muscle cramps. Muscle & Nerve;32(4):431-442. — DOI: 10.1002/mus.20341
- Garrison SR, Korownyk CS, Kolber MR, et al. (2020). Magnesium for skeletal muscle cramps. Cochrane Database of Systematic Reviews;2020(9):CD009402. — DOI: 10.1002/14651858.CD009402.pub3
- Supakatisant C, Phupong V (2015). Oral magnesium for relief in pregnancy-induced leg cramps: a randomised controlled trial. Maternal & Child Nutrition;11(2):139-145. — DOI: 10.1111/j.1740-8709.2012.00440.x
- Workinger JL, Doyle RP, Bortz J (2018). Challenges in the Diagnosis of Magnesium Status. Nutrients;10(9):1202. — DOI: 10.3390/nu10091202
- Rosanoff A, Weaver CM, Rude RK (2012). Suboptimal magnesium status in the United States: are the health consequences underestimated? Nutrition Reviews;70(3):153-164. — DOI: 10.1111/j.1753-4887.2011.00465.x
- Gröber U, Schmidt J, Kisters K (2015). Magnesium in Prevention and Therapy. Nutrients;7(9):8199-8226. — DOI: 10.3390/nu7095388
- Schlingmann KP, Weber S, Peters M, et al. (2002). Hypomagnesemia with secondary hypocalcemia is caused by mutations in TRPM6, a new member of the TRPM gene family. Nature Genetics;31(2):166-170. — DOI: 10.1038/ng889
- National Institutes of Health, Office of Dietary Supplements. Magnesium — Fact Sheet for Health Professionals. — ods.od.nih.gov
PubMed Topic Searches
- PubMed — Magnesium supplementation for muscle cramps
- PubMed — Hypomagnesemia, tetany, and neuromuscular excitability
- PubMed — Magnesium for pregnancy leg cramps (randomized trials)
- PubMed — Serum magnesium vs. body stores
- PubMed — Muscle fasciculations: causes and differential diagnosis
Connections
- Magnesium: The Mineral That Makes ATP Work — interactive animation
- Magnesium Deficiency Symptom Hub
- Low Magnesium and Heart Palpitations
- Low Magnesium, Anxiety & Insomnia
- Low Magnesium, Fatigue & Headaches
- Magnesium Overview
- Magnesium and Muscle Function
- Magnesium and Heart Health
- Magnesium and Sleep
- Magnesium and Migraines
- Magnesium Replenishment
- Potassium and Muscle Cramps
- Calcium
- Potassium
- Comprehensive Metabolic Panel
- Arrhythmia
- Heart Palpitations