Hypermagnesemia (High Magnesium): Symptoms, Causes, and Risks
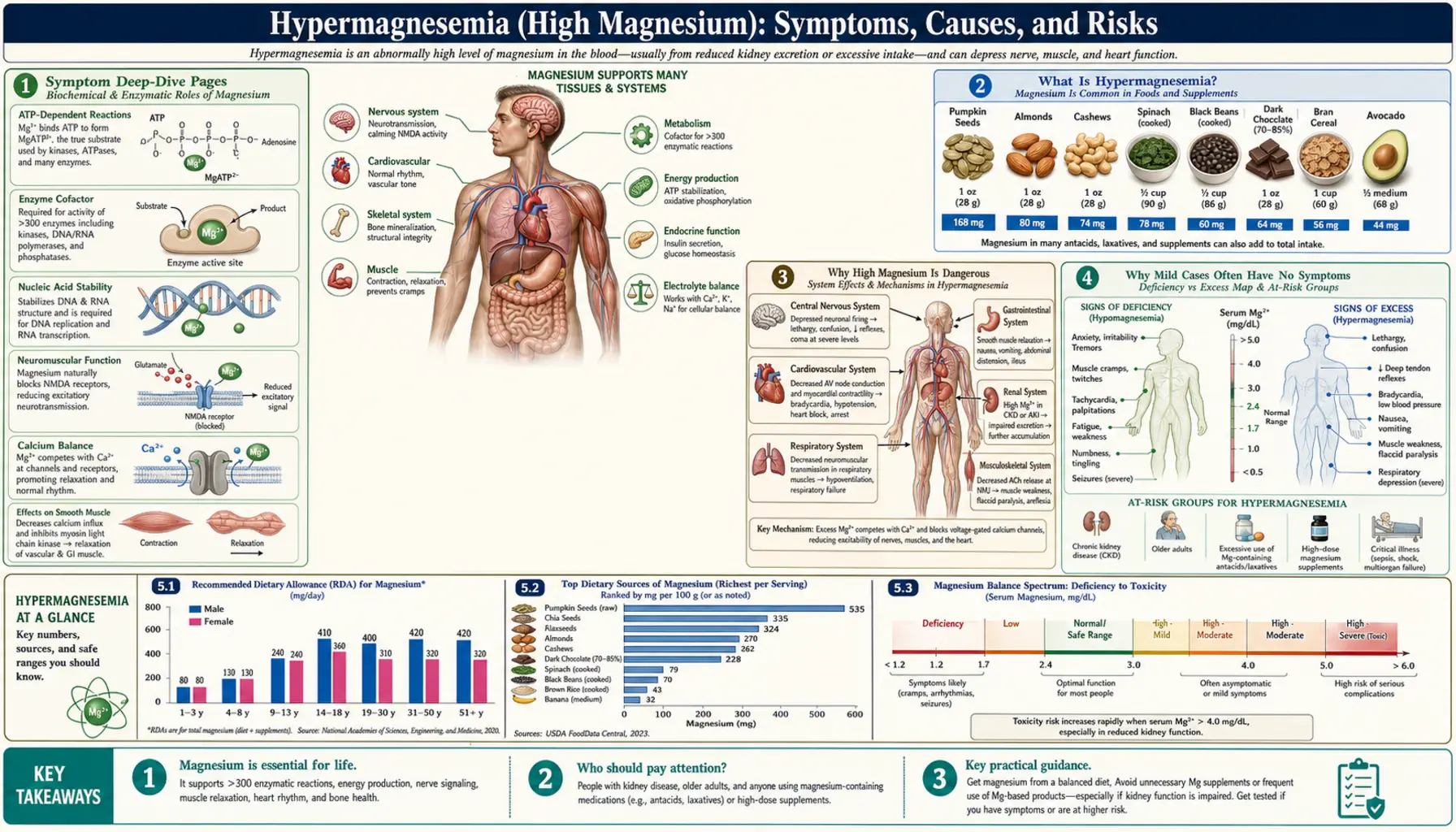
Hypermagnesemia means too much magnesium in the blood — usually defined as a serum level above about 2.5 mg/dL (roughly 1.0 mmol/L), where the normal range is about 1.7–2.4 mg/dL. Here is the single most important thing to understand: in a person with healthy kidneys, high magnesium is genuinely uncommon, because the kidneys are remarkably good at flushing out any excess. Most real cases share two ingredients — reduced kidney function plus a magnesium load the body cannot clear, most often from magnesium-containing laxatives, antacids, or Epsom-salt drinks. When symptoms do appear, the earliest is usually a quiet one a doctor notices before you do: fading deep-tendon reflexes. As the level climbs, magnesium acts like a natural calcium blocker — it relaxes muscle and blood vessels and slows the nerves, so people feel weak and drowsy, flushed and warm, with a low blood pressure and a slow heartbeat. At very high levels it can blunt breathing and the heart's rhythm, which is why severe hypermagnesemia is a medical emergency. This hub explains what hypermagnesemia is, why it is dangerous, why mild cases are so often silent, what causes it, and how it is diagnosed and treated — with deep-dive pages for each symptom it can produce. Do not self-treat a high magnesium level, and if you have kidney disease, treat magnesium laxatives and antacids as something to clear with your doctor first.
Symptom Deep-Dive Pages
Muscle Weakness
Why excess magnesium makes muscles feel heavy and weak by jamming the signal between nerve and muscle, why fading reflexes are an early and important sign, and why this is a clue rather than proof.
Low Blood Pressure & Flushing
How magnesium relaxes blood-vessel walls, lowering blood pressure and producing a warm, flushed feeling, why this can happen with IV magnesium or an overdose, and the many other causes of the same sensations.
Slow Heart Rate
Why high magnesium can slow the heartbeat and depress the heart's electrical conduction, how this differs from the heart effects of high potassium, and when a slow pulse becomes an emergency.
Nausea & Drowsiness
The early stomach upset and sleepy, sedated feeling that often arrive first with rising magnesium, why these symptoms are vague and easy to dismiss, and how they fit alongside the conditions that drive magnesium up.
Interactive Visualization Magnesium — the mineral that makes ATP work Bare ATP is useless and enzymes reject it. Watch magnesium clamp the phosphates and switch it on, plug the NMDA channel, and let a cramping muscle finally let go. Launch →
Table of Contents
- Symptom Deep-Dive Pages
- What Is Hypermagnesemia?
- Why High Magnesium Is Dangerous
- Why Mild Cases Often Have No Symptoms
- Common Causes of High Magnesium
- How Hypermagnesemia Is Diagnosed
- How High Magnesium Is Treated
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Is Hypermagnesemia?
Magnesium is an electrolyte — a mineral that carries an electrical charge in body fluid — and it is one of the busiest minerals you have, acting as a helper in hundreds of enzyme reactions, in muscle and nerve signaling, in keeping the heartbeat steady, and in building bone. Most of your magnesium is stored inside cells and in bone; only about 1% circulates in the blood, which is the part a blood test measures. Hypermagnesemia is the medical word for a blood (serum) magnesium level that is too high — most often defined as a value above about 2.5 mg/dL (roughly 1.0 mmol/L, or about 2.1 mEq/L), sitting just above the normal range of about 1.7 to 2.4 mg/dL. Laboratories report magnesium in several units, which can be confusing; the key point is simply that the value is above the lab's stated upper limit.
The most important fact about hypermagnesemia is what usually has to go wrong for it to happen at all. Healthy kidneys are extraordinarily good at getting rid of extra magnesium — they can ramp up magnesium excretion dramatically, so in a person with normal kidney function it is genuinely difficult to push the blood level high by diet or even by ordinary supplement doses. That is why clinically important hypermagnesemia is considered relatively uncommon, and why most real cases involve two things together: the kidneys are not clearing magnesium well, and a source is delivering more magnesium than the body can handle. Remove either ingredient and the problem usually does not occur.
As with most electrolyte disturbances, how high the level climbs matters a great deal, and the effects tend to appear in a fairly predictable order as magnesium rises. The bands below are approximate — people vary, and the rate of rise and the person's overall health shift the picture — but they capture the general pattern clinicians expect:
- Mild (about 2.5–4 mg/dL) — Often silent. Many people feel nothing, and the value turns up on a routine blood panel. The earliest objective sign a clinician may find is reduced deep-tendon reflexes (the knee-jerk and similar reflexes become sluggish), sometimes with mild nausea, flushing, or a little drowsiness.
- Moderate (about 4–7 mg/dL) — Now symptoms become more likely: noticeable muscle weakness, lethargy and sleepiness, lower blood pressure, a warm flushed feeling, and a slowing heart rate. Reflexes are typically lost in this range.
- Severe (above about 7–12 mg/dL and higher) — A medical emergency. Very high magnesium can depress breathing (the breathing muscles weaken), cause dangerously low blood pressure, profound slowing of the heart and abnormal conduction, and at extreme levels coma, paralysis, and cardiac arrest.
Two honesty notes are worth holding onto. First, these thresholds are guides, not guarantees — some people develop symptoms at lower levels (especially if the magnesium rose quickly), and others tolerate surprisingly high levels with few complaints. Second, because the early symptoms are so vague, the level on the blood test — not how a person feels — is what truly guides how seriously hypermagnesemia is taken.
Why High Magnesium Is Dangerous
If mild hypermagnesemia often causes nothing, why is it taken seriously? Because magnesium, in excess, is a powerful natural calcium antagonist — it gets in the way of calcium throughout the body — and the two systems most sensitive to that interference are the ones you cannot do without: the nerves and muscles that drive breathing, and the heart.
Here is the idea in plain language. Calcium is the trigger that makes nerves release their signaling chemicals and makes muscle fibers contract; think of calcium as the foot on the accelerator. Magnesium sits in the same molecular doorways — the calcium channels — and when there is too much of it, it competes with calcium and effectively eases off that accelerator. At the junction where a nerve tells a muscle to fire, high magnesium blocks the release of acetylcholine (the chemical messenger) and makes the muscle less responsive. The result is a body-wide damping: muscles weaken, reflexes fade, blood-vessel walls relax (so blood pressure falls and the skin flushes warm), the gut slows, and the brain feels sedated.
Two consequences are the real reasons hypermagnesemia can kill, and both follow directly from that "easing off the accelerator" idea:
- Respiratory depression — the most feared complication. Breathing depends on the diaphragm and other muscles contracting on command from the nerves. When magnesium climbs high enough to block neuromuscular transmission, those breathing muscles weaken and the drive to breathe falters. At severe levels this can progress to respiratory failure — the person stops breathing adequately — which is the classic cause of death in magnesium toxicity and the reason severe cases are managed in a hospital with the ability to support breathing.
- Cardiac effects — a slowing, faltering heart. The same calcium-blocking action slows the heart's pacemaker and its electrical conduction. High magnesium tends to produce bradycardia (a slow heart rate), low blood pressure, and conduction delays that can show up on an electrocardiogram (ECG) as a lengthening PR interval and widening QRS; at extreme levels the heart can develop dangerous block or stop entirely. (The deeper dive on this lives on the Slow Heart Rate page; for irregular heartbeats in general see Arrhythmia.)
A useful contrast helps here. People often lump magnesium and potassium together because both are electrolytes that affect the heart, but their dangers differ. Excess potassium destabilizes the heart's electrical rhythm and is dangerous chiefly through arrhythmia (see Hyperkalemia). Excess magnesium is more of a depressant — it slows and quiets nerve, muscle, and heart, with respiratory depression and bradycardia leading the picture. That difference is why the symptoms of high magnesium read as weakness, sleepiness, low pressure, and a slow pulse rather than racing palpitations.
Why Mild Cases Often Have No Symptoms
One of the easiest things to misunderstand about high magnesium is that, when it is mild, it frequently does not feel like anything. A person can have a modestly elevated magnesium level and notice nothing at all, because the body's damping effect is gentle at first and the earliest change — sluggish reflexes — is something a clinician detects with a reflex hammer, not something you feel. When symptoms do appear, the first ones are vague and forgettable: a bit of nausea, a little flushing, feeling unusually sleepy or weak. These are the kinds of complaints anyone might attribute to a poor night's sleep, a virus, or simply getting older — and they have a hundred other explanations.
Why so quiet? Largely because the level usually has to climb a fair way before magnesium's calcium-blocking effects become strong enough to produce obvious trouble. The progression is gradual: reflexes fade first, then weakness and drowsiness and a falling blood pressure, and only at higher levels do the truly dangerous effects on breathing and the heart emerge. The unsettling implication is that the symptoms which would alarm a person tend to arrive after the level is already high — the body is not a reliable early-warning system here.
This is exactly why knowing who is at risk matters more than waiting for symptoms. Because mild hypermagnesemia is quiet and because it essentially only develops when the kidneys cannot keep up with a magnesium load, the people who need to be careful are a fairly specific group:
- Anyone with chronic kidney disease or otherwise reduced kidney function — the single biggest risk factor, because the body's main route for removing magnesium is impaired (see Kidney Disease).
- People with kidney disease who use magnesium-containing laxatives or antacids — common over-the-counter products that quietly deliver a large magnesium load, the classic recipe for trouble.
- Older adults, in whom kidney function declines naturally with age and constipation (often treated with magnesium laxatives) is common — a combination that appears repeatedly in real cases.
- Women receiving intravenous magnesium sulfate in pregnancy (for preeclampsia or to slow preterm labor), who are monitored closely precisely because the dose is deliberately high.
The take-home message is the mirror image of false reassurance: in a healthy person, occasional dietary or modest supplemental magnesium is very safe and the kidneys handle the rest. But if your kidneys are not at full strength, feeling fine is not the same as being fine — and a magnesium-containing product you bought without a second thought can be the missing ingredient that tips the balance.
Common Causes of High Magnesium
Magnesium rises for essentially one of two reasons: the kidneys are not removing enough of it, or something is delivering more than the body can clear — and in most real-world cases, both are true at once. Because healthy kidneys clear magnesium so efficiently, a magnesium load alone rarely does it; reduced kidney function is the quiet partner behind most cases. Here are the causes worth knowing.
- Reduced kidney function / chronic kidney disease — the underlying setup in most cases. The kidneys are the body's main exit route for magnesium, and they can normally increase magnesium excretion enormously. When they are damaged or failing — gradually (chronic kidney disease) or suddenly (acute kidney injury) — that safety valve is impaired and magnesium can accumulate, especially if any extra is coming in. People on dialysis and those with advanced kidney disease are watched most closely.
- Magnesium-containing laxatives — a leading culprit. Many common laxatives and "bowel preps" are magnesium salts: magnesium hydroxide (milk of magnesia), magnesium citrate, magnesium oxide, and magnesium sulfate. They deliver a large magnesium load to the gut, and several factors make absorption worse than expected — a slow or obstructed bowel (constipation, blockage) holds the magnesium in contact with the gut lining longer, and an inflamed gut absorbs more of it. In an older person with constipation and some kidney impairment, a magnesium laxative is the textbook trigger for severe hypermagnesemia, and case reports describe fatal outcomes from exactly this combination.
- Magnesium-containing antacids. Some over-the-counter antacids contain magnesium hydroxide or magnesium carbonate. Used occasionally by a healthy person they are harmless, but taken regularly by someone with reduced kidney function they become a steady, easily-overlooked magnesium source.
- Epsom salts and high-dose supplements. Epsom salt is magnesium sulfate; drinking it (sometimes promoted as a "cleanse" or for constipation) can deliver a very large dose at once. Near-fatal hypermagnesemia has been reported even in people with normal kidneys after a large Epsom-salt ingestion, which shows that a big enough load can overwhelm even healthy kidneys. High-dose oral magnesium supplements can contribute in the same way, particularly when kidney function is reduced.
- Intravenous magnesium in pregnancy. Magnesium sulfate given by vein is a standard, effective treatment for preeclampsia and eclampsia and to protect the preterm infant's brain. Because the dose is intentionally high, mothers are monitored for early signs of toxicity — chiefly the loss of deep-tendon reflexes — so that the infusion can be slowed or stopped before levels become dangerous. This is a recognized, managed source rather than an accident.
- Other, less common sources. Magnesium-containing enemas (especially if retained or given to someone with a damaged bowel) and certain bowel-preparation regimens before colonoscopy or surgery have caused severe hypermagnesemia. Rarely, conditions that reduce magnesium excretion — such as adrenal insufficiency or hypothyroidism — or massive tissue breakdown can nudge levels up.
- Pseudohypermagnesemia / lab artifact — worth a thought. Occasionally a reported value is misleading — for example, hemolysis (red cells breaking down in the sample) or contamination of the sample can raise the measured magnesium. As with any unexpected electrolyte result in someone who feels well and has no risk factors, repeating the test is sometimes the first sensible step.
The practical thread running through all of this is the same: a magnesium source plus impaired clearance. The most common preventable version of the story is an older adult with some kidney impairment reaching for a magnesium laxative or antacid — which is why clinicians ask specifically about over-the-counter products when magnesium comes back high.
How Hypermagnesemia Is Diagnosed
Because mild hypermagnesemia is usually silent, it is most often discovered the same way other electrolyte problems are: on a blood test. Serum magnesium is not always part of the most basic panels, but it is a routine, inexpensive test that is frequently ordered when someone has kidney disease, takes magnesium-containing medicines, is acutely ill, or has unexplained weakness, drowsiness, or a slow heart rate. Many people first learn their magnesium is high not from a symptom but from bloodwork. A Comprehensive Metabolic Panel does not always include magnesium, but it reports kidney function (creatinine) and calcium — both directly relevant — and magnesium is easily added to the same draw.
When a high magnesium value comes back, the clinician's task is to answer three questions: is it real, how urgent is it, and why is it happening. Depending on the level and the situation, the workup may include:
- Confirming the value. An unexpected high result in someone who feels well and has no risk factors may be repeated, partly because sample problems (such as hemolysis) can falsely raise it. Confirming before treating avoids acting on a number that was never truly high.
- A focused physical exam — especially the reflexes. Because the loss of deep-tendon reflexes is one of the earliest and most reliable physical signs of rising magnesium, a clinician will often check the knee-jerk and other reflexes. Diminished or absent reflexes in the right context point strongly toward significant hypermagnesemia and signal that the level is high enough to matter. Blood pressure, heart rate, breathing, and alertness are also assessed.
- Kidney function tests. Creatinine and other markers on the metabolic panel reveal how well the kidneys are working, which usually explains why magnesium accumulated in the first place. Reduced kidney function plus a magnesium source is the pattern clinicians expect.
- An electrocardiogram (ECG / EKG) — a quick, painless tracing of the heart's electrical activity. Because high magnesium can slow the heart and delay conduction, the ECG can show a slow rate, a lengthening PR interval, and a widening QRS at higher levels, helping gauge how much the heart is being affected.
- A careful medication and product history. The clinician will ask specifically about magnesium-containing laxatives, antacids, Epsom-salt drinks, enemas, supplements, and any recent bowel preparation — because these are the usual sources and stopping them is the first step in treatment.
It is also worth knowing that calcium and magnesium are often interpreted together. Low calcium can accompany high magnesium and can amplify some of magnesium's effects, so a clinician frequently looks at both, alongside the kidney numbers, to build the full picture rather than reacting to a single value. For the broader role of calcium in the body, see Calcium.
How High Magnesium Is Treated
Treatment depends on how high the level is, how fast it rose, whether there are symptoms, and how well the kidneys work. This is medical territory, and severe or symptomatic hypermagnesemia is an emergency — there is no safe way to bring a dangerously high magnesium level down at home. The good news is that the first and most powerful step is often simple, and that healthy kidneys do most of the work once the source is removed. The logic of treatment runs in three parts: stop the source, protect the body and clear the excess, and remove magnesium directly when the kidneys cannot.
- Stop the source — the essential first move. Because most hypermagnesemia comes from an outside magnesium load, the single most important step is to stop all magnesium-containing products: laxatives, antacids, Epsom-salt drinks, supplements, enemas, and any magnesium infusion. In mild cases in a person with reasonable kidney function, simply stopping the source and letting the kidneys do their job is often enough, because they clear magnesium quickly once the extra intake ends.
- Protect the heart and neuromuscular system with calcium. In symptomatic or severe cases, intravenous calcium (calcium gluconate or calcium chloride) is given because calcium is magnesium's natural opponent — it directly counteracts magnesium's depressant effect on nerves, muscles, and the heart, working within minutes. Like its role in high potassium, calcium buys time and stabilizes the patient; it does not lower the magnesium level itself, so the next steps still matter.
- Help the kidneys clear it. When the kidneys are working, doctors can encourage magnesium excretion with intravenous fluids and sometimes a loop diuretic (such as furosemide), which increases the amount of magnesium the kidneys flush out. This is effective only insofar as the kidneys can respond.
- Remove magnesium directly with dialysis. When the kidneys cannot do the job — in advanced kidney failure, in people on dialysis, or in severe, refractory cases — hemodialysis is the definitive treatment. It filters magnesium straight out of the blood and can correct dangerous levels quickly. This is the standard route for severe hypermagnesemia in someone with little or no kidney function.
- Support breathing and circulation as needed. Because the gravest danger is respiratory depression, severe cases are managed where breathing can be supported (up to and including mechanical ventilation), and low blood pressure or a dangerously slow heart rate is treated with the appropriate emergency measures while the magnesium is brought down.
The reassuring part is that, caught in time and with the source removed, hypermagnesemia is very treatable — and in people with healthy kidneys it usually resolves on its own once the magnesium load stops. The hard part is prevention in the at-risk group: for anyone with kidney disease, the most effective "treatment" is never developing the problem, which means treating magnesium-containing laxatives, antacids, and high-dose supplements as products to clear with a clinician rather than reach for casually. (This is the opposite situation from the Deficiency side of magnesium, where the goal is to get more in — another reason these decisions belong with someone who knows your kidney function and your level.)
When to Seek Care / Red Flags
Because mild high magnesium is usually silent, the most important "red flag" is often a situation rather than a symptom: if you have kidney disease or reduced kidney function, the right move is to avoid magnesium-containing laxatives, antacids, and high-dose supplements unless your doctor has specifically approved them — and to ask before starting any new over-the-counter product. That said, certain symptoms can mean magnesium is high enough to threaten breathing or the heart. Seek emergency care right away if you (or someone you are caring for) have any of the following, especially in the setting of kidney disease or recent use of a magnesium-containing laxative, antacid, or Epsom-salt drink:
- Trouble breathing — slow, shallow, or weak breathing, or feeling unable to take a full breath. This is the most dangerous sign of magnesium toxicity.
- Severe muscle weakness — especially weakness that is spreading, or difficulty holding up the head, standing, or moving the limbs.
- A very slow or weak pulse, fainting, or near-fainting — signs the heart's rate or output may be affected.
- Profound drowsiness, confusion, or being difficult to wake — a sign the nervous system is being heavily depressed.
- Marked flushing with very low blood pressure — severe warmth and lightheadedness together, particularly after a large magnesium dose.
Milder warning signs — new or worsening nausea, unusual sleepiness, or muscle weakness in someone with kidney disease who has been using a magnesium product — are a reason to stop the product and get checked promptly, even before the more dramatic symptoms appear. A simple blood test settles the question. For related symptoms covered elsewhere on the site, see the deep-dive pages on Muscle Weakness, Slow Heart Rate, and Nausea & Drowsiness, and the general page on Arrhythmia.
Key Research Papers
- Adomako EA, Yu ASL (2024). Magnesium Disorders: Core Curriculum 2024. American Journal of Kidney Diseases;83(6):803-815. — DOI: 10.1053/j.ajkd.2023.10.017
- Aal-Hamad AH, Al-Alawi AM, Kashoub MS, Falhammar H (2023). Hypermagnesemia in Clinical Practice. Medicina;59(7):1190. — DOI: 10.3390/medicina59071190
- Jahnen-Dechent W, Ketteler M (2012). Magnesium basics. Clinical Kidney Journal;5(Suppl 1):i3-i14. — DOI: 10.1093/ndtplus/sfr163
- Tosto F, Magro G, Laterza V, Romozzi M (2025). Neurological manifestations of hypermagnesemia: a narrative review. Acta Neurologica Belgica;125(2):283-298. — DOI: 10.1007/s13760-024-02653-3
- Cheungpasitporn W, Thongprayoon C, Qian Q (2015). Dysmagnesemia in Hospitalized Patients: Prevalence and Prognostic Importance. Mayo Clinic Proceedings;90(8):1001-1010. — DOI: 10.1016/j.mayocp.2015.04.023
- Yamaguchi H, Shimada H, Yoshita K, et al. (2019). Severe hypermagnesemia induced by magnesium oxide ingestion: a case series. CEN Case Reports;8(1):31-37. — DOI: 10.1007/s13730-018-0359-5
- Khairi T, Amer S, Spitalewitz S, Alasadi L (2014). Severe Symptomatic Hypermagnesemia Associated with Over-the-Counter Laxatives in a Patient with Renal Failure and Sigmoid Volvulus. Case Reports in Nephrology;2014:560746. — DOI: 10.1155/2014/560746
- Si GF, Ge YX, Lv XP, et al. (2024). Case report: Near-fatal hypermagnesemia resulting from the use of Epsom salts in a patient with normal renal function. Frontiers in Medicine;11:1416956. — DOI: 10.3389/fmed.2024.1416956
- Uematsu M, Imaizumi T, Tanaka S, et al. (2025). Risk of hypermagnesemia in patients with eating disorders taking magnesium oxide preparations: a retrospective study. Eating and Weight Disorders;30(1):24. — DOI: 10.1007/s40519-025-01796-3
- Topf JM, Murray PT (2003). Hypomagnesemia and hypermagnesemia. Reviews in Endocrine and Metabolic Disorders;4(2):195-206. — PubMed
- National Institutes of Health, Office of Dietary Supplements. Magnesium — Health Professional Fact Sheet (Upper Intake Levels and excess magnesium). — NIH Office of Dietary Supplements
PubMed Topic Searches
- PubMed — Hypermagnesemia: causes, diagnosis, and management
- PubMed — Hypermagnesemia, magnesium laxatives, and renal failure
- PubMed — Hypermagnesemia, neuromuscular block, and respiratory depression
- PubMed — Magnesium sulfate toxicity in preeclampsia and reflex monitoring
- PubMed — Treatment of hypermagnesemia (calcium, dialysis)
Connections
- Magnesium: The Mineral That Makes ATP Work — interactive animation
- Hypermagnesemia: Muscle Weakness
- Hypermagnesemia: Low Blood Pressure & Flushing
- Hypermagnesemia: Slow Heart Rate
- Hypermagnesemia: Nausea & Drowsiness
- Magnesium Overview
- Hypomagnesemia (Low Magnesium) Hub
- Magnesium Benefits Hub
- Calcium
- Potassium Overview
- Hyperkalemia (High Potassium) Hub
- Kidney Disease
- Comprehensive Metabolic Panel
- Arrhythmia
- Heart Palpitations