Migraine
Interactive Visualization Nerve Impulse — fire an action potential Watch it race down the axon: sodium rushing in, potassium out, a live voltage trace spiking, and neurotransmitter crossing the synapse. Launch → Interactive Visualization Pain & the Gate Control — close the gate yourself Fire a pain signal up the spinal cord — then rub the skin and watch the gate close, or release endorphins and see the same signal fade before it ever reaches the brain. Launch → Interactive Visualization Balance & Vertigo — spin the inner ear Turn and tilt your head and watch the inner-ear canals and otoliths fire your sense of balance — then knock a crystal loose to trigger BPPV vertigo, and roll it back out with the Epley manoeuvre. Launch → Interactive Visualization Why Chili Burns — hijack your heat receptor Discover that chili isn't hot — it hijacks your heat receptor to fake a burn — then reach for water and fail, milk and succeed, and see how the same trick turns nerve pain down in a capsaicin cream. Launch → Interactive Visualization What Happens in a Migraine Ride the wave of cortical spreading depression, watch the trigeminal nerve dump CGRP and inflame the meninges — then block CGRP and calm the throb. Launch →
Table of Contents
- What is Migraine?
- Migraine Phases
- Common Triggers
- Types of Migraine
- Acute Treatments
- Preventive Treatments
- Lifestyle and Self-Care
- Research Papers
- Connections
- Featured Videos
What is Migraine?
Migraine is a chronic neurovascular disorder characterized by recurrent attacks of moderate-to-severe, often unilateral, throbbing headache lasting 4–72 hours, typically accompanied by nausea, vomiting, and sensitivity to light (photophobia) and sound (phonophobia). It is far more than “a bad headache”: migraine is a disabling neurological disease driven by abnormal sensory processing in the brain, with rich genetic and hormonal underpinnings.
Migraine affects roughly 12% of adults worldwide, with a striking female-to-male ratio of about 3:1 during reproductive years, largely reflecting the role of estrogen fluctuations. The World Health Organization ranks migraine among the leading causes of years lived with disability globally.
Clinicians divide migraine into two broad patterns based on attack frequency:
- Episodic migraine: fewer than 15 headache days per month.
- Chronic migraine: 15 or more headache days per month for at least 3 months, with at least 8 of those days meeting full migraine criteria. Chronic migraine often evolves out of episodic migraine and frequently coexists with medication-overuse headache.
Migraine Phases
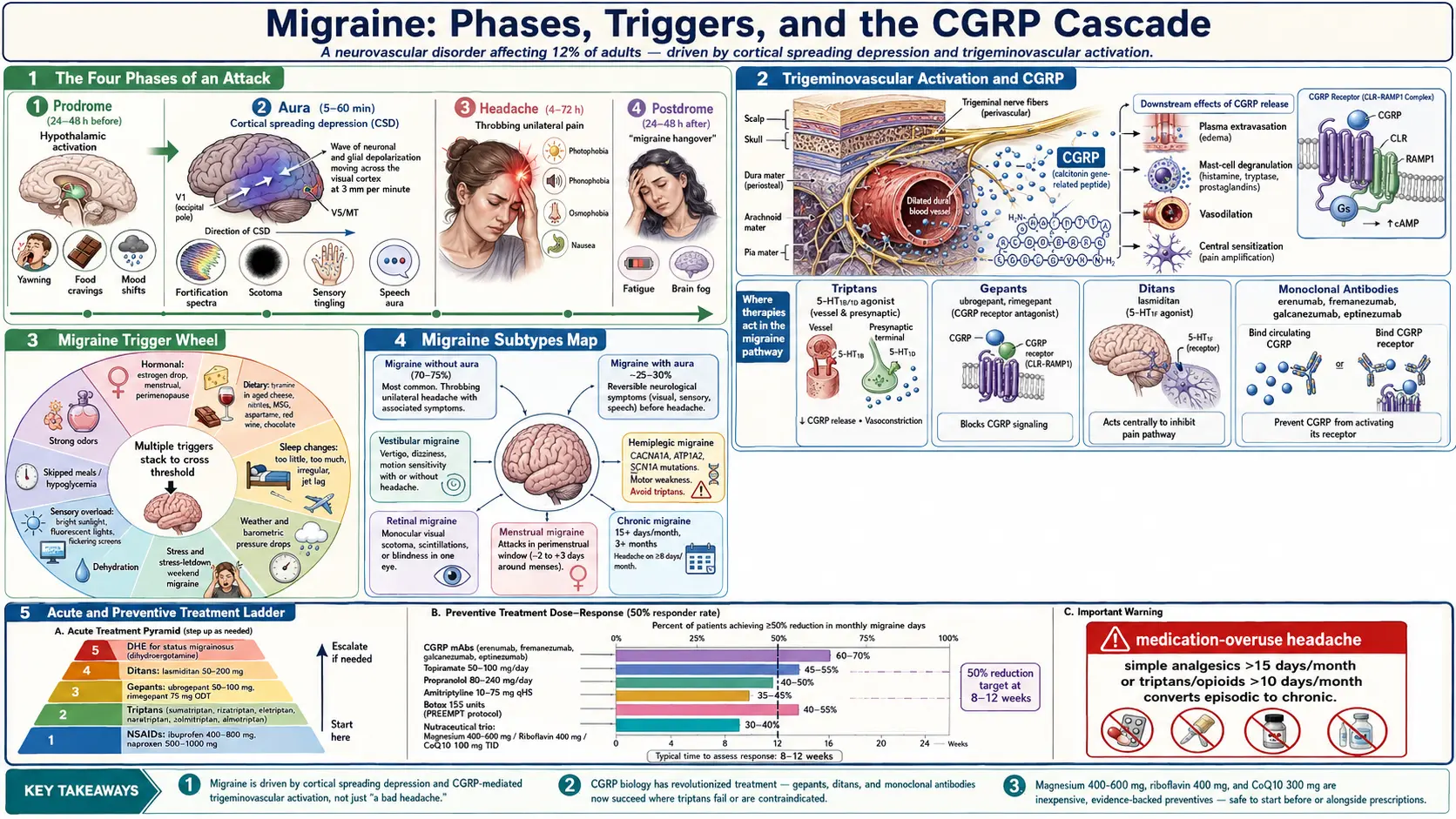
A migraine attack is not a single event but an evolving process that can unfold across four distinct phases. Not every patient experiences every phase, but recognizing them helps target treatment earlier and more effectively.
1. Prodrome (24–48 hours before)
- Subtle premonitory symptoms: yawning, food cravings, mood changes (irritability or euphoria), neck stiffness, increased thirst or urination, fatigue, difficulty concentrating.
- Driven by hypothalamic activation; many patients learn to recognize these signals as a warning to take preventive action.
2. Aura (5–60 minutes)
- Occurs in roughly 25–30% of migraine sufferers.
- Visual aura is most common: shimmering zigzag lines (fortification spectra), blind spots (scotomas), or flashing lights that gradually expand across the visual field.
- Sensory aura: tingling or numbness spreading up an arm and into the face.
- Speech aura: word-finding difficulty, slurred speech.
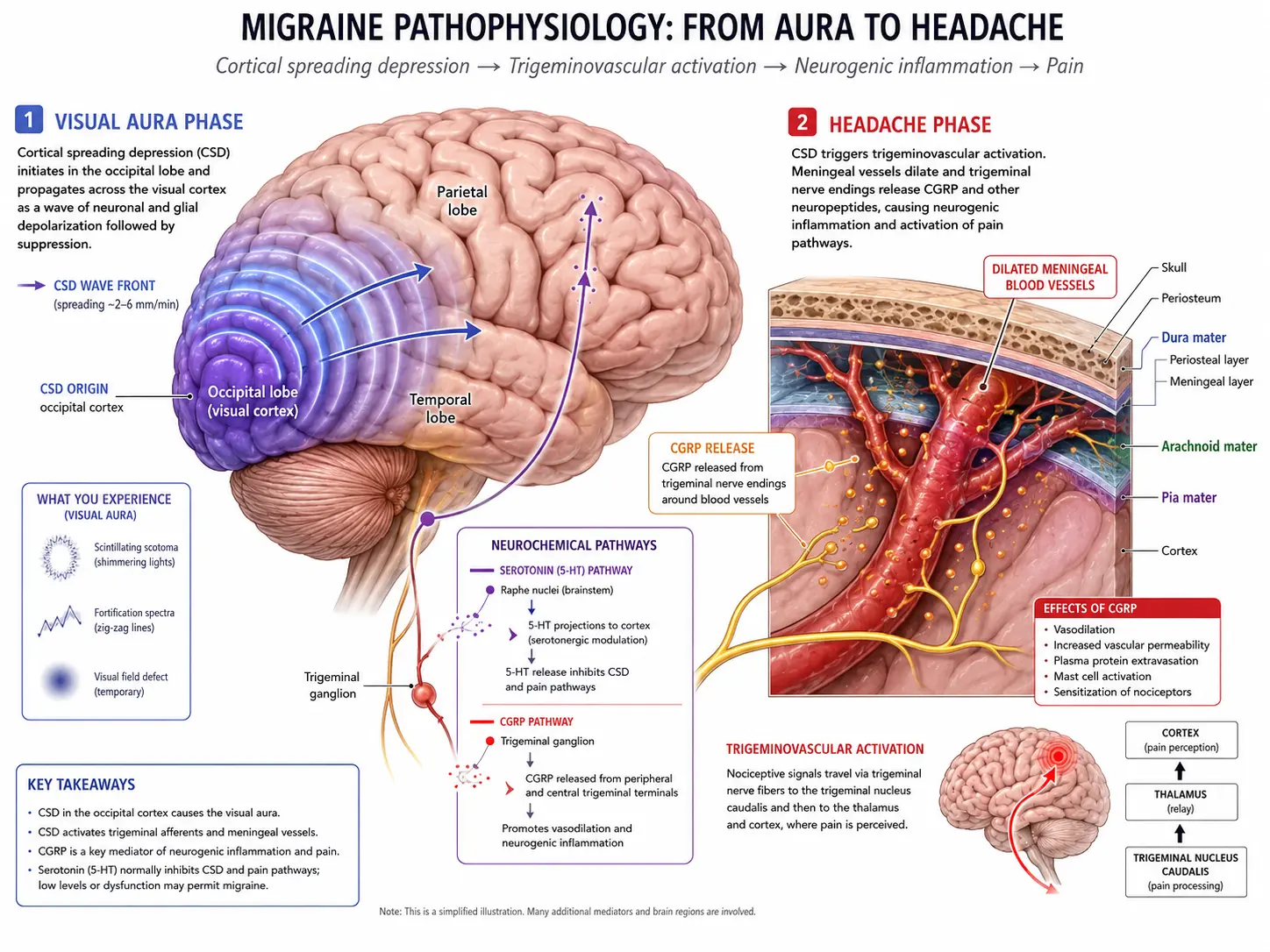
- Caused by cortical spreading depression (CSD) — a slow wave of neuronal and glial depolarization (about 3 mm per minute) sweeping across the cortex, followed by suppressed activity. CSD is shown spreading across the cortex in the first illustration above.
3. Headache (4–72 hours)
- Throbbing or pulsating pain, typically unilateral, often centered behind one eye or temple.
- Accompanied by nausea, vomiting, photophobia, phonophobia, and osmophobia (sensitivity to smells).
- Worsened by routine physical activity; many patients seek a dark, quiet room.
- Driven by activation of the trigeminovascular system: trigeminal nerve fibers innervate cranial blood vessels and the meninges, releasing inflammatory neuropeptides — especially calcitonin gene-related peptide (CGRP) — that produce vasodilation, plasma protein extravasation, and central sensitization.
4. Postdrome (24–48 hours after)
- Often called the “migraine hangover”.
- Fatigue, cognitive slowness (“brain fog”), mood depression or elation, residual mild head tenderness.
- Reflects gradual normalization of brain network activity after the attack.
Common Triggers
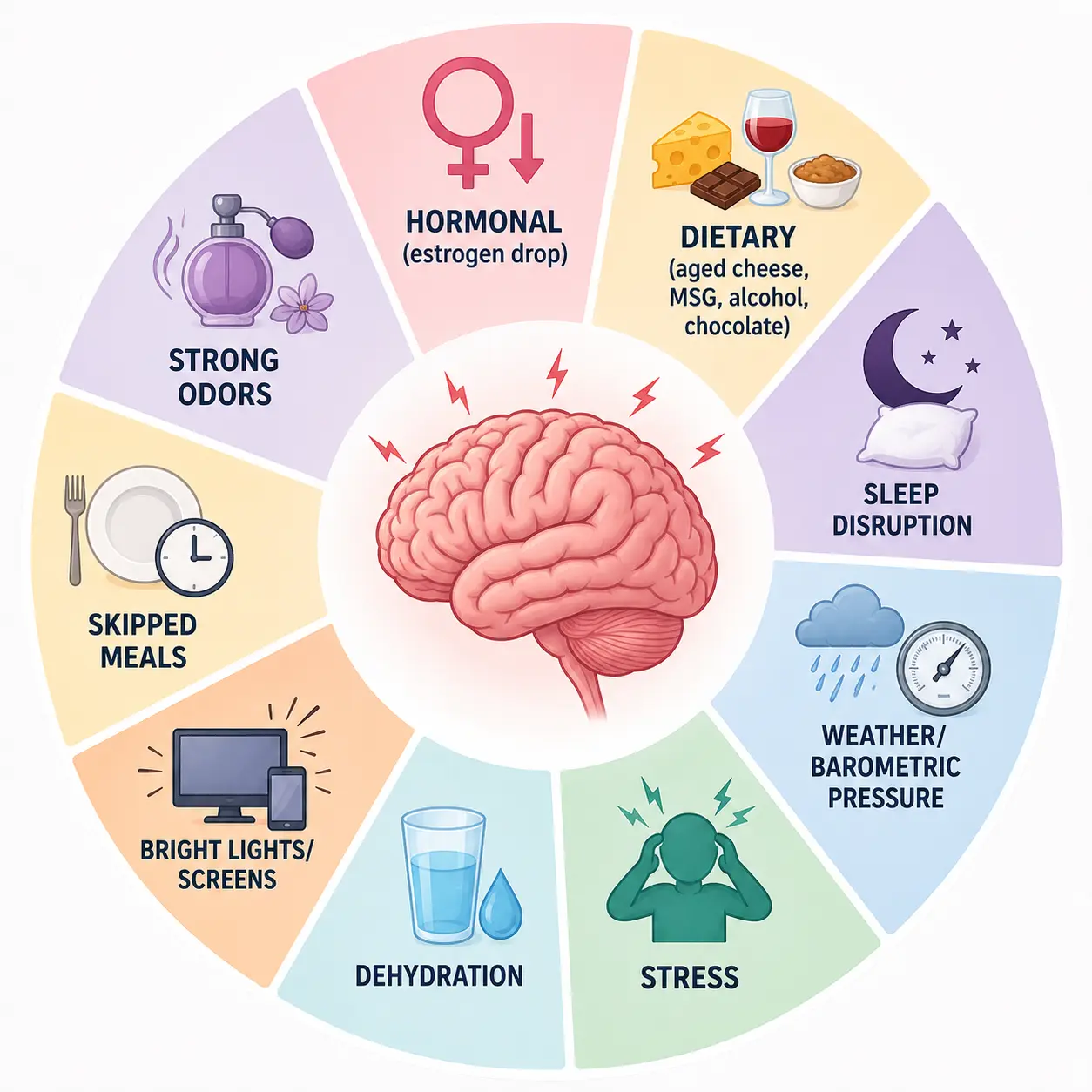
Triggers do not cause migraine on their own — they tip an already vulnerable nervous system over its threshold. Most patients have multiple triggers that interact, and the same exposure may or may not provoke an attack depending on hormones, sleep, and stress at the time. The triggers wheel above summarizes the most common categories. A headache diary (tracking foods, sleep, cycle day, weather, stress, attack onset) is the single best tool for identifying personal triggers.
- Hormonal: the drop in estrogen just before menstruation is one of the most reliable triggers (menstrual migraine). Perimenopause, ovulation, and the placebo week of combined oral contraceptives can also provoke attacks.
- Dietary: aged cheeses (tyramine), processed meats with nitrites/nitrates, monosodium glutamate (MSG), aspartame, alcohol — especially red wine — chocolate, and for some people caffeine (both excess and withdrawal).
- Sleep changes: too little sleep, too much sleep, irregular sleep timing, jet lag, and shift work all elevate risk.
- Weather and barometric pressure: rapid pressure drops (storm fronts), high heat and humidity, dry hot winds.
- Stress and stress letdown: attacks frequently strike on the first day off after a stressful workweek (the “weekend migraine”), reflecting cortisol rebound.
- Dehydration: even mild fluid deficit can lower the migraine threshold.
- Sensory overload: bright sunlight, fluorescent lights, flickering screens, loud noise.
- Skipped meals and hypoglycemia: long fasting windows, especially for sensitive individuals.
- Strong odors: perfume, cleaning products, gasoline, cigarette smoke.
Types of Migraine
Migraine Without Aura
- The most common form (about 70–75% of migraine).
- Throbbing, often one-sided headache with nausea, photophobia, and phonophobia, but no neurological warning symptoms.
Migraine With Aura
- Reversible visual, sensory, or speech disturbances precede or accompany the headache.
- Aura with brainstem features (vertigo, dysarthria, double vision) was historically called “basilar migraine”.
- Migraine with aura is associated with a small but real increase in stroke risk, especially in women who smoke or use estrogen-containing contraceptives.
Vestibular Migraine
- Recurrent episodes of vertigo, imbalance, or motion sensitivity lasting minutes to days, with or without headache.
- One of the most common causes of recurrent dizziness in adults; often misdiagnosed as inner-ear disease.
Hemiplegic Migraine
- Aura includes temporary one-sided weakness or paralysis, sometimes mimicking a stroke.
- Can be sporadic or familial (autosomal dominant mutations in CACNA1A, ATP1A2, SCN1A).
- Triptans and ergots are typically avoided in this subtype because of theoretical vasoconstriction risk.
Retinal Migraine
- Repeated attacks of monocular visual disturbance (one eye only) — scintillations, scotoma, or temporary blindness lasting under an hour — followed by headache.
- Rare; requires careful workup to exclude vascular and ocular causes.
Chronic Migraine
- Headache on 15 or more days per month for at least 3 months, with migraine features on at least 8 of those days.
- Major risk factors for transformation from episodic to chronic: medication overuse, obesity, depression, sleep apnea, and frequent caffeine use.
Menstrual Migraine
- Attacks reliably tied to the perimenstrual window (2 days before through 3 days after menstruation onset).
- Often longer, more severe, and more refractory to acute treatment than non-menstrual attacks.
- Short-term “mini-prophylaxis” with NSAIDs, long-acting triptans, or magnesium around the cycle can reduce frequency.
Acute Treatments
The goal of acute (abortive) treatment is to stop an attack early, restore function within 2 hours, and avoid a recurrence within 24 hours. Treating at the first sign of pain is consistently more effective than waiting.
- NSAIDs: ibuprofen 400–800 mg, naproxen 500–1000 mg, diclofenac potassium 50 mg sachets, ketorolac. First line for mild-to-moderate attacks; effective and inexpensive.
- Triptans (5-HT1B/1D agonists): sumatriptan, rizatriptan, eletriptan, zolmitriptan, almotriptan, naratriptan, frovatriptan. They constrict cranial vessels and inhibit trigeminal neuropeptide release. Available as tablets, dissolving wafers, nasal sprays, and subcutaneous injection. Avoid in uncontrolled hypertension, coronary artery disease, and hemiplegic or retinal migraine.
- Gepants (small-molecule CGRP receptor antagonists): ubrogepant 50–100 mg and rimegepant 75 mg ODT. No vasoconstriction, so they are safe in patients with cardiovascular disease who cannot take triptans. Rimegepant doubles as both an acute and a preventive agent.
- Ditans (selective 5-HT1F agonists): lasmiditan 50–200 mg. Centrally acting, no vasoconstriction. Causes dose-dependent dizziness; patients are advised not to drive for 8 hours after dosing.
- Anti-emetics: metoclopramide and prochlorperazine treat nausea and also have intrinsic anti-migraine activity, especially when given parenterally in the emergency department.
- Dihydroergotamine (DHE): nasal spray, subcutaneous, intramuscular, or intravenous. Useful for prolonged or refractory attacks and for breaking medication-overuse cycles in inpatient settings.
- Status migrainosus (a debilitating attack lasting more than 72 hours): typically managed in urgent care with intravenous fluids, IV NSAIDs (ketorolac), IV anti-emetics (metoclopramide, prochlorperazine), IV magnesium sulfate 1–2 g, IV valproate, or DHE protocols. A short oral steroid taper may prevent recurrence.
Beware medication-overuse headache: regularly taking simple analgesics on more than 15 days per month, or triptans/opioids/combination analgesics on more than 10 days per month, can drive episodic migraine into a chronic, harder-to-treat pattern.
Preventive Treatments
Daily preventive therapy is appropriate when migraine occurs on 4 or more days per month, when attacks are disabling despite good acute treatment, when acute drugs are contraindicated, or when medication overuse is emerging. The goal is at least a 50% reduction in monthly headache days, fewer disability hours, and less reliance on rescue medication. Most preventives need 8–12 weeks at target dose before being judged.
- CGRP monoclonal antibodies (migraine-specific, monthly or quarterly injection): erenumab (anti-receptor), fremanezumab, galcanezumab, and eptinezumab (IV every 3 months). Generally well tolerated; constipation and injection-site reactions are the most common adverse effects. Often effective within the first month.
- Topiramate: 50–100 mg/day. Effective but limited by cognitive slowing (“dopamax”), paresthesias, weight loss, and a small risk of kidney stones; avoid in pregnancy.
- Beta-blockers: propranolol 80–240 mg/day, metoprolol, timolol. Especially useful when migraine coexists with hypertension, anxiety, or essential tremor.
- Tricyclic antidepressants: amitriptyline 10–75 mg at bedtime. Particularly helpful when migraine coexists with insomnia, tension-type headache, or chronic pain.
- Venlafaxine: an SNRI used at 75–150 mg/day; useful in patients who also have anxiety, depression, or vasomotor menopausal symptoms.
- Onabotulinumtoxin A (Botox): FDA-approved for chronic migraine. The PREEMPT protocol delivers 155 units across 31–39 sites in the head and neck every 12 weeks.
- Magnesium: 400–600 mg/day of magnesium glycinate or citrate. Multiple randomized trials show modest reduction in attack frequency, particularly in menstrual migraine and migraine with aura. Diarrhea is the main dose-limiting effect.
- Riboflavin (vitamin B2): 400 mg/day. Supports mitochondrial energy metabolism; improves migraine frequency in 8–12 weeks. Turns urine bright yellow but is otherwise extremely safe.
- Coenzyme Q10: 100 mg three times daily. A mitochondrial cofactor; randomized trials show reduced migraine frequency over 3 months.
- Other options in selected cases: candesartan, lisinopril, valproate (avoided in women of childbearing potential), flunarizine (where available), and the oral CGRP-receptor antagonists atogepant and rimegepant.
Lifestyle and Self-Care
Lifestyle is not a substitute for medical care, but consistent daily habits raise the migraine threshold and amplify the benefit of any pharmacologic plan. Many patients are able to reduce attack frequency substantially with the following measures:
- Regular sleep: same wake time and bedtime every day, including weekends. Aim for 7–9 hours. Treat snoring and obstructive sleep apnea aggressively — untreated apnea is a strong driver of chronic migraine.
- Hydration: roughly 2–3 liters of water per day, more in heat or with exercise. Adding a pinch of salt or an electrolyte tablet helps in hot climates.
- Headache diary: record date, time, severity, suspected triggers, menstrual cycle day, sleep, foods, weather, and medications used. Apps and paper diaries both work; review monthly with your clinician to identify personal patterns.
- Regular meals: avoid skipping meals or long fasting windows; protein at breakfast helps stabilize morning blood sugar.
- Aerobic exercise: 30–40 minutes of moderate cardio (brisk walking, cycling, swimming) 3–5 times per week reduces attack frequency in randomized trials — comparable in effect size to topiramate.
- Stress management: cognitive behavioral therapy, biofeedback, mindfulness-based stress reduction, and progressive muscle relaxation all have evidence in migraine prevention.
- Mineral and vitamin support: magnesium 400–600 mg/day, riboflavin 400 mg/day, and CoQ10 100 mg three times daily are inexpensive, well tolerated, and have randomized-trial support; they are reasonable to start before or alongside prescription preventives.
- Caffeine discipline: keep daily intake modest and consistent; sudden withdrawal is a classic Saturday-morning trigger.
- Limit screen glare: anti-glare overlays, blue-light filters in the evening, and FL-41 tinted lenses help photophobic patients.
Research Papers
The following PubMed topic searches return current peer-reviewed literature relevant to this condition. Each link opens a live PubMed query.
- Cortical spreading depression migraine
- CGRP monoclonal antibodies migraine
- Triptans efficacy migraine
- Gepants ubrogepant rimegepant
- Lasmiditan ditans migraine
- Botulinum toxin chronic migraine
- Magnesium migraine prophylaxis
- Riboflavin migraine
- CoQ10 migraine
- Hormonal estrogen migraine
- Vestibular migraine
- Chronic migraine medication overuse
Connections
- Migraine: History and Discovery — the long backstory to the treatments on this page — hemicrania in antiquity, Liveing’s nerve-storm, Wolff’s vascular theory, cortical spreading depression, and the trigeminovascular and CGRP turn that produced the modern drugs.
- What Happens in a Migraine — interactive animation
- Why Chili Burns: Capsaicin & the TRPV1 Heat Sensor — interactive animation
- Balance & the Inner Ear: Vertigo & BPPV — interactive animation
- Pain, the Gate Control & Why Rubbing Helps — interactive animation
- Nerve Impulse — interactive animation
- Magnesium
- Vitamin B2 (Riboflavin)
- Anxiety
- Insomnia
- Vitamin D3
- Sleep Hygiene
- Anti-Inflammatory Diet
- Gut-Brain Axis
- PTSD
- Depression
- Headache
- Stress Management
- Magnesium Glycinate
- Dizziness
- Ginger
- Nausea Vomiting
- MSG
- Sulfites
- Trigeminal Neuralgia
- PMS and PMDD