Insomnia
Interactive Visualization Sleep Stages & Your Body Clock — run a whole night Watch deep sleep and REM cycle through the night — then add late-night light, an afternoon coffee, or a nightcap and see what breaks. Launch → Interactive Visualization Caffeine, Adenosine & Why Coffee Stops Working Caffeine doesn’t give you energy — it blocks the tiredness signal while adenosine keeps piling up behind the blockade. Move your coffee to 2 p.m. and watch your deep sleep vanish. Launch → Interactive Visualization GABA, the Brain's Brake — press it with a benzo or alcohol Watch glutamate try to fire a neuron while GABA slams the chloride brake on — then add a benzodiazepine or alcohol and see the brake amplified, and why stacking them is dangerous. Launch → Interactive Visualization Melatonin & the Body Clock — reset your clock with light Let darkness raise melatonin and open the gate to sleep — then shine a screen at night to suppress it and delay your clock, fly across time zones for jet lag, or reset it with well-timed light. Launch →
Table of Contents
- Overview
- Do You Actually Have Insomnia?
- How Common Is It?
- Why Insomnia Persists
- Causes, Comorbidities & Medications
- Screen for What Mimics or Drives It
- Sleep Hygiene: Necessary but Not Sufficient
- CBT-I: The First-Line Treatment
- Medication: An Honest Assessment
- Alcohol, Cannabis & Over-the-Counter Sleep Aids
- Special Situations
- Insomnia and Mental Health
- Tests and Sleep Studies
- Consequences of Untreated Insomnia
- What to Expect
- When to Seek Medical Care
- Recent Research and Advances
- References & Research
- Connections
- Featured Videos
1. Overview
Insomnia is persistent difficulty falling asleep, staying asleep, or waking earlier than you want to — despite having a fair chance to sleep — and feeling the consequences during the day. It is the most common sleep disorder in the world, and one of the most frustrating things a person can live with, because the harder you try to fix it the worse it tends to get.
If you take one thing away from this page, take this:
The first-line treatment for chronic insomnia is not a sleeping pill. It is a structured behavioural therapy called CBT-I — Cognitive Behavioural Therapy for Insomnia. This is not a fringe or alternative position. It is the explicit recommendation of the American College of Physicians, the American Academy of Sleep Medicine, and the European Sleep Research Society — every major guideline body puts CBT-I ahead of medication, as the thing you should try first. Yet most people with insomnia have never heard of it, and are offered a prescription instead. That gap between what the evidence says and what actually happens in clinics is the single biggest problem in this field.
CBT-I works about as well as sleeping pills in the short term, works better in the long term, and — crucially — the benefit keeps working after you stop doing it. Medication only works while you are taking it. That difference is the whole ballgame.
The second thing worth knowing is that insomnia is now understood as a condition in its own right, not merely a symptom of something else. For most of the twentieth century, doctors were taught to treat insomnia as "secondary" — fix the depression, or the pain, or the stress, and the sleep would follow. That model has been abandoned. Insomnia develops its own self-sustaining machinery, and once it has, it will happily carry on long after whatever started it has gone. It needs to be treated as its own target, at the same time as anything else that is going on.
2. Do You Actually Have Insomnia?
Insomnia is a clinical diagnosis made from your story. There is no blood test for it, and — for straightforward cases — no sleep study is needed either. Both the DSM-5 and the International Classification of Sleep Disorders (ICSD-3) define chronic insomnia disorder the same way. You need all of the following:
- A sleep problem — difficulty initiating sleep (taking more than about 30 minutes to fall asleep), difficulty maintaining sleep (waking in the night and struggling to get back off), or waking too early and not being able to return to sleep.
- At least 3 nights per week.
- For at least 3 months. Under three months, it is called short-term or acute insomnia, and most of it resolves on its own.
- Despite adequate opportunity to sleep. This is the clause people miss, and it matters enormously. If you are only allowing yourself five hours in bed because of a night shift, a newborn, or a commute, you are sleep-deprived — which is a different problem with a different solution. Insomnia means you have the time and the conditions to sleep, and still cannot.
- Daytime consequences. Fatigue, low mood or irritability, trouble concentrating or remembering, reduced motivation, more mistakes and near-misses, strain at work or at home. Sleeping "badly" with no daytime cost is not a disorder — some people simply need less sleep than the mythical eight hours.
A useful self-check is the Insomnia Severity Index (ISI), a free 7-question questionnaire scored 0–28: 0–7 no clinically significant insomnia, 8–14 subthreshold, 15–21 moderate, 22–28 severe. It is the standard outcome measure in clinical trials, and it is a good way to track whether treatment is actually working rather than relying on the impression left by last night.
One important distinction: tired versus sleepy
People with insomnia are usually fatigued but not sleepy. They feel wrung-out, foggy, and depleted — yet if you sat them in a quiet room at 2 p.m. and told them to nap, they often could not. That is the signature of insomnia, and it is a clue to the underlying biology (see Why Insomnia Persists).
If instead you are genuinely sleepy — nodding off in meetings, in front of the TV, or, alarmingly, at the wheel — that points away from plain insomnia and towards something like obstructive sleep apnoea or narcolepsy. That distinction changes the whole workup, and it is why clinicians ask about it.
3. How Common Is It?
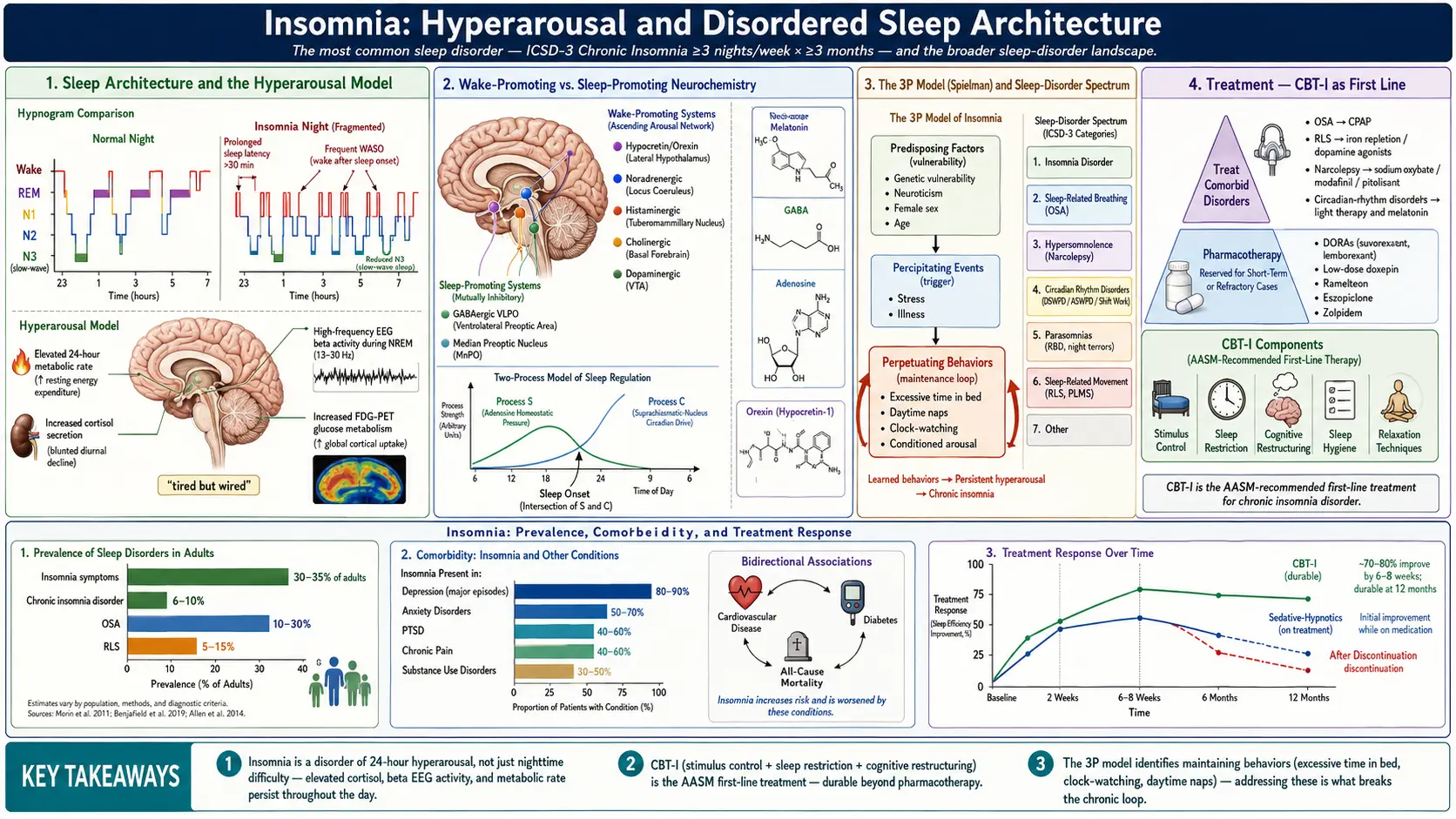
Roughly 30–35% of adults report insomnia symptoms at any given time. About 6–10% meet the full criteria for chronic insomnia disorder, with the daytime impairment that goes with it. So if it feels like everyone you know complains about sleep but you seem to be suffering more than they are — both of those things are true.
- Women are affected roughly 1.4 times as often as men, and the gap widens after menopause.
- Older adults report it far more often (up to 30–48% of people over 65), though a good deal of that reflects accumulated illness, pain, and medication rather than age itself.
- Shift workers run at 25–35%.
- Mental health overlap is large. Around 40–60% of people with chronic insomnia also have a psychiatric condition — most often depression or anxiety. Running the other way, insomnia shows up in 80–90% of depressive episodes.
Despite being this common, insomnia remains badly under-treated — and, when it is treated, it is usually treated with the second-line option (a drug) rather than the first-line one (CBT-I).
4. Why Insomnia Persists
The two-process model: sleep pressure versus the body clock
Normal sleep is the product of two systems pulling against each other. Process S is homeostatic sleep pressure: the longer you are awake, the more adenosine accumulates in the brain, and the heavier the pull toward sleep. Sleeping clears it out and resets the gauge. Caffeine works by blocking adenosine receptors — it does not give you energy, it hides the sleep pressure you have already built up. Process C is the circadian alerting signal from the suprachiasmatic nucleus, the body clock in the hypothalamus, which is set primarily by light hitting the retina. It rises and falls on a roughly 24-hour cycle and actively pushes against sleep at certain times of day — including a "forbidden zone" in the early evening when it is genuinely hard to fall asleep no matter how tired you are.
Good sleep happens when high sleep pressure lines up with a falling circadian alerting signal. Insomnia happens when that alignment breaks — or when something else overrides both. You can watch these two processes interact, and see exactly what caffeine and alcohol do to them, in the interactive sleep and body-clock animation.
Hyperarousal: "tired but wired"
The best-supported explanation for chronic insomnia is hyperarousal — the nervous system is running hot, not just at bedtime but around the clock. This is not a figure of speech; it is measurable. People with chronic insomnia show a higher 24-hour metabolic rate, elevated evening cortisol, a raised core body temperature at sleep onset, altered heart-rate variability, and — most tellingly — excess high-frequency beta activity on EEG during sleep itself, the same brainwave pattern that characterises being awake. Parts of the brain are, in effect, refusing to fully clock off.
This explains the central paradox that patients describe and that no one believes: exhausted all day, wide awake the moment the light goes out. It also explains why a drug that simply forces sedation does not cure anything — it sedates over the top of the hyperarousal without touching it, which is why the insomnia is still there when the drug is stopped.
Conditioned arousal: your bed has been trained against you
Here is a question worth sitting with: have you ever fallen asleep instantly on the sofa, then found yourself completely alert the moment you got into bed?
If so, you have experienced conditioned arousal — plain classical conditioning, the Pavlov's-dogs kind. After enough nights of lying in bed awake, frustrated, and clock-watching, the bed and bedroom stop being cues for sleep and become cues for wakefulness and anxiety. Your brain has learned the association, and it learned it exactly the way you would expect it to. This is not a character flaw or a lack of willpower. It is a trained reflex — and, importantly, one that can be untrained. That is precisely what the stimulus control component of CBT-I is for.
The 3P model — and the insight that changes everything
Arthur Spielman's 3P model is the most useful framework for understanding why one person shrugs off a rough fortnight and another is still not sleeping three years later:
- Predisposing factors — what you brought to the table. A genetic tendency toward hyperarousal (heritability is estimated at 31–58%), a temperament that runs to worry, perfectionism, or rumination, and being female.
- Precipitating factors — what set it off. Bereavement, redundancy, a diagnosis, a divorce, a new baby, a house move, a shift-pattern change. Something happened, and you stopped sleeping. This part is normal; almost everyone has had it.
- Perpetuating factors — what is keeping it going now. Sensible-seeming compensations: going to bed early to "catch up," lying in bed awake hoping sleep will come, napping, cancelling evening plans to conserve energy, checking the clock at 3 a.m. and calculating how many hours are left, and lying there dreading the coming day.
The key insight — and it is the one that reframes the entire problem — is that what is maintaining your insomnia today is usually not what started it.
The divorce is finalised. The grief has softened. The stressful project shipped months ago. And you still are not sleeping — which feels inexplicable and often makes people conclude something is deeply wrong with them. Nothing is deeply wrong with them. What happened is that the original trigger has faded, and the coping behaviours you sensibly adopted to survive it have quietly taken over as the engine of the problem.
Every one of those compensations is rational in the moment and destructive over time. Extra time in bed dilutes your sleep pressure across more hours, so sleep becomes shallower and more broken. Napping bleeds off the very drive you need at 11 p.m. Lying awake in bed is a conditioning trial that trains your brain to associate the mattress with alertness. Clock-watching converts a neutral 3 a.m. awakening — which good sleepers also have, and simply roll over and forget — into an adrenaline-releasing emergency.
This is genuinely good news, and it is worth pausing on. It means you do not have to undo the past to sleep again. You cannot un-grieve the bereavement or un-happen the redundancy. But you can absolutely change what you are doing between 10 p.m. and 7 a.m. — and that is the part that is actually holding the insomnia in place. That is the whole rationale for CBT-I, and it is why it works.
5. Causes, Comorbidities & Medications
Conditions that commonly travel with insomnia
Most clinical insomnia sits alongside something else. Treat both — do not wait for one to fix the other.
- Depression — classically causes early-morning waking as well as trouble getting off. Insomnia often precedes the mood change by weeks and is frequently the first symptom people notice.
- Anxiety — racing thoughts and anticipatory worry are engines of sleep-onset insomnia.
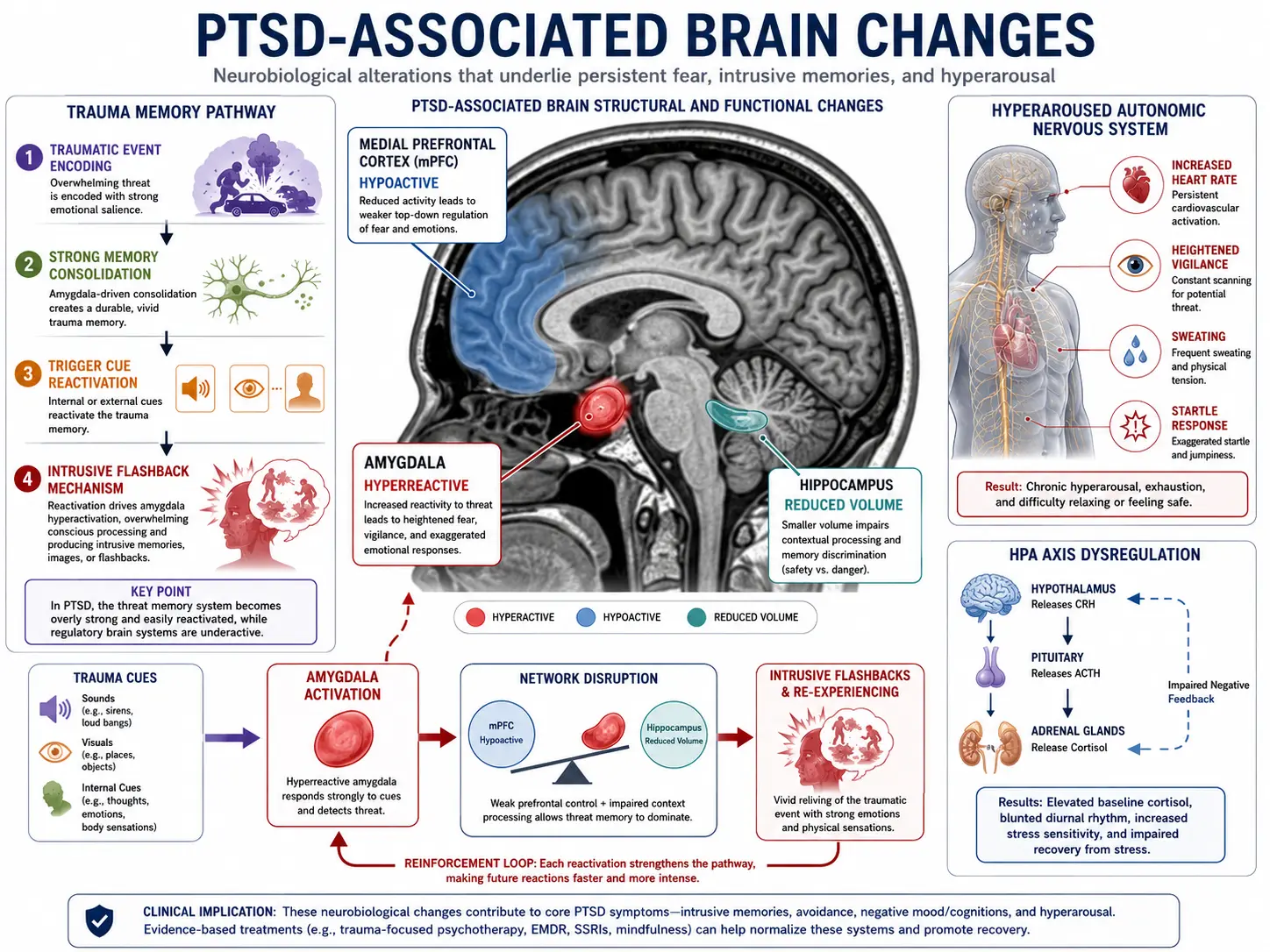
- PTSD — nightmares and hypervigilance disrupt sleep at both ends of the night.
- Chronic pain and fibromyalgia — pain lowers the arousal threshold; poor sleep then lowers the pain threshold. Each amplifies the other.
- Heart failure and COPD — breathlessness lying flat, nocturia, and the stimulant effect of inhaled beta-agonists and steroids all fragment the night.
- Acid reflux (GERD) — lying flat worsens reflux, and the resulting micro-awakenings often are not consciously remembered. People report "broken sleep for no reason."
- Thyroid disease — an overactive thyroid raises heart rate, temperature, and mental arousal: a hyperarousal amplifier. Worth a TSH test.
- Menopause — hot flushes fragment sleep most severely around the final period and can persist for years.
- Advanced kidney disease — restless legs is especially common, and uraemia is itself arousing.
- Dementia — circadian fragmentation and "sundowning" are early features.
Medications and substances that cause insomnia
This list is worth reading carefully, because the cause of a lot of stubborn insomnia is sitting in the medicine cabinet or the coffee cup.
- Caffeine — half-life 5–7 hours, meaning a 3 p.m. coffee still has roughly a quarter of its dose active at 10 p.m. A common trap: "coffee doesn't affect me, I fall asleep fine." Falling asleep is not the issue — caffeine measurably reduces deep sleep even in people who fall asleep normally. Slow metabolisers (a common CYP1A2 variant) may need to stop by midday. Do not forget tea, cola, energy drinks, dark chocolate, and some painkillers.
- Alcohol — see the section below. Briefly: it helps you fall asleep and then wrecks the second half of the night.
- Nicotine — a stimulant, and overnight withdrawal fragments sleep in regular smokers.
- Corticosteroids (prednisone) — an evening dose can cause dramatic insomnia. Moving the dose to the morning often fixes it entirely.
- Beta-blockers — suppress the body's own melatonin. The fat-soluble ones (propranolol, metoprolol) cross into the brain and are more likely to cause vivid dreams and nightmares than water-soluble ones such as atenolol.
- Decongestants (pseudoephedrine) — genuinely stimulating and very commonly overlooked.
- SSRI and SNRI antidepressants — often activating in the first week or two, and can cause vivid dreams. Usually settles.
- Bupropion — reliably activating; avoid taking it in the evening.
- Stimulants — amphetamines, methylphenidate, modafinil.
- Theophylline — blocks adenosine, exactly like caffeine.
- Thyroid hormone — particularly if the dose is too high.
6. Screen for What Mimics or Drives It
Before anyone reaches for a sleeping pill, this list needs to be worked through. A hypnotic prescribed on top of untreated sleep apnoea, untreated restless legs, or untreated depression will not fix the problem — and in the case of apnoea it can make it actively more dangerous by suppressing your drive to breathe and blunting the arousals that end each apnoea.
Obstructive sleep apnoea (OSA)
The most important thing to rule out, and the most frequently missed. Insomnia and apnoea co-occur far more often than chance — studies of the overlap (known as COMISA, co-morbid insomnia and sleep apnoea) put the shared prevalence at roughly 30–50%, which is remarkable. Many people who think they have "just insomnia" have both.
Suspect it if: loud snoring, witnessed pauses in breathing, waking with a gasp or choke, morning headaches, a dry mouth, nocturia, unrefreshing sleep despite adequate hours, or genuine daytime sleepiness (as opposed to fatigue). Risk rises with weight, age over 50, male sex, and a collar size over 17 inches (16 in women) — but thin people get it too, so a normal BMI does not rule it out. Screen with: the STOP-BANG questionnaire; a score of 3 or more warrants a sleep study. More on obstructive sleep apnoea.
Restless legs syndrome (RLS)
An irresistible urge to move the legs, with unpleasant crawling or aching sensations, worse at rest, worse in the evening, and relieved by moving. It is very treatable and very often mistaken for ordinary difficulty falling asleep.
Check: serum ferritin. RLS is strongly linked to low brain iron, and treatment guidelines suggest iron supplementation when ferritin is below about 75 ng/mL — a level most laboratories will still report as "normal," which is exactly why it gets missed. Ask for the actual number, not just "normal." More on restless legs syndrome and iron.
Depression and anxiety
Screen with the PHQ-9 and GAD-7. This is not a formality: insomnia roughly doubles the risk of going on to develop depression, and is often the first sign of it. If low mood, loss of interest, or hopelessness are present, they need treating in parallel — not after.
Chronic pain
Pain and insomnia are mutually reinforcing, and treating only one usually disappoints. Notably, CBT-I works in people with chronic pain and often improves the pain as well.
Thyroid disease
An overactive thyroid is a classic, easily-tested, easily-fixed cause of insomnia with palpitations, heat intolerance, and weight loss. Get a TSH. (An underactive thyroid can also disturb sleep, often via sleep apnoea.)
Medications and substances
Go through the list above item by item. Caffeine, alcohol, nicotine, steroids, decongestants, beta-blockers, and activating antidepressants account for a surprising share of "unexplained" insomnia — and removing the cause beats medicating around it.
Circadian rhythm disorders
If you sleep perfectly well but at the "wrong" times — cannot fall asleep until 3 a.m. but then sleep soundly until 11 a.m. — that is a body-clock timing problem, not insomnia, and the treatment is completely different (timed light and timed melatonin, not sleeping pills or sleep restriction). This distinction is routinely botched. More on circadian rhythm disorders.
7. Sleep Hygiene: Necessary but Not Sufficient
Sleep hygiene is the familiar list of sensible habits. It is worth doing. It is also — and this is the part almost nobody is told — not a treatment for chronic insomnia on its own.
The standard advice
- Keep a consistent wake time — including weekends. The single most powerful habit on this list. Your rise time is the anchor that sets the body clock; a variable one keeps the clock permanently unsettled.
- Dark, quiet, cool. Around 65–68°F (18–20°C) suits most adults. Even small light sources — a charging LED, a streetlight through thin curtains — suppress melatonin. Blackout curtains genuinely help.
- Get bright light in the morning. The most underused item here. Morning light is the strongest signal you can give your body clock, and it does more good than evening screen-avoidance does.
- Limit screens for an hour before bed — but understand why. Blue light does suppress melatonin, yet for most people the content is the bigger problem. Work email, the news, and social media are cognitively and emotionally activating. Blue-light-filtering glasses address the light and do precisely nothing about the argument you just read.
- Cut caffeine by early afternoon — 2 p.m. for most, earlier if you are a slow metaboliser.
- Do not drink alcohol to sleep. See below.
- Exercise regularly — it builds sleep pressure and, done outdoors, delivers morning light. Vigorous exercise in the 1–2 hours before bed delays sleep onset in some people, though far less than folklore suggests.
- Use the bed for sleep and sex only. Working, eating, scrolling, and watching TV in bed teach your brain that the bed is a place for being awake.
- Only get into bed when you are actually sleepy — not merely tired, and not merely because it is 10:30.
- Turn the clock around. Checking the time at 3 a.m. starts the arithmetic ("four hours left..."), and the arithmetic releases cortisol.
- If you nap, keep it under 20 minutes and before 3 p.m. — naps spend the sleep pressure you need tonight.
The reality check
Sleep hygiene alone does not fix established chronic insomnia, and the evidence on this is not ambiguous. The 2021 American Academy of Sleep Medicine guideline issues a strong recommendation against using sleep hygiene as a standalone treatment for chronic insomnia — one of the few strong negative recommendations in the whole document. A systematic review and meta-analysis of sleep hygiene education as a monotherapy found it consistently inferior to CBT-I.
This is worth stating bluntly because so many people have already been through it. If you have been told to put your phone down, cut out coffee, and buy blackout curtains — and you did all of it, diligently, and you are still lying awake — you have not failed, and you are not beyond help. You were given an incomplete treatment. Telling someone with three years of insomnia to have a warm bath is a bit like telling someone with significant hypertension to use less salt: sensible, worth doing, and nowhere near sufficient on its own.
Sleep hygiene is one component of CBT-I. It is not the active ingredient. The active ingredients are next.
8. CBT-I: The First-Line Treatment
Cognitive Behavioural Therapy for Insomnia (CBT-I) is the recommended first-line treatment for chronic insomnia — ahead of medication — by the American College of Physicians (2016), the American Academy of Sleep Medicine (2021, a strong recommendation for multicomponent CBT-I), and the European Insomnia Guideline (updated 2023). There is no serious dissent on this point.
The evidence is strong and consistent. Meta-analyses show CBT-I reliably improves how long it takes to fall asleep, how long you are awake in the night, and sleep efficiency — with roughly 70–80% of people improving meaningfully and around 40% reaching full remission. A landmark randomised trial directly comparing CBT-I with medication found that the behavioural treatment held its gains after treatment stopped, while the drug's benefits faded on discontinuation.
It is typically 4–8 sessions. It is not open-ended talking therapy — it is a structured, practical protocol with homework and a sleep diary, and it has a defined end point.
The components — what CBT-I actually consists of
1. Sleep restriction therapy — the engine
This is the most powerful component, and it is the one that sounds insane when you first hear it: to sleep more, you must first spend less time in bed.
Here is the logic. Suppose you are in bed for 9 hours but only sleeping about 5½ of them. Your sleep efficiency — sleep time divided by time in bed — is about 61%. Those 3½ hours of lying awake are doing active harm: they dilute your sleep drive across a longer window (making sleep lighter and more broken), and every one of them is a conditioning trial teaching your brain that bed means being awake.
So the sleep window is cut to match what you are actually sleeping — in this example, about 5½ hours, with a fixed rise time (say, midnight to 5:30 a.m.). This deliberately builds a sleep debt. Sleep pressure climbs, sleep consolidates, you begin falling asleep quickly and staying asleep, and efficiency rises. Once you are consistently above 85–90% efficiency, the window is widened by 15–30 minutes at a time. You gradually earn your sleep back — but now it is solid.
Be warned, because this is where most people quit: the first one to two weeks are genuinely unpleasant. You will be sleepier during the day before you are better at night. That is not the treatment failing — that is the treatment working, and it is a predictable phase. Take real care with driving and machinery during this period. Anyone doing sleep restriction properly should be told this explicitly, and it is a reason to do it with guidance rather than freelancing it. It should also be modified or avoided in people with bipolar disorder (sleep loss can trigger mania), poorly controlled epilepsy, or untreated sleep apnoea.
2. Stimulus control — retraining the bed
This directly attacks the conditioned arousal described above. The rules are short and hard to follow:
- Go to bed only when sleepy — not merely tired, and not simply because of the hour.
- If you are awake for more than about 20 minutes, get out of bed. Go to another room. Do something quiet and dull in dim light. Return only when you feel sleepy. Repeat as many times as necessary — and yes, that might be four times in one night.
- Use the bed for sleep and sex only.
- Get up at the same time every morning, regardless of how badly the night went. No sleeping in to compensate.
- Do not nap.
The "get out of bed" rule feels completely wrong. Every instinct says stay put, keep your eyes shut, and try harder. But lying in bed straining to sleep is the single behaviour most reliably keeping you awake — you cannot force sleep, and the effort of trying is itself arousing. Getting up breaks the association. Do it consistently and the bed slowly becomes a sleep cue again.
3. Cognitive restructuring — the thoughts that keep you awake
Chronic insomnia is fed by a set of beliefs that are frightening, sound plausible at 3 a.m., and are mostly false:
- "I must get eight hours or tomorrow is ruined." — Sleep need varies genuinely between people. Plenty of people function well on six and a half hours. And human performance is far more robust to a poor night than the catastrophising suggests.
- "I haven't slept properly in years." — Almost always an overgeneralisation. People with insomnia systematically underestimate how much they sleep, sometimes dramatically; sleep studies routinely record hours of sleep that the person is certain they did not get.
- "If I don't sleep tonight, something terrible will happen."
- "I have no control over this."
These beliefs generate anxiety; anxiety generates arousal; arousal prevents sleep; the bad night then "proves" the belief. Cognitive work targets that loop directly. Mindfulness- and acceptance-based approaches, which reduce the monitoring of and struggle against sleeplessness, work along the same lines and have good evidence.
There is a paradox worth naming: sleep is one of the few things that gets further away the harder you chase it. Much of CBT-I is, in effect, teaching you to stop trying so hard.
4. Relaxation training
Progressive muscle relaxation, diaphragmatic breathing, and guided imagery target the physical side of hyperarousal. Useful, and a reasonable adjunct — but on its own, not the driver of improvement.
5. Sleep hygiene education
Necessary background conditions, as covered above. One ingredient, not the recipe.
How to actually get CBT-I
Access to trained CBT-I therapists is the real bottleneck: there are far too few of them. Good alternatives exist.
- Digital CBT-I delivers the full protocol — sleep restriction, stimulus control, cognitive work — through an app or web program, and meta-analyses show it performs comparably to face-to-face therapy. A large randomised trial of Sleepio published in JAMA Psychiatry found improvements not only in sleep but in psychological wellbeing and quality of life; Somryst (which grew out of the academic SHUTi program) was authorised by the FDA in 2020 as a prescription digital therapeutic for chronic insomnia. Commercial availability of specific products does change, so check what is currently offered in your country.
- CBT-i Coach — a free app from the US Department of Veterans Affairs and Stanford. It is designed as a companion to therapy rather than a standalone course, but it is free, it is good, and it contains real CBT-I content including a sleep diary.
- Brief Behavioural Treatment for Insomnia (BBTI) — a condensed 1–4 session version built around the two heavy hitters (sleep restriction and stimulus control). Deliverable in primary care by a nurse or GP.
- Group CBT-I — as effective as individual therapy and cheaper.
- Self-help books based on the CBT-I protocol have a genuine evidence base and are a legitimate starting point if nothing else is available.
Whatever the format, keep a sleep diary. The whole method runs on it: it sets your initial sleep window, and it tells you — rather than your 4 a.m. impressions — whether things are getting better.
9. Medication: An Honest Assessment
Medication has a legitimate place. It is reasonable when insomnia is acute and severely disabling, when CBT-I is genuinely unavailable, when CBT-I has been tried and has not fully worked, or as a short bridge while behavioural treatment takes hold. It is not a moral failing to take a sleeping pill.
But you deserve a straight account of what these drugs do and do not do — and the most telling fact is this: the American Academy of Sleep Medicine's 2017 guideline on drug treatment of chronic insomnia issued only weak recommendations for every single medication it examined, on the grounds that the benefits are modest and the quality of evidence is low. That is the state of the field, from the people most sympathetic to prescribing.
The honest summary: these drugs work while you take them; none of them cure insomnia; and the effect sizes are smaller than most people imagine. Averaged across trials, the typical hypnotic gets you to sleep somewhere in the region of 10–20 minutes faster and adds a modest amount of total sleep. That is a real benefit. It is not the transformation the advertising implies.
Z-drugs — zolpidem, eszopiclone, zaleplon
Short-term use only. These act on GABA-A receptors and are the most-prescribed hypnotics in the world. The risks are real and should not be glossed over:
- Complex sleep behaviours — sleepwalking, sleep-driving, sleep-eating, with no memory of it afterwards. The FDA added a boxed warning (its most serious) for this, after cases including fatalities. Rare, but it happens at ordinary doses.
- Next-day impairment — driving performance can be measurably reduced the following morning, particularly with longer-acting and extended-release forms.
- Falls and fractures in older adults — a leading cause of death and disability in the over-65s. This is the main reason these drugs should be avoided in that group.
- Tolerance and dependence, and rebound insomnia when you stop.
- Women clear zolpidem more slowly — the FDA cut the recommended dose for women to 5 mg (vs 10 mg for men) for exactly this reason.
Zaleplon's very short half-life (about an hour) makes it the one option that can be taken during a middle-of-the-night waking, provided at least 4 hours remain before you need to be up.
Benzodiazepines — temazepam, triazolam, estazolam
Short-term use only, and increasingly a last resort. They work, but with a serious risk profile on continued use: tolerance requiring escalating doses, physical dependence and a genuinely difficult withdrawal, next-day sedation, memory impairment, and — again — falls and hip fractures.
Avoid in adults over 65 (flagged as potentially inappropriate by the American Geriatrics Society Beers Criteria, which say the same about Z-drugs); avoid in untreated sleep apnoea (they suppress breathing and blunt the arousals that terminate apnoeas); and avoid in anyone with a history of substance use disorder.
If you are already on one long-term, do not stop abruptly — benzodiazepine withdrawal can be dangerous and needs a supervised, gradual taper. It is very doable; it just needs to be done properly. Notably, CBT-I helps people come off hypnotics.
Orexin receptor antagonists — suvorexant, lemborexant, daridorexant
The genuine advance of the last decade. Rather than sedating the whole brain, these block orexin — the signal that actively holds you awake. In effect they turn down wakefulness instead of forcing unconsciousness, and the resulting sleep looks more like natural sleep. They work for both falling asleep and staying asleep, have lower dependence potential, and — unlike the older drugs — do not show the same tolerance and rebound pattern on long-term use.
They are not risk-free: next-morning drowsiness and impaired driving can occur (especially at higher doses), complex sleep behaviours have been reported, and they are contraindicated in narcolepsy. They are also expensive, with no generics — which in practice is the biggest barrier for most people. In older adults, lemborexant has been directly compared with extended-release zolpidem in a randomised trial and performed well, which matters given how poorly the older drugs suit that group.
Low-dose doxepin (3–6 mg)
An old antidepressant that, at these very low doses, acts as a clean, selective antihistamine without the anticholinergic baggage of full tricyclic doses. FDA-approved for sleep-maintenance insomnia (staying asleep, not falling asleep). No dependence. The pivotal trial was conducted in elderly subjects, which is unusual and useful — this is one of the better-supported options in older adults, where the alternatives are mostly contraindicated. Often overlooked, and cheap.
Ramelteon
A melatonin-receptor agonist. Modest effect, mainly on falling asleep. Its virtue is safety: no abuse potential, not a controlled substance, and safe in older adults — which makes it worth considering where dependence is a concern.
Melatonin — what it does and does not do
Melatonin is the most oversold sleep product in the shops, so here is the plain version.
Melatonin is a body-clock signal, not a sedative. Its real strength is shifting the timing of sleep — it is genuinely useful for jet lag, delayed sleep phase (the person who cannot fall asleep until 3 a.m.), shift work, and circadian disruption in blind people. For classic chronic insomnia — where your timing is fine and you simply cannot sleep — the effect is modest at best, and confined mainly to sleep onset, shortening the time to fall asleep by only several minutes on average. It does little for staying asleep. The AASM's 2017 guideline, having reviewed the evidence, actually recommends against melatonin as a treatment for chronic insomnia.
Two practical points if you use it anyway:
- Timing matters far more than dose. For a circadian problem, a small physiological dose (0.5–3 mg) taken several hours before your target bedtime shifts the clock earlier. Taking 10 mg as you get into bed — the most common way people use it — is close to the least effective approach.
- Supplement quality is poor. In the US, melatonin is sold as a dietary supplement and is not tightly regulated. An analysis of commercial products found actual melatonin content ranging from 83% below to 478% above the label — and some products also contained serotonin, which should not be there at all. If you buy it, buy a brand with independent third-party testing.
Trazodone — popular, but the evidence is thin
Trazodone (25–150 mg) is one of the most-prescribed sleep medications in the US — prescribed off-label, because it is not actually approved for insomnia. Its popularity is not matched by its evidence: the randomised trial data in primary insomnia is sparse and unimpressive, and the AASM 2017 guideline recommends against using trazodone for sleep-onset or sleep-maintenance insomnia. It is prescribed as much as it is because it is cheap, not controlled, and carries no dependence risk — not because it was shown to work well.
It does have legitimate uses, particularly where depression coexists. One adverse effect must be mentioned because it is a genuine emergency: priapism — a prolonged, painful erection. It is rare (on the order of 1 in 6,000 men treated), but an erection lasting more than 4 hours requires immediate emergency care to avoid permanent damage.
A trap worth knowing about: rebound insomnia
When you stop a hypnotic — especially a benzodiazepine or Z-drug — you often get a few nights that are worse than your original insomnia. This is rebound, it is a predictable pharmacological effect, and it is temporary. It feels exactly like proof that you cannot sleep without the drug, which is precisely why so many people conclude they are stuck and stay on it for years. Knowing rebound exists, expecting it, and tapering slowly with support is what gets people off. CBT-I is the most reliable way to do it.
10. Alcohol, Cannabis & Over-the-Counter Sleep Aids
Alcohol: the nightcap problem
Alcohol is by a wide margin the most common self-prescribed sleep aid, and one of the most counterproductive. Understanding why requires separating what it does to the first half of the night from what it does to the second.
The first half: alcohol is a sedative. It genuinely shortens the time it takes to fall asleep and increases deep slow-wave sleep early on. This is real, it is immediately noticeable, and it is why people believe it works. If you judge a sleep aid purely by how quickly you lose consciousness, alcohol looks excellent.
The second half: as your body metabolises the alcohol, the picture reverses completely.
- REM sleep is suppressed early in the night, then rebounds later — producing vivid, unsettling dreams and light, fragile sleep.
- The second half of the night becomes badly fragmented. Sleep gets shallow and broken, and awakenings multiply.
- The falling blood-alcohol level produces a rebound in arousal — a wired, restless wakefulness, often around 3–4 a.m., which is a genuinely miserable way to spend the small hours.
- Alcohol relaxes the upper airway muscles, making snoring and sleep apnoea measurably worse — so if you have undiagnosed apnoea, a nightcap makes it more dangerous, not just less restful.
- It is a diuretic, so you will also be getting up to use the bathroom.
- Tolerance develops quickly — the sedative effect fades within days, while the damage to the second half of the night does not. So the dose creeps up, and the sleep keeps getting worse.
Net effect: harmful. Alcohol trades a faster sleep onset for a wrecked second half of the night — and the trade gets worse over time. It is not a treatment for insomnia; used regularly for sleep, it is a reliable way to manufacture one, on top of the dependence risk. If you currently rely on it, this is not a scolding — it is the single most valuable thing you can change, and the improvement in the back half of the night is usually noticeable within a couple of weeks. You can see the fragmentation for yourself in the interactive sleep animation.
Over-the-counter antihistamines
Nearly every OTC sleep aid — "PM" formulations, night-time cold remedies, dedicated sleep tablets — is diphenhydramine or doxylamine, sedating antihistamines. The problems:
- Tolerance develops within days, so they stop working almost immediately.
- Strong anticholinergic effects — grogginess, dry mouth, constipation, urinary retention, blurred vision, confusion.
- They should be avoided in older adults (the Beers Criteria are explicit), where they raise the risk of confusion and falls; long-term anticholinergic exposure has also been linked to cognitive decline.
- The hangover effect the next morning is often worse than the insomnia was.
Occasional use for a night or two is unlikely to hurt. As a strategy for chronic insomnia, they are a poor choice.
Cannabis and CBD
Widely used for sleep, and the evidence does not yet support the enthusiasm. THC does tend to shorten sleep onset in the short term, but tolerance develops, it suppresses REM sleep, and stopping after regular use reliably produces withdrawal insomnia and vivid, disturbing dreams — which frequently drives people straight back to it. Evidence for CBD specifically in insomnia is weak. It is honest to say that the long-term picture here looks structurally similar to alcohol's: helpful tonight, unhelpful over months.
Herbal and nutritional options
Several traditional remedies have some supporting evidence, though generally modest and well short of CBT-I: valerian, chamomile, passionflower, and lemon balm. Magnesium is worth attention mainly if you are deficient — which is common — and magnesium glycinate is the better-tolerated form. None of these is a substitute for treating the disorder, and none should delay screening for apnoea, restless legs, or depression.
11. Special Situations
Older adults
Some of what gets diagnosed as insomnia after 65 is simply normal ageing of sleep and does not need treating: getting sleepy earlier and waking earlier, lighter and more fragmented sleep, less deep sleep, and a slightly shorter night. This is physiology, not disease — though it can be distressing, and reassurance is itself useful.
When genuine insomnia disorder is present, CBT-I remains first-line and works well in this age group. If medication is needed: avoid benzodiazepines and Z-drugs — the Beers Criteria flag both, and falls and hip fractures are a leading cause of death and lasting disability in older adults. Better options are low-dose doxepin (whose pivotal trial was run in elderly subjects), ramelteon, and orexin antagonists. Also avoid OTC antihistamines. And screen for sleep apnoea first — it is badly underdiagnosed in this group.
Pregnancy
Sleep is disturbed in 70–80% of pregnancies, especially the third trimester — discomfort, heartburn, fetal movement, frequent urination, leg cramps, and restless legs (which is markedly more common in pregnancy and is worth an iron check). CBT-I is first-line and is safe throughout pregnancy, which makes it an unusually clear choice here. Avoid benzodiazepines, particularly in the first trimester. Melatonin has insufficient safety data in pregnancy. Any medication should be discussed with your obstetric team.
Shift workers
Shift work sleep disorder is what happens when your job requires you to be awake when your body clock insists it is night. Standard insomnia treatment alone will not solve it — you are fighting the clock itself. What helps: timed bright light during the shift and strict light avoidance (dark glasses on the commute home); melatonin taken to target the new sleep time; a genuinely dark, quiet, cool daytime sleep space (blackout blinds, earplugs, phone off, household on board); forward-rotating shifts where there is any choice; and, where appropriate, modafinil or armodafinil, which are approved for alertness in shift work disorder.
Teenagers
The teenager who cannot fall asleep before midnight and cannot be prised out of bed at 7 a.m. is usually not lazy or defiant. Puberty produces a real, biologically driven shift to a later chronotype — melatonin release moves later. Combine that with a 7 a.m. alarm and you get chronic sleep deprivation, which looks like moodiness, poor concentration, and falling grades. The American Academy of Pediatrics recommends that middle and high schools start no earlier than 8:30 a.m. for precisely this reason.
Distinguishing genuine delayed phase from behavioural sleep restriction (phones, gaming, social media until 2 a.m.) requires a sleep diary. Morning bright light and a consistent rise time help shift the clock earlier; CBT-I adapted for adolescents works.
12. Insomnia and Mental Health
Depression: the traffic runs both ways
The old assumption was that depression causes insomnia. It is now clear the relationship is bidirectional, and the direction people find surprising is the important one: chronic insomnia roughly doubles the risk of later developing a depressive episode, and insomnia frequently arrives weeks before the mood symptoms — it is often the first sign, not a side effect.
The practical consequence: treat both, at the same time. Do not park the insomnia and hope the antidepressant sorts it out. Treating insomnia in its own right improves mood outcomes, and leaving it untreated is a well-established predictor of depressive relapse. There is a real prevention opportunity here that is routinely missed.
Anxiety
CBT-I works well for insomnia alongside anxiety, and the two treatments reinforce each other — the cognitive work overlaps substantially with standard anxiety therapy, and stimulus control and sleep restriction directly attack the anticipatory dread that drives sleep-onset insomnia. Benzodiazepines deserve extra caution here, given how easily their use becomes long-term in anxious patients.
PTSD and nightmares
In PTSD, sleep is disrupted by trauma nightmares, hypervigilance, and an exaggerated startle response. Two treatments are worth knowing about, and it is worth being accurate about the evidence for each:
- Image Rehearsal Therapy (IRT) — the best-evidenced treatment for recurrent nightmares, and endorsed by the AASM. You take a recurring nightmare, rewrite it while awake with a different, non-threatening ending, and rehearse the new version daily. It sounds too simple to work. It works: nightmare frequency and distress typically fall substantially within a handful of sessions.
- Prazosin — a blood-pressure drug that blocks adrenaline's alpha-1 receptors. The evidence is genuinely mixed, and it is often overstated. Several earlier, smaller trials — mostly in veterans — reported reduced nightmares, and it became widely used on that basis. But the largest and most rigorous trial, published in the New England Journal of Medicine in 2018, was negative: prazosin did not reduce distressing dreams or improve sleep quality compared with placebo. Guidelines have since become considerably more cautious. Prazosin may still help some individuals, and it is not unreasonable to trial it, but anyone offering it as a proven fix is ahead of the evidence. (Titrate slowly if used — it can cause dizziness and fainting from low blood pressure on standing.)
Bipolar disorder
An important safety point. In bipolar disorder, sleep loss is not only a symptom — it is a trigger for mania, and new insomnia can be the first sign of an episode building. This means sleep restriction therapy must be used with real caution, because deliberately building sleep debt can precipitate hypomania or mania. It can be done, but gradually, under mood-stabiliser cover, and in coordination with the psychiatric team. Do not undertake sleep restriction unsupervised if you have bipolar disorder.
13. Tests and Sleep Studies
The sleep diary — the one that actually matters
A two-week sleep diary is the cornerstone of both diagnosis and treatment. Each morning you record when you went to bed, roughly how long you took to fall asleep, how often and how long you woke, when you finally got up, and how you rated the night. From it comes your average total sleep time, your sleep efficiency (sleep time ÷ time in bed), and how variable your schedule is — which is what sets your CBT-I sleep window and tracks whether you are improving. It is low-tech, free, and more useful than any gadget.
Questionnaires
- Insomnia Severity Index (ISI) — 7 items, 0–28; ≥15 indicates moderate-to-severe insomnia. The best tool for tracking progress.
- Pittsburgh Sleep Quality Index (PSQI) — broader sleep-quality screen; a global score above 5 suggests poor sleep.
- Epworth Sleepiness Scale (ESS) — measures sleepiness, not fatigue. A score of 11 or more should prompt a hunt for apnoea or narcolepsy rather than a diagnosis of plain insomnia, which typically causes fatigue without pathological sleepiness.
- STOP-BANG — apnoea risk (Snoring, Tiredness, Observed apnoeas, blood Pressure, BMI, Age, Neck circumference, Gender). A score of 3 or more warrants a sleep study.
Blood tests worth having
- Ferritin — for restless legs. Ask for the number; supplementation is advised below ~75 ng/mL, which most labs still report as "normal."
- TSH — thyroid disease is a treatable cause that is easy to miss.
Polysomnography (an overnight lab sleep study)
Not routinely needed for insomnia. This surprises people, but insomnia is diagnosed from your history, and a sleep study adds nothing to a straightforward case. It is indicated when:
- Sleep apnoea is suspected — snoring, witnessed pauses, gasping, daytime sleepiness, STOP-BANG ≥3.
- Narcolepsy is suspected — sleep attacks, sleep paralysis, hallucinations at sleep onset, or cataplexy (sudden muscle weakness triggered by emotion). Followed next day by a Multiple Sleep Latency Test.
- Periodic limb movement disorder needs documenting.
- REM sleep behaviour disorder is suspected — physically acting out dreams, sometimes violently. This matters well beyond the bedroom: it is a strong early marker for Parkinson's and related conditions, and warrants neurological review.
- Insomnia has not responded to properly delivered CBT-I — to look for occult apnoea or limb movements.
Home sleep apnoea testing
Simpler, cheaper, done in your own bed, and validated for people with a high probability of straightforward obstructive sleep apnoea. Not suitable if central sleep apnoea, significant heart or lung disease, or another sleep disorder is suspected — those need a full lab study.
Actigraphy
A wrist accelerometer worn for one to two weeks. Genuinely useful for mapping circadian patterns and confirming sleep-window adherence during CBT-I. It cannot diagnose sleep apnoea.
A word about sleep trackers
Consumer wearables are reasonable at estimating when you slept and poor at staging what kind of sleep you had. More importantly, there is a well-described trap here called orthosomnia — where anxiously chasing a good sleep score makes the insomnia worse. If you find yourself waking up and immediately reaching for your sleep score to find out how you feel, the tracker has stopped helping. For people with insomnia, the usual advice is to take the tracker off. Your diary is more useful and considerably less cruel.
14. Consequences of Untreated Insomnia
Chronic insomnia is associated with a range of downstream risks. Before the list, an important caveat about how to read it — because reading a list like this at 3 a.m. is itself a known way to make insomnia worse.
These are population-level associations, not a prophecy about you, and certainly not about tonight. A bad night is not damaging you. The evidence that treating insomnia reduces these risks is strongest for depression and weaker elsewhere, and much of the association reflects long-term patterns rather than any single night. Read this as a reason to get proper treatment — not as something to lie awake worrying about, which would be precisely the wrong response and would make things worse.
- Depression — roughly a two-fold increase in risk of a future depressive episode. This is the best-established consequence and the most reversible.
- Anxiety disorders — approximately doubled risk.
- Cardiovascular disease and hypertension — insomnia, particularly when combined with objectively short sleep, is associated with a higher risk of high blood pressure and coronary disease.
- Type 2 diabetes and weight gain — sleep restriction impairs glucose tolerance and shifts appetite hormones (ghrelin up, leptin down), which reliably increases hunger.
- Inflammation and immune function — sleep disturbance is consistently linked to raised inflammatory markers.
- Concentration, memory and mood — the daytime cost most people feel most immediately.
- Accidents — drowsy driving is a real and serious hazard, and the one item on this list that can hurt you tomorrow. Do not drive when you are seriously sleep-deprived, and take particular care in the first weeks of sleep restriction therapy.
- Brain clearance and dementia risk — deep sleep drives the glymphatic system, the brain's overnight waste-clearance process, which removes proteins including amyloid-beta. Chronic disruption impairs it. This is an active and genuinely interesting research area — but it remains an association, and nobody has yet shown that treating insomnia prevents dementia. Be wary of anyone who tells you otherwise.
- Substance dependence — from using alcohol or sedatives to cope.
15. What to Expect
If it is recent
The odds are strongly in your favour, and this is worth hearing clearly. A large prospective study of good sleepers who developed acute insomnia found that about 72% recovered good sleep, and only around 6% went on to develop chronic insomnia. Most short-term insomnia resolves on its own once the stressor passes.
This deserves emphasis because the opposite message — that acute insomnia usually becomes chronic — is widely repeated and is simply not what the data show. If you are two weeks into a bad patch after a stressful event, you are far more likely to recover than not. Believing you are doomed to chronic insomnia is itself a perpetuating factor: it generates exactly the anxiety and over-compensation that convert a temporary problem into a permanent one.
The most useful thing you can do during an acute episode is avoid the compensations — do not go to bed early, do not lie in, do not nap, do not cancel your life. Keep your rise time fixed and ride it out.
If it is already chronic
Once insomnia is established, it does tend to persist without treatment. In a population-based 3-year study, roughly 46% of people with insomnia still met criteria three years later. It does not reliably burn itself out — which is the argument for treating it rather than waiting.
With treatment
- CBT-I: around 70–80% improve meaningfully and about 40% remit fully. Critically, the gains hold at 1–2 year follow-up with no ongoing treatment — you learn a skill and keep it.
- Medication: works while you take it; symptoms usually return when you stop.
- Combining them is reasonable — for instance, medication for the first few weeks while CBT-I gets going — with the plan being to taper the drug once the behavioural skills are established.
The honest summary: chronic insomnia is one of the more treatable conditions in medicine, provided you get the treatment that actually works. The main obstacle is not that insomnia is intractable — it is that most people are never offered CBT-I.
16. When to Seek Medical Care
- Sleep difficulty 3 or more nights a week for more than 3 months, with daytime consequences.
- Loud snoring, witnessed pauses in breathing, or waking with a gasp — get assessed for sleep apnoea.
- Falling asleep unintentionally — at the wheel, in meetings, mid-conversation. This is sleepiness, not insomnia, and needs urgent assessment.
- Depression, hopelessness, or any thoughts of self-harm or suicide. This warrants help now, not at the next available appointment. If you are in crisis, contact your local emergency number or a crisis line immediately.
- Acting out dreams, sleepwalking, or any night-time behaviour that could injure you or a partner.
- Evening leg discomfort relieved by movement — likely restless legs; ask for a ferritin level.
- Sudden new insomnia in an older adult — can be the first sign of depression, delirium, or a new medical problem.
- Insomnia that began with a new medication or dose change — often fixable by changing the drug or the timing.
- You want to stop a sleeping pill you have been on for a long time. Do not stop abruptly — ask for a supervised taper.
17. Recent Research and Advances
Orexin receptor antagonists are the first genuinely new mechanism in insomnia pharmacology in decades. Instead of broadly sedating the brain the way the older drugs do, they block the specific signal that keeps you awake. Long-term studies of suvorexant, lemborexant and daridorexant show sustained benefit without the tolerance and rebound that characterise the older agents, and with lower dependence potential. Cost remains the main barrier.
Digital CBT-I is the most consequential development for actual patients, because the binding constraint on CBT-I was never efficacy — it was that there are nowhere near enough trained therapists. Large randomised trials show app- and web-delivered CBT-I performing comparably to face-to-face treatment, and it is now being folded into primary care and stepped-care pathways. This is how the treatment gap actually closes.
Sleep and Alzheimer's disease. The discovery that the brain's glymphatic waste-clearance system is most active during deep sleep — clearing amyloid-beta among other proteins — has driven intense interest in whether treating sleep disorders could reduce dementia risk. Trials are underway. It is a genuinely exciting hypothesis, and it is still a hypothesis: the association is solid, the causal claim is not yet proven, and it is being over-marketed.
Insomnia subtypes and precision treatment. There is growing evidence that "insomnia" is not one condition. Work using biological and personality-based markers suggests distinct subtypes that may respond differently to CBT-I versus medication. If it holds up, this would let treatment be matched to the person rather than tried in sequence.
Wearables — and orthosomnia. Consumer sleep trackers keep improving and are increasingly used in research. But clinicians have now named the flip side: orthosomnia, insomnia driven or worsened by anxious pursuit of a good sleep score. It is a good illustration of a general truth about this condition — monitoring your sleep more closely tends to make it worse.
18. References & Research
Historical Background
Sleep medicine is a strikingly young discipline. Nathaniel Kleitman founded the first sleep laboratory at the University of Chicago in the 1920s, and in 1953 he and his student Eugene Aserinsky discovered REM sleep — before which the sleeping brain was widely assumed to be simply switched off. William Dement opened the first clinical sleep disorders centre at Stanford in 1970 and did more than anyone to establish sleep medicine as a specialty.
For most of the twentieth century insomnia was treated as a symptom of something else, and managed with barbiturates and later benzodiazepines. The turning point was behavioural. Richard Bootzin introduced stimulus control in the 1970s, and Arthur Spielman developed sleep restriction and, in 1987, published the 3P model that reframed chronic insomnia as a self-perpetuating condition rather than a symptom. Through the 1980s and 1990s Charles Morin, Jack Edinger, Colin Espie and others assembled these techniques into CBT-I and tested it in randomised trials.
The ICSD-3 (2014) formally abandoned the old "secondary insomnia" framework and recognised chronic insomnia disorder as an independent diagnosis. The 2016 American College of Physicians guideline then elevated CBT-I to first-line treatment ahead of drugs — a position reinforced by the 2021 AASM guideline and the 2023 European Insomnia Guideline. On the pharmacological side, the discovery of orexin/hypocretin in 1998 by Masashi Yanagisawa and Luis de Lecea led to suvorexant (2014), lemborexant (2019) and daridorexant (2022) — the first new mechanism in decades.
Key Research Papers
Every citation below has been individually verified against Crossref or PubMed.
- Morin CM, Benca R. Chronic insomnia. Lancet. 2012;379(9821):1129–1141.
- Qaseem A, Kansagara D, Forciea MA, Cooke M, Denberg TD. Management of chronic insomnia disorder in adults: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2016;165(2):125–133.
- Edinger JD, Arnedt JT, Bertisch SM, et al. Behavioral and psychological treatments for chronic insomnia disorder in adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2021;17(2):255–262.
- Sateia MJ, Buysse DJ, Krystal AD, Neubauer DN, Heald JL. Clinical practice guideline for the pharmacologic treatment of chronic insomnia in adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017;13(2):307–349.
- Riemann D, Espie CA, Altena E, et al. The European Insomnia Guideline: an update on the diagnosis and treatment of insomnia 2023. J Sleep Res. 2023;32(6):e14035.
- Trauer JM, Qian MY, Doyle JS, Rajaratnam SMW, Cunnington D. Cognitive behavioral therapy for chronic insomnia: a systematic review and meta-analysis. Ann Intern Med. 2015;163(3):191–204.
- van Straten A, van der Zweerde T, Kleiboer A, Cuijpers P, Morin CM, Lancee J. Cognitive and behavioral therapies in the treatment of insomnia: a meta-analysis. Sleep Med Rev. 2018;38:3–16.
- Morin CM, Vallières A, Guay B, et al. Cognitive behavioral therapy, singly and combined with medication, for persistent insomnia: a randomized controlled trial. JAMA. 2009;301(19):2005–2015.
- Maurer LF, Schneider J, Miller CB, Espie CA, Kyle SD. The clinical effects of sleep restriction therapy for insomnia: a meta-analysis of randomised controlled trials. Sleep Med Rev. 2021;58:101493.
- Spielman AJ, Saskin P, Thorpy MJ. Treatment of chronic insomnia by restriction of time in bed. Sleep. 1987;10(1):45–56.
- Spielman AJ, Caruso LS, Glovinsky PB. A behavioral perspective on insomnia treatment. Psychiatr Clin North Am. 1987;10(4):541–553.
- Chung KF, Lee CT, Yeung WF, Chan MS, Chung EW, Lin WL. Sleep hygiene education as a treatment of insomnia: a systematic review and meta-analysis. Fam Pract. 2018;35(4):365–375.
- Espie CA, Emsley R, Kyle SD, et al. Effect of digital cognitive behavioral therapy for insomnia on health, psychological well-being, and sleep-related quality of life: a randomized clinical trial. JAMA Psychiatry. 2019;76(1):21–30.
- Bonnet MH, Arand DL. Hyperarousal and insomnia: state of the science. Sleep Med Rev. 2010;14(1):9–15.
- Perlis ML, Vargas I, Ellis JG, et al. The natural history of insomnia: the incidence of acute insomnia and subsequent progression to chronic insomnia or recovery in good sleeper subjects. Sleep. 2020;43(6):zsz299.
- Morin CM, Bélanger L, LeBlanc M, et al. The natural history of insomnia: a population-based 3-year longitudinal study. Arch Intern Med. 2009;169(5):447–453.
- Morin CM, LeBlanc M, Daley M, Gregoire JP, Mérette C. Epidemiology of insomnia: prevalence, self-help treatments, consultations, and determinants of help-seeking behaviors. Sleep Med. 2006;7(2):123–130.
- Sateia MJ. International classification of sleep disorders — third edition: highlights and modifications. Chest. 2014;146(5):1387–1394.
- Baglioni C, Battagliese G, Feige B, et al. Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. J Affect Disord. 2011;135(1-3):10–19.
- Sweetman A, Lack L, Bastien C. Co-morbid insomnia and sleep apnea (COMISA): prevalence, consequences, methodological considerations, and recent randomized controlled trials. Brain Sci. 2019;9(12):371.
- Herring WJ, Connor KM, Ivgy-May N, et al. Suvorexant in patients with insomnia: results from two 3-month randomized controlled clinical trials. Biol Psychiatry. 2016;79(2):136–148.
- Rosenberg R, Murphy P, Zammit G, et al. Comparison of lemborexant with placebo and zolpidem tartrate extended release for the treatment of older adults with insomnia disorder. JAMA Netw Open. 2019;2(12):e1918254.
- Mignot E, Mayleben D, Fietze I, et al. Safety and efficacy of daridorexant in patients with insomnia disorder: results from two multicentre, randomised, double-blind, placebo-controlled, phase 3 trials. Lancet Neurol. 2022;21(2):125–139.
- Krystal AD, Durrence HH, Scharf M, et al. Efficacy and safety of doxepin 1 mg and 3 mg in a 12-week sleep laboratory and outpatient trial of elderly subjects with chronic primary insomnia. Sleep. 2010;33(11):1553–1561.
- Erland LAE, Saxena PK. Melatonin natural health products and supplements: presence of serotonin and significant variability of melatonin content. J Clin Sleep Med. 2017;13(2):275–281.
- Ebrahim IO, Shapiro CM, Williams AJ, Fenwick PB. Alcohol and sleep I: effects on normal sleep. Alcohol Clin Exp Res. 2013;37(4):539–549.
- Raskind MA, Peskind ER, Chow B, et al. Trial of prazosin for post-traumatic stress disorder in military veterans. N Engl J Med. 2018;378(6):507–517. (Note: this trial was negative — prazosin did not reduce distressing dreams or improve sleep quality versus placebo.)
- By the 2023 American Geriatrics Society Beers Criteria Update Expert Panel. American Geriatrics Society 2023 updated AGS Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2023;71(7):2052–2081.
- Vgontzas AN, Liao D, Bixler EO, Chrousos GP, Vela-Bueno A. Insomnia with objective short sleep duration is associated with a high risk for hypertension. Sleep. 2009;32(4):491–497.
- Irwin MR, Olmstead R, Carroll JE. Sleep disturbance, sleep duration, and inflammation: a systematic review and meta-analysis of cohort studies and experimental sleep deprivation. Biol Psychiatry. 2016;80(1):40–52.
- Xie L, Kang H, Xu Q, et al. Sleep drives metabolite clearance from the adult brain. Science. 2013;342(6156):373–377.
- Sakurai T. The role of orexin in motivated behaviours. Nat Rev Neurosci. 2014;15(11):719–731.
PubMed Topic Searches
- Cognitive behavioural therapy for insomnia (CBT-I)
- Sleep restriction therapy
- Stimulus control therapy
- Digital CBT-I randomised trials
- Hyperarousal in insomnia
- Chronic insomnia disorder — diagnosis
- Co-morbid insomnia and sleep apnoea (COMISA)
- Insomnia and depression — bidirectional risk
- Orexin receptor antagonists
- Z-drugs, falls and older adults
- Melatonin and circadian phase shifting
- Alcohol and sleep architecture
- Restless legs syndrome and iron
- Image rehearsal therapy for nightmares
- Orthosomnia and sleep trackers
19. Connections
- Melatonin & the Body Clock — interactive animation
- GABA: The Brain’s Brake — interactive animation
- Caffeine, Adenosine & Why Coffee Stops Working — interactive animation
- Sleep Stages & Your Body Clock — interactive animation
- History of Insomnia
- Obstructive Sleep Apnea
- Restless Legs Syndrome
- Circadian Rhythm Sleep-Wake Disorders
- Narcolepsy
- Depression
- Anxiety
- PTSD
- Bipolar Disorder
- Addiction
- Postpartum Depression
- Sleep Hygiene
- Stress Management
- Melatonin
- Chronic Pain
- Fibromyalgia
- Hyperthyroidism
- Hashimoto's Thyroiditis
- Fatigue
- Brain Fog
- Heart Palpitations
- Night Sweats
- Alzheimer's Disease
- Magnesium
- Magnesium Glycinate
- Iron
- Valerian
- Chamomile
- Passionflower
- Lemon Balm
- Hormone Panel