Iron-Deficiency Anemia: Symptoms, Causes, and Recovery
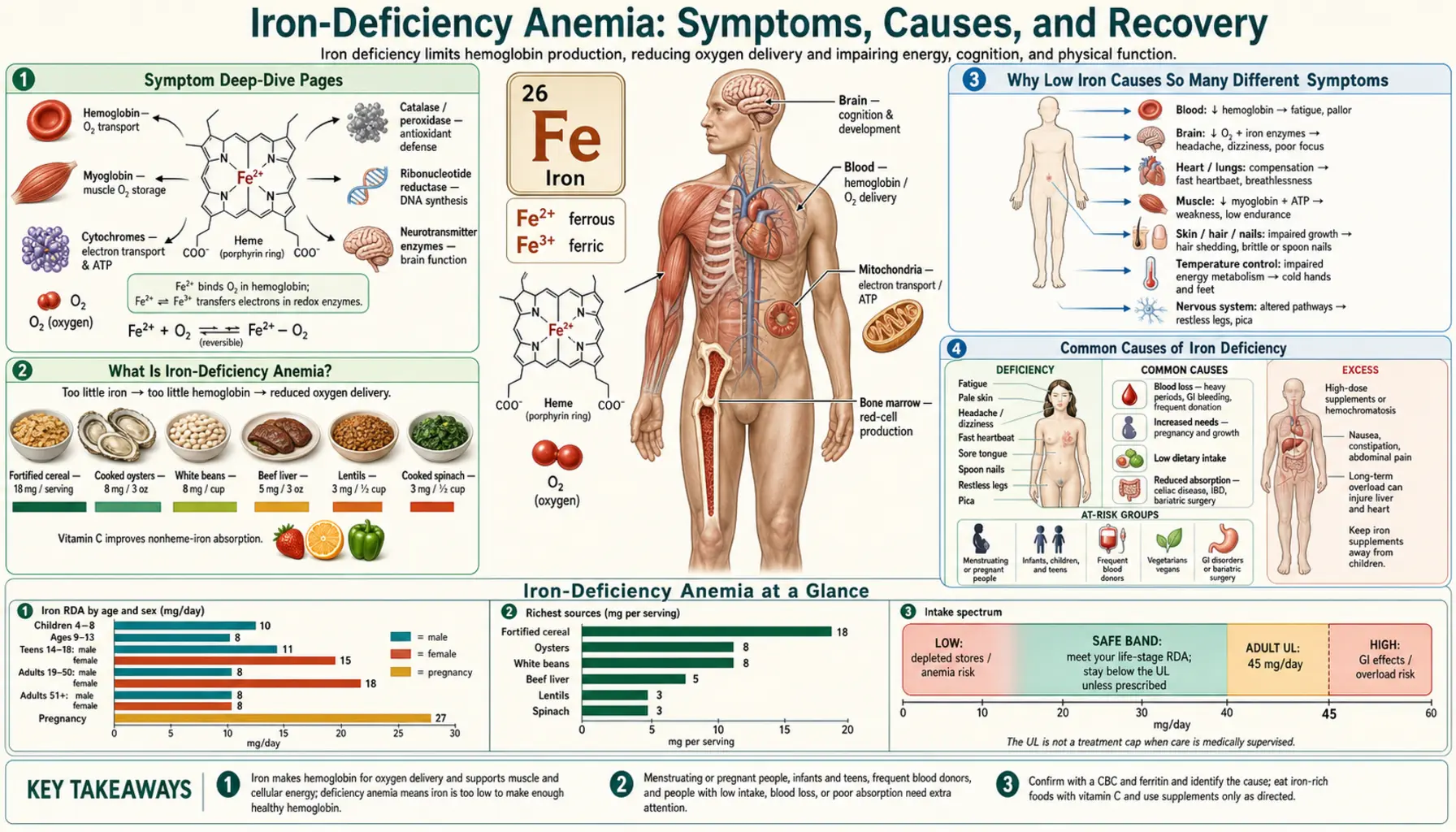
Iron-deficiency anemia means your body has run so low on iron that it can no longer build enough healthy red blood cells — and those cells are how oxygen gets delivered to every tissue you have. It is the most common nutritional deficiency in the world, affecting an estimated billion-plus people, and it produces a strikingly broad set of symptoms: bone-deep tiredness, breathlessness climbing a flight of stairs, pale skin, hair that sheds more than it should, brittle spoon-shaped nails, restless legs at night, and sometimes a strange compulsion to crunch ice. The reason one shortage causes so many different complaints is that iron sits at the center of hemoglobin, the oxygen-carrying pigment in blood; when iron falls, oxygen delivery falls, and every organ that runs on oxygen feels it. The encouraging part is that iron deficiency is usually easy to confirm with a simple blood test — especially a ferritin level, which measures your iron stores — and almost always treatable, often with food and iron tablets, occasionally with an iron infusion. But there is one rule that matters more than any other: iron deficiency is a symptom, not a diagnosis. Finding it should always prompt the question of why, because in an adult the cause is sometimes slow bleeding that needs attention. This hub explains what iron-deficiency anemia is, why it ripples into so many symptoms, what commonly causes it, and exactly how it is diagnosed and corrected — with deep-dive pages for each of the major symptoms.
Symptom Deep-Dive Pages
Fatigue & Weakness
The heavy, disproportionate tiredness and reduced exercise capacity that are usually the first and most universal signs of low iron — why oxygen-starved muscles tire so fast, and why fatigue can begin before anemia even shows up.
Breathlessness & Pallor
Why fewer red cells leave you short of breath on exertion and turn the skin, lips, and inner eyelids pale — the body's visible attempt to move enough oxygen with too little hemoglobin.
Hair Loss
The link between low ferritin and increased shedding (telogen effluvium): how iron-hungry hair follicles react to depleted stores, why hair loss can appear even without full-blown anemia, and what recovery looks like.
Restless Legs & Pica
The peculiar neurological and behavioral signs of iron deficiency — the irresistible urge to move the legs at night (restless legs syndrome), the craving to chew ice or non-food items (pica), and brittle, spoon-shaped nails.
Table of Contents
- Symptom Deep-Dive Pages
- What Is Iron-Deficiency Anemia?
- Why Low Iron Causes So Many Different Symptoms
- Common Causes of Iron Deficiency
- Related Nutrients: Vitamin C, Copper, and B12
- How Iron Deficiency Is Diagnosed
- How Iron Deficiency Is Corrected
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Is Iron-Deficiency Anemia?
To understand iron-deficiency anemia, it helps to separate two ideas that are often blurred together. Iron deficiency means your body's iron stores are low. Anemia means you do not have enough healthy red blood cells — or, more precisely, not enough hemoglobin, the iron-containing protein inside red cells that actually carries oxygen. Iron-deficiency anemia is the late stage: stores have been empty long enough that red-cell production finally falls and the hemoglobin level drops. The two do not arrive at the same moment, which is one of the most important and least appreciated facts about this condition.
Think of it as a savings account and a paycheck. Iron coming in from food is the paycheck; ferritin (stored iron) is the savings. When intake cannot keep up with losses, the body first quietly drains its savings. During this phase — called iron deficiency without anemia, or latent iron deficiency — the hemoglobin on a standard blood count can still look completely normal, yet ferritin is already low and symptoms such as fatigue, hair shedding, or restless legs may have begun. Only when the savings are truly exhausted does the paycheck-to-paycheck shortfall start to choke off red-cell production, and the hemoglobin finally falls into the anemic range. This is why a person can feel unwell, be told their "blood count is fine," and still be genuinely iron deficient — the right test simply was not ordered.
When anemia does develop, the red cells produced under iron starvation are small (the lab term is microcytic, a low MCV) and pale (hypochromic). The hemoglobin thresholds that define anemia, set by the World Health Organization, are roughly below 13 g/dL in men and below 12 g/dL in non-pregnant women (lower in pregnancy and different in young children). Severity is graded by how far hemoglobin falls:
- Iron deficiency without anemia — Low ferritin, normal hemoglobin. There may be no symptoms, or there may be early ones (tiredness, reduced stamina, hair shedding, restless legs). This is the stage where treating early is easiest and most rewarding, but also the stage most often missed.
- Mild anemia — Hemoglobin modestly below normal. Many people adapt and feel only a little more tired or breathless than usual, especially if the drop happened slowly. The body is remarkably good at compensating for a gradual decline.
- Moderate anemia — Symptoms become hard to ignore: clear fatigue, breathlessness on everyday exertion, pale skin, palpitations, lightheadedness, headaches, and trouble concentrating. This is the range where most people seek help.
- Severe anemia — Hemoglobin very low (often quoted around 7–8 g/dL or below). Now even rest may bring breathlessness and a racing heart, and the strain on the cardiovascular system becomes a genuine concern, particularly in older adults or anyone with heart disease. Severe or rapidly developing anemia can require urgent treatment, sometimes including transfusion.
Two facts are worth holding together. First, iron-deficiency anemia is extraordinarily common — it is the leading cause of anemia worldwide and the most prevalent nutritional deficiency on the planet, hitting menstruating women, pregnant women, young children, and people with gut disorders hardest. Second, and crucially, the anemia is the body's signal, not the whole story. Iron does not vanish on its own. In a child or a menstruating woman the explanation is often straightforward, but in a man or a postmenopausal woman, unexplained iron deficiency must be treated as a clue that something — frequently slow bleeding somewhere in the gut — is draining iron faster than it can be replaced. The deficiency is real and worth fixing; finding its cause can be life-saving.
Why Low Iron Causes So Many Different Symptoms
The puzzle of iron-deficiency anemia is how one missing mineral can produce complaints as different as breathlessness, hair loss, an urge to chew ice, and legs that will not settle at night. The answer is that iron is not a bit-player; it is a foundational ingredient in the single most important logistics system in the body — the delivery of oxygen — and it has a second career inside the machinery that every cell uses to make energy. Restore iron and these scattered symptoms tend to resolve together; let it run out and they appear together.
Here is the core idea in plain language. Iron is the heart of hemoglobin, the red pigment that fills your red blood cells. Each hemoglobin molecule cradles four iron atoms, and it is those iron atoms that grab oxygen in the lungs and release it in the tissues. No iron, no hemoglobin; no hemoglobin, no oxygen delivery. When iron stores run dry, the bone marrow simply cannot build enough fully-loaded red cells, so the blood's oxygen-carrying capacity drops. Every organ in the body runs on oxygen, so a shortfall in the delivery service is felt almost everywhere at once. That single mechanism explains the bulk of the symptoms:
- Muscles and whole-body energy — muscles are heavy oxygen consumers, so under-delivery makes them tire quickly and feel weak; the result is the heavy, disproportionate tiredness covered on the Fatigue & Weakness page. Iron is also a direct component of the energy-producing enzymes inside every cell's mitochondria, which is why fatigue can start even before the hemoglobin has fallen — the cellular power plants feel the shortage before the blood count does.
- Lungs and heart — the body compensates for thin, oxygen-poor blood by breathing faster and pumping harder, producing breathlessness on exertion and palpitations. The visible pallor of skin, lips, and the inner eyelids comes from the same thinned, pigment-poor blood. Both are explored on the Breathlessness & Pallor page.
- Hair, skin, and nails — fast-growing, non-essential tissues are first in line to be deprioritized when oxygen and raw materials are scarce. Hair follicles shift prematurely into the shedding phase (telogen effluvium) and nails grow brittle, ridged, and sometimes spoon-shaped (koilonychia). See the Hair Loss page.
- The brain and nervous system — iron is essential for making the brain's chemical messengers, especially dopamine. Low iron in specific brain regions is the leading explanation for restless legs syndrome and likely contributes to the brain fog and poor concentration many people report. Iron deficiency can also trigger pica — a craving to chew ice or non-food substances. These are covered on the Restless Legs & Pica page.
This is the unifying theme to carry into the symptom pages: there is nothing mysterious about iron deficiency producing a scattershot of complaints. One mineral powers both oxygen delivery and cellular energy production, so one shortage is felt in many tissues — and, helpfully, correcting it tends to lift all of them.
Common Causes of Iron Deficiency
Iron runs low for one of three broad reasons: you are losing iron through blood loss (the most important to identify in adults), you are taking in or absorbing too little, or your body's demand has outrun your supply. Because the body has no active way to excrete excess iron and conserves it tightly, a deficiency almost always points to a specific reason worth finding. Here are the causes worth knowing.
- Heavy menstrual bleeding — by far the most common cause in women who menstruate. Each period loses blood, and therefore iron; heavy or prolonged periods (menorrhagia) can drain iron faster than diet replaces it, year after year. This is so common that in a young woman with iron deficiency, the menstrual history is the first thing to review.
- Gastrointestinal blood loss — the cause that must not be missed, especially in men and postmenopausal women. Slow, often invisible bleeding from the stomach or intestines — from ulcers, long-term use of aspirin or NSAID pain relievers, polyps, inflammatory bowel disease, and importantly colorectal or stomach cancer — can deplete iron with no obvious symptom other than the anemia itself. This is precisely why unexplained iron deficiency in an adult triggers an evaluation of the gut: the deficiency can be the first and only warning sign of a serious but treatable problem.
- Pregnancy — demand soars. A growing baby, an expanding placenta, and a near-50% increase in the mother's blood volume require a large amount of extra iron, more than diet alone usually supplies. Iron deficiency is the most common nutritional problem of pregnancy, which is why iron status is checked and supplements are routinely recommended.
- Poor absorption (malabsorption) — even with adequate iron in the diet, the gut may not take it in. Celiac disease is a classic and frequently overlooked cause — sometimes iron deficiency that will not resolve is the only clue to it. Crohn's disease and other inflammatory bowel conditions, infection with Helicobacter pylori, chronic use of acid-suppressing medications (proton-pump inhibitors), and surgery that removes or bypasses part of the stomach or small intestine (such as bariatric surgery) all impair iron uptake.
- Inadequate dietary intake — less common as a sole cause in adults, because the body conserves iron well, but a real contributor when demand or losses are high. The most absorbable iron (heme iron) comes from meat, poultry, and fish; people eating little or no animal food can fall short unless they deliberately combine plant iron sources with vitamin C. Infants and toddlers fed a diet low in iron are a well-recognized at-risk group.
- Infancy, childhood, and adolescence — rapid growth raises iron needs at exactly the ages when intake is often marginal. Toddlers given large volumes of cow's milk (which is low in iron and can irritate the gut) and teenagers in a growth spurt — especially menstruating girls and athletes — are common scenarios.
- Endurance athletics and frequent blood donation — long-distance runners and other endurance athletes can lose iron through several routes (including tiny amounts of gut bleeding, foot-strike breakdown of red cells, and sweat) and have higher needs. Regular blood donors give away a meaningful amount of iron with each donation and can slip into deficiency without realizing it.
A practical note: these causes often combine. A menstruating woman who also eats little red meat and takes an NSAID for joint pain has three modest pushes in the same direction. And the single most important habit in this whole topic bears repeating: in a man or a postmenopausal woman, iron deficiency should be considered to be from gastrointestinal blood loss until proven otherwise, because the deficiency may be the body's earliest signal of something that is far easier to treat when caught early.
Related Nutrients: Vitamin C, Copper, and B12
Iron does not work alone, and understanding a few of its partner nutrients explains both why some people stay deficient despite eating iron and why iron-deficiency anemia sometimes hides inside a more complicated picture. Three relationships matter most.
Vitamin C — the absorption helper. The iron in plant foods (non-heme iron) is poorly absorbed on its own, and it is easily blocked by compounds in tea, coffee, whole grains, and legumes. Vitamin C dramatically improves the uptake of this plant iron by keeping it in the chemical form the gut absorbs best and by countering those inhibitors. In practical terms, this is why pairing iron-rich plant foods with a vitamin-C source — lentils with tomatoes and peppers, spinach with a squeeze of lemon, a glass of orange juice with a fortified cereal — meaningfully raises how much iron you actually absorb. It is one of the simplest, most evidence-based dietary tactics in this entire topic.
Copper — the quiet partner in iron transport. Copper is required to move iron around the body: copper-dependent enzymes (such as ceruloplasmin) load iron onto its transport protein so it can travel from storage and from the gut into the bloodstream. When copper is genuinely deficient — an uncommon but real situation, seen for example after bariatric surgery, with very high zinc intake from supplements or denture creams, or with certain malabsorption — iron cannot be mobilized properly, and the result can be an anemia that looks like iron deficiency but does not respond to iron. This is worth remembering when iron supplementation unexpectedly fails. (For the reverse interaction, note that high-dose zinc supplements can drive copper down.)
Vitamin B12 and folate — the other anemias, and a common disguise. Iron deficiency makes red cells small (low MCV). Deficiencies of vitamin B12 or folate do the opposite — they make red cells large (high MCV). When someone is deficient in both iron and B12 or folate at once (not unusual in malabsorption, poor diet, or after gut surgery), the two effects can cancel out, leaving a deceptively "normal" average cell size that masks two simultaneous problems. This is one reason a thoughtful work-up for anemia often checks iron studies alongside B12 and folate rather than stopping at the cell size. For more on the broader category, see the Anemia overview.
How Iron Deficiency Is Diagnosed
The reassuring part of this story is that iron deficiency is usually easy to confirm with simple, inexpensive blood tests — the difficulty is almost never in detecting it, but in remembering to order the right test and then asking why it is low. Diagnosis happens in two layers: confirming the iron deficiency, and then finding its cause.
The standard blood tests are:
- Complete blood count (CBC) — the first-line test, routine and cheap. In iron-deficiency anemia it shows a low hemoglobin together with red cells that are small (low MCV) and pale (low MCH), and often a widened range of cell sizes (high RDW). But remember the savings-account principle: the CBC can be entirely normal in early iron deficiency, before anemia has set in. A normal CBC does not rule out iron deficiency. See the Complete Blood Count page for how to read it.
- Ferritin — the single most useful test. Ferritin measures your stored iron, so it falls first, before the hemoglobin does, making it the earliest and most reliable marker of iron deficiency. A low ferritin essentially confirms the diagnosis. There is one important catch: ferritin is also an "acute-phase reactant," meaning it rises with inflammation, infection, liver disease, or chronic illness — so in those settings a normal or even high ferritin can hide a true iron deficiency. That is why doctors interpret ferritin alongside the clinical picture and the other iron studies. The full panel is detailed on the Iron Panel page.
- Serum iron, transferrin / TIBC, and transferrin saturation — together these describe iron in transit. In iron deficiency, serum iron is low, the iron-carrying capacity (TIBC/transferrin) rises as the body tries to scavenge more, and the transferrin saturation (the percentage of carrying-capacity actually filled) falls. This pattern is especially helpful for distinguishing true iron deficiency from the anemia of chronic disease, where iron is present in the body but locked away by inflammation.
Once iron deficiency is confirmed, attention turns to the more important question: why. The depth of this search depends on the person. In a menstruating woman with heavy periods, the cause may be obvious and the work-up brief. But the guidelines are clear and emphatic that in a man or a postmenopausal woman, unexplained iron deficiency warrants investigation of the gastrointestinal tract — typically endoscopy of the upper gut and a colonoscopy — to look for a bleeding source, because of the real possibility of a polyp, ulcer, or cancer. Depending on the picture, a doctor may also test for celiac disease (a blood test for tissue transglutaminase antibodies), check for H. pylori, review medications such as aspirin and NSAIDs, and in some cases test the stool for hidden blood. The point is consistent throughout the medical literature: finding the iron deficiency is the beginning of the evaluation, not the end of it.
How Iron Deficiency Is Corrected
Treatment rests on two pillars that must go together: replace the iron, and treat the underlying cause so the deficiency does not simply return. Replacing iron while ignoring a bleeding ulcer or untreated celiac disease just resets the clock. The replacement itself is usually straightforward.
- Food first — and food always. Diet alone is often too slow to correct an established anemia, but iron-rich eating supports recovery and helps prevent relapse. The most absorbable form is heme iron from animal foods — liver, red meat, poultry, and fish such as sardines. Plant (non-heme) iron — from lentils, beans, spinach and other greens, pumpkin seeds, tofu, and fortified cereals — is less efficiently absorbed but still valuable, especially when paired with a vitamin C source and kept apart from tea, coffee, and calcium-rich foods at the same meal. See Heme vs Non-Heme Iron for the practical details.
- Oral iron supplements — the usual treatment. For most people, iron tablets (commonly ferrous sulfate, ferrous gluconate, or ferrous fumarate) are the mainstay and are highly effective. Two points make them work better and feel better. First, absorption is improved by taking iron with vitamin C and on a relatively empty stomach, away from coffee, tea, dairy, and antacids. Second — and this surprised the field — recent studies suggest that taking iron every other day, in a single morning dose, can actually be absorbed as well as or better than splitting it across the day, while causing fewer side effects; this is because a large dose transiently raises hepcidin, the hormone that then blocks the next dose. The common downside of oral iron is gastrointestinal upset — nausea, constipation, dark stools, cramping — which is the main reason people stop taking it. Lowering the dose or switching to alternate-day dosing usually helps. It typically takes weeks for hemoglobin to climb and several months of continued treatment to refill the body's iron stores after the blood count has normalized; stopping too early is a frequent reason deficiency comes back.
- Intravenous (IV) iron — when tablets won't do. Modern IV iron formulations are safe and effective and are reserved for specific situations: when oral iron is not tolerated, not absorbed (for example in active inflammatory bowel disease or after certain gut surgeries), not working fast enough, or when the deficiency is severe or ongoing losses are heavy. IV iron is also commonly used in later pregnancy, chronic kidney disease, and heart failure. It refills stores quickly, often in one or a few sessions.
- Blood transfusion — for emergencies only. Transfusion is reserved for severe, symptomatic anemia or active heavy bleeding — it rapidly restores oxygen-carrying capacity but does not address the underlying iron deficiency, which still must be corrected afterward.
For most people the outlook is excellent. Once iron is replaced and the cause is addressed, energy returns, breathlessness eases, hair shedding settles over the following months, and restless legs often improve — usually within weeks to a few months. The key is to take iron long enough to refill the stores, not just to fix the blood count, and to make sure the reason for the deficiency was found and dealt with.
When to Seek Care / Red Flags
Most iron-deficiency symptoms are uncomfortable rather than dangerous, and a non-urgent appointment for a blood test is the right step for gradual tiredness, hair shedding, restless legs, or mild breathlessness — especially if you have heavy periods, are pregnant, or eat little iron-rich food. But certain features mean the situation needs prompt or emergency attention, either because the anemia is severe or because its cause may be serious. Seek urgent medical care if you have any of the following:
- Visible blood loss — black, tarry, or bloody stools; vomiting blood or material that looks like coffee grounds; or coughing up blood. These can signal significant gastrointestinal bleeding and need evaluation right away.
- Chest pain, severe breathlessness, fainting, or a racing heart — signs that anemia is straining the heart and that oxygen delivery is dangerously low, particularly in older adults or anyone with heart disease.
- Iron deficiency in a man or a postmenopausal woman — not an emergency in itself, but it should never be brushed off or simply treated with iron and forgotten. It warrants a proper evaluation of the gut to rule out a bleeding source, including cancer. Ask specifically about this if it is not offered.
- Unintended weight loss, a change in bowel habits, abdominal pain, or difficulty swallowing — alongside iron deficiency, these point toward a gastrointestinal cause that needs investigation rather than reassurance.
- Iron deficiency that does not improve with treatment — if you have taken iron correctly for a couple of months and the blood count is not responding, this needs review: the diagnosis, the dose, ongoing bleeding, poor absorption (such as undiagnosed celiac disease), or a copper or B12 problem may all be in play.
People at higher risk — pregnant women, those with heavy periods, people with inflammatory bowel disease or celiac disease, the elderly, and anyone with known heart disease — should have a lower threshold for getting their iron status checked, because the consequences of an unaddressed deficiency are greater. When in doubt, a simple ferritin and blood count settle the question. For related symptoms, see Heart Palpitations and the broader Fatigue page.
Key Research Papers
- Camaschella C (2015). Iron-Deficiency Anemia. New England Journal of Medicine;372(19):1832-1843. — DOI: 10.1056/NEJMra1401038
- Camaschella C (2019). Iron deficiency. Blood;133(1):30-39. — DOI: 10.1182/blood-2018-05-815944
- Pasricha SR, Tye-Din J, Muckenthaler MU, Swinkels DW (2021). Iron deficiency. The Lancet;397(10270):233-248. — DOI: 10.1016/S0140-6736(20)32594-0
- Camaschella C (2015). Iron deficiency: new insights into diagnosis and treatment. Hematology (American Society of Hematology Education Program);2015(1):8-13. — DOI: 10.1182/asheducation-2015.1.8
- Snook J, Bhala N, Beales ILP, Cannings D, Kightley C, et al. (2021). British Society of Gastroenterology guidelines for the management of iron deficiency anaemia in adults. Gut;70(11):2030-2051. — DOI: 10.1136/gutjnl-2021-325210
- Pavord S, Daru J, Prasannan N, Robinson S, Stanworth S, Girling J (2020). UK guidelines on the management of iron deficiency in pregnancy. British Journal of Haematology;188(6):819-830. — DOI: 10.1111/bjh.16221
- Weiss G, Goodnough LT (2005). Anemia of Chronic Disease. New England Journal of Medicine;352(10):1011-1023. — DOI: 10.1056/NEJMra041809
- Camaschella C (2020). Iron metabolism and iron disorders revisited in the hepcidin era. Haematologica;105(2):260-272. — DOI: 10.3324/haematol.2019.232124
- Trost LB, Bergfeld WF, Calogeras E. The diagnosis and treatment of iron deficiency and its potential relationship to hair loss. Journal of the American Academy of Dermatology (review). — PubMed
- Allen RP, Picchietti DL, Auerbach M, et al. Evidence-based and consensus clinical practice guidelines for the treatment of restless legs syndrome / iron. — PubMed
PubMed Topic Searches
- PubMed — Iron-deficiency anemia: diagnosis and management
- PubMed — Ferritin and iron deficiency without anemia
- PubMed — Oral iron, alternate-day dosing, and hepcidin
- PubMed — Iron deficiency and gastrointestinal blood loss
- PubMed — Intravenous iron: efficacy and safety
Connections
- Iron Deficiency: Fatigue & Weakness
- Iron Deficiency: Breathlessness & Pallor
- Iron Deficiency: Hair Loss
- Iron Deficiency: Restless Legs & Pica
- Iron-Deficiency Anemia (Hematology) — the same condition written as a blood disorder — the staged fall from depleted stores to frank anemia, the differential against other anemias, intravenous iron, complications, and prognosis.
- Iron Overview
- Iron Toxicity / Overload
- Iron Benefits Hub
- Heme vs Non-Heme Iron
- Iron Panel
- Complete Blood Count
- Comprehensive Metabolic Panel
- Anemia
- Hemochromatosis (Iron Overload)
- Celiac Disease
- Crohn's Disease
- Restless Legs Syndrome
- Hair Loss
- Fatigue
- Heart Palpitations
- Vitamin C
- Copper
- Zinc
- Beef Liver
- Beef
- Lentils
- Spinach
- Sardines
- Pumpkin Seeds