Complete Blood Count (CBC)
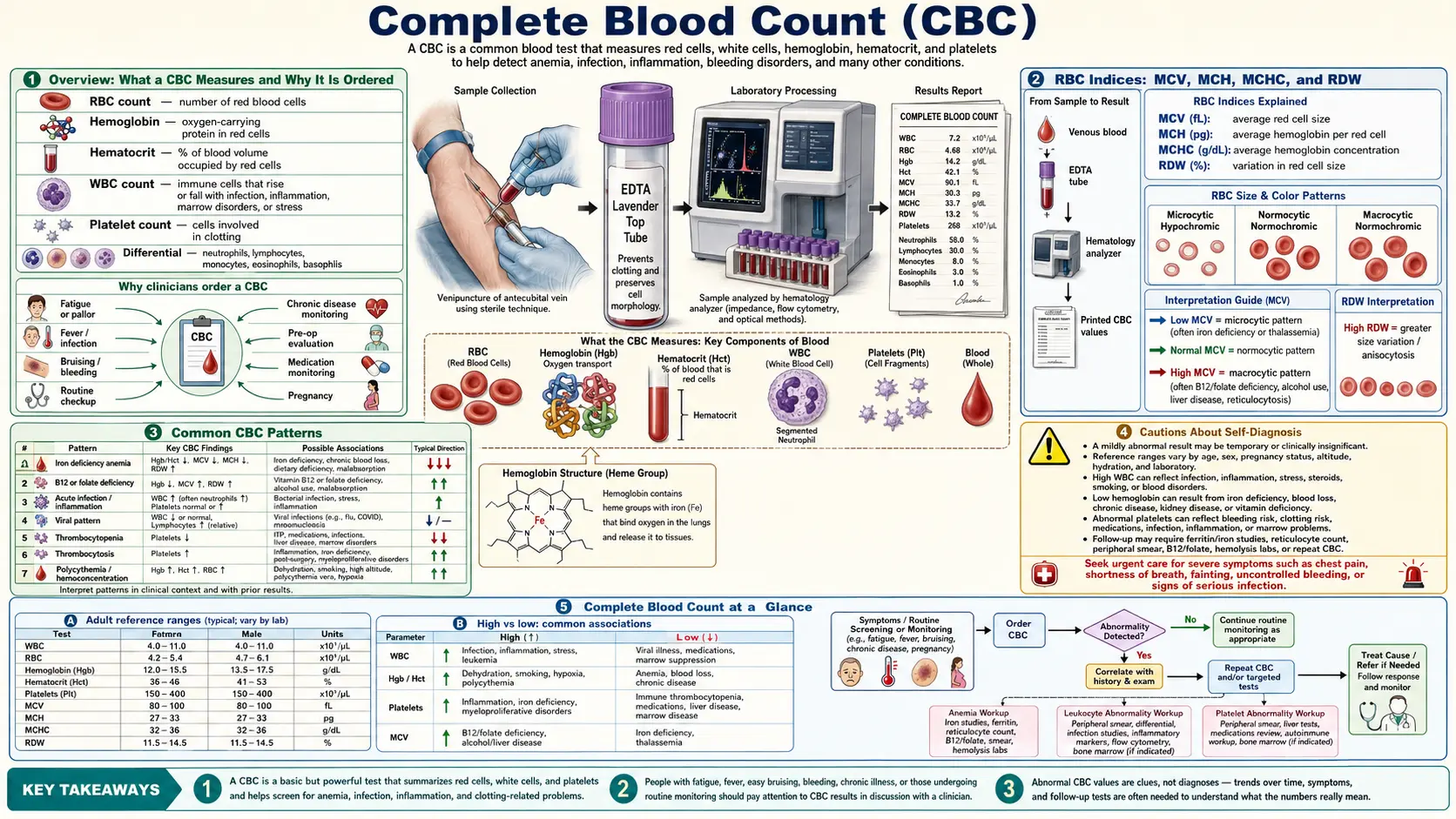


Table of Contents
- Overview: What a CBC Measures and Why It Is Ordered
- White Blood Cells (WBC) — Total Count
- WBC Differential: Neutrophils, Lymphocytes, Monocytes, Eosinophils, and Basophils
- Red Blood Cells (RBC) — Count, Hemoglobin, and Hematocrit
- RBC Indices: MCV, MCH, MCHC, and RDW
- Platelets: Count and Mean Platelet Volume (MPV)
- What High and Low Values Mean for Each Marker
- Common CBC Patterns
- Natural Strategies for Improving CBC Markers
- When to Retest
- Related Tests to Request
- Cautions About Self-Diagnosis
- Featured Videos
Overview: What a CBC Measures and Why It Is Ordered
The Complete Blood Count (CBC) is one of the most commonly ordered laboratory tests and serves as a foundational window into your overall health. It provides a comprehensive snapshot of the three major types of cells circulating in your blood: white blood cells (leukocytes), red blood cells (erythrocytes), and platelets (thrombocytes). Each of these cell populations carries critical information about immune function, oxygen-carrying capacity, and clotting ability.
From a functional medicine perspective, the CBC is far more than a simple screening tool. When interpreted through optimal (functional) reference ranges rather than just conventional laboratory ranges, it can reveal early-stage nutritional deficiencies, chronic inflammation, immune dysregulation, and metabolic imbalances long before overt disease manifests. Conventional ranges are typically derived from a population that includes many unhealthy individuals, so "normal" does not always mean "optimal."
A CBC is commonly ordered for the following reasons:
- Annual wellness exams and general health screening
- Evaluation of fatigue, weakness, or unexplained symptoms
- Monitoring of known conditions such as anemia, infection, or autoimmune disease
- Pre-surgical assessment
- Tracking the effects of medications or nutritional interventions
- Investigating unexplained bruising, bleeding, or recurrent infections
White Blood Cells (WBC) — Total Count
White blood cells are the soldiers of the immune system. The total WBC count reflects the overall level of immune activity in your body. It is one of the first markers clinicians examine when infection, inflammation, or immune compromise is suspected.
Conventional Reference Range: 4,500 - 11,000 cells per microliter (cells/mcL)
Functional (Optimal) Range: 5,000 - 8,000 cells/mcL
A total WBC count that falls within the conventional range but sits at the upper end (9,000-11,000) may indicate subclinical inflammation, chronic stress, or an immune system that is chronically activated. Conversely, a count at the lower end of conventional (4,500-5,000) may suggest immune suppression, chronic viral infection, or nutrient depletion.
From a naturopathic standpoint, the total WBC is a starting point. The true clinical value lies in examining the differential — the breakdown of the five types of white blood cells — which reveals the nature and chronicity of the immune response.
WBC Differential: Neutrophils, Lymphocytes, Monocytes, Eosinophils, and Basophils
The WBC differential breaks down the total white blood cell count into its five component types. Each cell type has a distinct role in immune defense, and shifts in their relative proportions tell a detailed story about what is happening in the body.
Neutrophils
Neutrophils are the most abundant white blood cells and serve as the first responders to bacterial infections and acute inflammation. They are short-lived cells that arrive quickly at sites of tissue damage or microbial invasion.
- Conventional Range: 40-60% (or 1,800-7,700 cells/mcL absolute)
- Functional Range: 40-60% (or 2,500-6,000 cells/mcL absolute)
Elevated neutrophils (neutrophilia) suggest acute bacterial infection, physical stress, corticosteroid use, or acute inflammation. Low neutrophils (neutropenia) may indicate viral infection, certain medications, autoimmune conditions, or bone marrow suppression.
Lymphocytes
Lymphocytes include T cells, B cells, and natural killer (NK) cells. They are the cornerstone of adaptive immunity and are involved in fighting viral infections, producing antibodies, and maintaining immune memory.
- Conventional Range: 20-40% (or 1,000-4,800 cells/mcL absolute)
- Functional Range: 25-40% (or 1,500-3,500 cells/mcL absolute)
Elevated lymphocytes (lymphocytosis) are commonly seen with viral infections, chronic infections, and certain lymphoproliferative disorders. Low lymphocytes (lymphopenia) may indicate chronic stress with elevated cortisol, HIV infection, autoimmune disease, or immune suppression from medications.
Monocytes
Monocytes are the largest of the white blood cells and serve as the cleanup crew. They migrate into tissues and differentiate into macrophages, which engulf pathogens, dead cells, and debris. They also play a role in antigen presentation to T cells.
- Conventional Range: 2-8% (or 200-950 cells/mcL absolute)
- Functional Range: 2-7% (or 200-700 cells/mcL absolute)
Elevated monocytes (monocytosis) suggest chronic inflammation, chronic infection (such as tuberculosis or endocarditis), recovery from acute infection, or autoimmune conditions. In functional medicine, persistently elevated monocytes often point to chronic, low-grade infections or unresolved tissue inflammation.
Eosinophils
Eosinophils are specialized cells involved in combating parasitic infections and modulating allergic and inflammatory responses. They release cytotoxic granules and pro-inflammatory mediators.
- Conventional Range: 1-4% (or 15-500 cells/mcL absolute)
- Functional Range: 0-3% (or 15-300 cells/mcL absolute)
Elevated eosinophils (eosinophilia) are a hallmark of allergic conditions (asthma, eczema, hay fever), parasitic infections, food sensitivities, drug reactions, and certain autoimmune conditions. From a naturopathic perspective, eosinophilia often warrants investigation into food allergies, environmental sensitivities, and intestinal parasites.
Basophils
Basophils are the rarest of the white blood cells and play a role in allergic reactions by releasing histamine and heparin. They are involved in immediate hypersensitivity responses.
- Conventional Range: 0.5-1% (or 15-100 cells/mcL absolute)
- Functional Range: 0-1% (or 15-80 cells/mcL absolute)
Elevated basophils (basophilia) may be seen with allergic reactions, hypothyroidism, chronic inflammation, myeloproliferative disorders, and certain infections. Low basophils are common and usually not clinically significant on their own.
Red Blood Cells (RBC) — Count, Hemoglobin, and Hematocrit
Red blood cells are responsible for transporting oxygen from the lungs to every tissue in the body and carrying carbon dioxide back for exhalation. The RBC section of a CBC provides critical information about your oxygen-carrying capacity and can reveal anemias, polycythemia, dehydration, and nutritional deficiencies.
RBC Count
The RBC count measures the total number of red blood cells in a given volume of blood.
- Conventional Range (Male): 4.7 - 6.1 million cells/mcL
- Conventional Range (Female): 4.2 - 5.4 million cells/mcL
- Functional Range (Male): 4.8 - 5.5 million cells/mcL
- Functional Range (Female): 4.3 - 5.0 million cells/mcL
Hemoglobin (Hgb)
Hemoglobin is the iron-containing protein within red blood cells that binds oxygen. It is the single most important marker for diagnosing anemia.
- Conventional Range (Male): 13.5 - 17.5 g/dL
- Conventional Range (Female): 12.0 - 16.0 g/dL
- Functional Range (Male): 14.0 - 16.0 g/dL
- Functional Range (Female): 13.0 - 15.0 g/dL
Low hemoglobin is the hallmark of anemia, which can result from iron deficiency, B12 or folate deficiency, chronic disease, blood loss, or bone marrow disorders. Elevated hemoglobin may indicate dehydration, polycythemia vera, chronic hypoxia (as seen in smokers or at high altitude), or excessive erythropoietin production.
Hematocrit (Hct)
Hematocrit represents the percentage of blood volume that is occupied by red blood cells. It moves in parallel with hemoglobin and RBC count.
- Conventional Range (Male): 38.3 - 48.6%
- Conventional Range (Female): 35.5 - 44.9%
- Functional Range (Male): 40 - 48%
- Functional Range (Female): 37 - 44%
Hematocrit is particularly useful for assessing hydration status. Dehydration causes hemoconcentration, which artificially raises hematocrit. Overhydration or excess fluid retention can lower it. Always interpret hematocrit in the context of hydration and the other RBC markers.
RBC Indices: MCV, MCH, MCHC, and RDW
The RBC indices provide detailed information about the size, hemoglobin content, and uniformity of red blood cells. These values are essential for classifying anemias and identifying their underlying causes.
Mean Corpuscular Volume (MCV)
MCV measures the average size of red blood cells in femtoliters (fL). It is one of the most clinically useful markers for differentiating types of anemia.
- Conventional Range: 80 - 100 fL
- Functional Range: 85 - 92 fL
Low MCV (microcytic anemia): The most common cause is iron deficiency. Other causes include thalassemia trait, chronic disease, lead poisoning, and sideroblastic anemia.
High MCV (macrocytic anemia): Often caused by vitamin B12 or folate deficiency. Other causes include hypothyroidism, liver disease, alcohol use, certain medications (methotrexate, phenytoin), and reticulocytosis.
Mean Corpuscular Hemoglobin (MCH)
MCH measures the average amount of hemoglobin per red blood cell in picograms (pg). It generally correlates with MCV.
- Conventional Range: 27 - 33 pg
- Functional Range: 28 - 32 pg
Mean Corpuscular Hemoglobin Concentration (MCHC)
MCHC measures the average concentration of hemoglobin within red blood cells. It reflects how densely packed hemoglobin is within each cell.
- Conventional Range: 32 - 36 g/dL
- Functional Range: 33 - 35 g/dL
Low MCHC (hypochromic cells) is most often seen in iron deficiency anemia. High MCHC can indicate spherocytosis or severe dehydration.
Red Cell Distribution Width (RDW)
RDW measures the variation in red blood cell size (anisocytosis). A higher RDW means greater variation in cell size, which often indicates mixed nutritional deficiencies or early-stage nutrient depletion.
- Conventional Range: 11.5 - 14.5%
- Functional Range: 11.5 - 13.0%
An elevated RDW is one of the earliest markers of iron deficiency, even before hemoglobin drops below the conventional range. In functional medicine, a rising RDW with other markers still in range is taken seriously as an early warning sign. RDW is also elevated in combined iron and B12/folate deficiency, hemolytic anemias, and after blood transfusions.
Platelets: Count and Mean Platelet Volume (MPV)
Platelets are small cell fragments produced by megakaryocytes in the bone marrow. They are essential for blood clotting and wound healing. The platelet section of the CBC provides information about both clotting ability and underlying inflammatory or marrow conditions.
Platelet Count
- Conventional Range: 150,000 - 400,000 cells/mcL
- Functional Range: 200,000 - 300,000 cells/mcL
Low platelets (thrombocytopenia) may result from autoimmune destruction (immune thrombocytopenic purpura), bone marrow suppression, viral infections, liver disease, certain medications, or nutritional deficiencies (B12, folate, iron). High platelets (thrombocytosis) can be reactive, occurring in response to infection, inflammation, iron deficiency, or surgery, or may indicate a primary myeloproliferative disorder.
Mean Platelet Volume (MPV)
- Conventional Range: 7.5 - 12.0 fL
- Functional Range: 8.0 - 10.5 fL
MPV measures the average size of platelets. Larger platelets are younger and more metabolically active. A high MPV with a low platelet count may suggest that the bone marrow is producing platelets rapidly to compensate for peripheral destruction. A low MPV with low platelets may suggest bone marrow underproduction. MPV has also been studied as an inflammatory marker, with elevated MPV being associated with cardiovascular disease risk.
What High and Low Values Mean for Each Marker
Interpreting CBC results requires looking at each marker individually and in relation to the others. Below is a summary of what elevated and depressed values may indicate for each major CBC component.
White Blood Cells
- High WBC: Bacterial infection, acute stress, corticosteroid use, leukemia, chronic inflammation, smoking, obesity
- Low WBC: Viral infection, bone marrow suppression, autoimmune conditions, severe nutritional deficiency, chemotherapy, chronic stress with cortisol dysregulation
Red Blood Cells, Hemoglobin, and Hematocrit
- High values: Dehydration, polycythemia vera, chronic hypoxia, smoking, high altitude, excessive erythropoietin
- Low values: Iron deficiency anemia, B12/folate deficiency, chronic disease anemia, blood loss, hemolysis, bone marrow failure, chronic kidney disease
MCV
- High MCV: B12 deficiency, folate deficiency, hypothyroidism, liver disease, alcohol excess, reticulocytosis
- Low MCV: Iron deficiency, thalassemia, chronic disease, lead poisoning
RDW
- High RDW: Early iron deficiency, mixed nutritional deficiency, hemolytic anemia, recent blood loss, post-transfusion
- Low RDW: Generally not clinically significant; indicates uniform cell size
Platelets
- High Platelets: Reactive thrombocytosis (infection, inflammation, iron deficiency), myeloproliferative disorders
- Low Platelets: Immune destruction, bone marrow suppression, liver disease, viral infections, drug-induced, nutritional deficiency
Common CBC Patterns
One of the most powerful aspects of the CBC is pattern recognition. Certain combinations of abnormalities point toward specific underlying conditions.
Iron Deficiency Pattern
This is the most common nutritional deficiency pattern seen on a CBC. It typically presents as:
- Low or low-normal hemoglobin and hematocrit
- Low MCV (microcytic cells)
- Low MCH and low MCHC (hypochromic cells)
- Elevated RDW (early sign, often the first marker to shift)
- Possible reactive thrombocytosis (elevated platelets)
- Low or low-normal RBC count
This pattern should be confirmed with a full iron panel including serum iron, ferritin, TIBC, and transferrin saturation. Functional ferritin targets are typically above 50 ng/mL for women and above 70 ng/mL for men, well above conventional lower limits.
B12 and Folate Deficiency Pattern
This pattern reflects impaired DNA synthesis in developing red blood cells, causing them to become abnormally large:
- Low or low-normal hemoglobin and hematocrit
- High MCV (macrocytic cells, often above 100 fL)
- High MCH
- Normal or elevated MCHC
- Elevated RDW
- Possible low WBC and low platelets in severe cases (pancytopenia)
This pattern warrants testing serum B12, methylmalonic acid (MMA), homocysteine, and serum folate. Functional B12 targets are typically above 600 pg/mL, far above the conventional lower limit of 200 pg/mL. Elevated homocysteine or MMA with a B12 in the 200-400 range is functionally deficient.
Chronic Infection Pattern
Chronic infections create a sustained, low-grade immune activation that produces characteristic CBC shifts:
- WBC that is high-normal or mildly elevated
- Elevated monocytes (suggesting chronic macrophage activation)
- Lymphocyte shifts depending on the type of infection (viral infections tend to raise lymphocytes)
- Possible mild anemia of chronic disease (low hemoglobin with normal MCV)
- Possible elevated platelets (reactive thrombocytosis)
In naturopathic practice, this pattern often leads to investigation of chronic viral reactivation (Epstein-Barr, cytomegalovirus), tick-borne infections, intestinal parasites, or dental infections.
Dehydration Pattern
Dehydration concentrates the blood, causing false elevations in several markers:
- Elevated hemoglobin and hematocrit (hemoconcentration)
- Elevated RBC count
- High-normal or elevated WBC count
- Elevated platelet count
- Normal MCV, MCH, and MCHC
This pattern is important to recognize because it can mask an underlying anemia. When a dehydrated patient is rehydrated, their hemoglobin and hematocrit may drop significantly, revealing a previously hidden deficiency. Always consider hydration status when interpreting CBC results.
Natural Strategies for Improving CBC Markers
From a naturopathic and functional medicine perspective, optimizing CBC values involves addressing root causes — primarily nutritional deficiencies, digestive function, inflammation, and lifestyle factors.
Iron-Rich Foods and Iron Absorption
For iron deficiency patterns, dietary intervention is the first line of approach:
- Heme iron sources (best absorbed): Grass-fed red meat, liver and organ meats, dark poultry meat, wild-caught fish, oysters and clams
- Non-heme iron sources: Lentils, chickpeas, dark leafy greens (spinach, kale, Swiss chard), pumpkin seeds, blackstrap molasses, quinoa
- Enhance absorption: Pair iron-rich foods with vitamin C sources (citrus, bell peppers, broccoli). Cook in cast iron cookware. Soak and sprout grains and legumes to reduce phytates.
- Reduce absorption blockers: Avoid drinking tea, coffee, or calcium-rich foods within one hour of iron-rich meals. Reduce excessive fiber supplementation around meals.
When supplementation is necessary, consider gentle forms such as iron bisglycinate, which is better tolerated and causes less gastrointestinal distress than ferrous sulfate. Lactoferrin is another option that enhances iron absorption while supporting immune function.
Vitamin B12 Strategies
B12 deficiency is extremely common, particularly in vegetarians, vegans, older adults, and those with digestive impairments:
- Food sources: Liver, clams, sardines, beef, eggs, nutritional yeast (fortified), and nori seaweed (limited bioavailability)
- Supplementation: Methylcobalamin or hydroxocobalamin are preferred over cyanocobalamin. Sublingual or liposomal forms may be better absorbed by those with digestive issues.
- Address root causes: Low stomach acid (hypochlorhydria), H. pylori infection, SIBO, celiac disease, and intrinsic factor deficiency can all impair B12 absorption. Consider digestive support with betaine HCl, digestive enzymes, or addressing gut infections.
Folate Strategies
- Food sources: Dark leafy greens, asparagus, Brussels sprouts, avocado, lentils, beets, liver
- Supplementation: Use methylfolate (5-MTHF) rather than synthetic folic acid, especially for individuals with MTHFR polymorphisms. Typical functional doses range from 400-1,000 mcg daily.
- Note: Folate and B12 work together. Supplementing folate alone can mask B12 deficiency by normalizing MCV while neurological damage from B12 deficiency continues. Always assess both nutrients together.
Vitamin C for Blood Cell Health
Vitamin C plays multiple roles in blood health:
- Enhances non-heme iron absorption by reducing ferric iron to ferrous iron
- Supports immune function and WBC activity
- Protects red blood cells from oxidative damage
- Supports collagen synthesis, which is essential for blood vessel integrity
Aim for 500-2,000 mg daily from food and supplements. Whole-food sources include citrus fruits, kiwi, strawberries, bell peppers, broccoli, and guava.
Additional Supportive Nutrients
- Copper: Essential for iron metabolism and red blood cell formation. Found in liver, oysters, dark chocolate, and mushrooms.
- Zinc: Supports immune function and WBC production. Found in oysters, pumpkin seeds, beef, and chickpeas.
- Vitamin A: Supports red blood cell production and iron mobilization from stores. Found in liver, sweet potato, carrots, and egg yolks.
- Vitamin B6: Required for hemoglobin synthesis. Found in poultry, fish, potatoes, bananas, and sunflower seeds.
When to Retest
The timing of CBC retesting depends on the clinical context and the interventions undertaken.
- After starting iron supplementation: Recheck CBC and iron panel in 8-12 weeks. Hemoglobin typically begins rising within 2-4 weeks, but full repletion of iron stores takes 3-6 months.
- After starting B12 or folate supplementation: Recheck in 8-12 weeks. MCV should begin to normalize within 4-8 weeks. Recheck B12, MMA, and homocysteine alongside the CBC.
- Monitoring chronic conditions: Every 3-6 months depending on severity and stability.
- Annual screening: For generally healthy individuals, an annual CBC is reasonable as part of a comprehensive wellness panel.
- Acute illness: Repeat as clinically indicated, potentially within days to weeks depending on the condition being monitored.
When retesting, try to keep conditions consistent: same time of day, similar hydration status, and fasting if other tests are being drawn simultaneously. This improves the comparability of results over time.
Related Tests to Request
A CBC provides a valuable overview, but it often raises questions that require additional testing to answer fully. Consider requesting these complementary tests based on CBC findings:
- Iron Panel: Serum iron, ferritin, TIBC (total iron-binding capacity), and transferrin saturation. Essential for confirming iron deficiency or iron overload.
- Vitamin B12 and Folate: Serum B12, serum folate, methylmalonic acid (MMA), and homocysteine. Critical for evaluating macrocytic anemia.
- Reticulocyte Count: Measures the production rate of new red blood cells. Helps distinguish between underproduction anemias and destruction or loss anemias.
- Comprehensive Metabolic Panel (CMP): Provides information about liver and kidney function that affects blood cell production and survival.
- C-Reactive Protein (CRP) and ESR: Markers of systemic inflammation that help contextualize WBC and platelet elevations.
- Thyroid Panel: TSH, free T3, free T4, and thyroid antibodies. Hypothyroidism can cause macrocytic anemia and other CBC abnormalities.
- Peripheral Blood Smear: A manual microscopic review of blood cells that can reveal abnormal cell shapes, inclusions, and other findings not captured by automated CBC analysis.
- Hemoglobin A1c: While primarily a diabetes marker, it also reflects red blood cell turnover. An unexpectedly low A1c with normal glucose may indicate shortened RBC lifespan.
- Copper and Zinc Levels: These minerals are involved in blood cell production and immune function and can affect CBC results when imbalanced.
Cautions About Self-Diagnosis
While understanding your CBC results is empowering and supports informed conversations with your healthcare providers, there are important cautions to keep in mind.
- Context matters: A single CBC result is a snapshot in time. Values can fluctuate with hydration, stress, time of day, recent exercise, illness, and medications. Trends over multiple tests are far more meaningful than any single result.
- Patterns over individual markers: Isolated values rarely tell the complete story. A slightly elevated WBC means something very different in the context of an acute cold than in the context of months of unexplained fatigue. Always look at the CBC as a whole and in conjunction with symptoms and other lab work.
- Serious conditions require professional evaluation: While many CBC abnormalities reflect benign, correctable causes like nutritional deficiencies, some abnormalities can indicate serious conditions including leukemia, lymphoma, myelodysplastic syndromes, aplastic anemia, and other blood disorders. Significant or persistent abnormalities always warrant thorough evaluation by a qualified healthcare provider.
- Do not self-prescribe high-dose supplements without guidance: Iron supplementation, for example, can be dangerous in individuals with hemochromatosis or iron overload. High-dose B12 can mask other conditions. Always work with a knowledgeable practitioner who can assess your full clinical picture.
- Functional ranges are guidelines, not diagnoses: Functional reference ranges are tools for identifying suboptimal patterns early. Being outside a functional range does not necessarily mean you have a disease. It means further investigation and optimization may be warranted.
- Individual variation: Some individuals have consistently low or high values for certain markers that represent their personal normal. Athletes, for example, often have lower hematocrit due to plasma volume expansion. Baseline values established during health are invaluable for comparison during illness.
The CBC is a powerful, affordable, and widely available tool for monitoring health. When interpreted through a functional medicine lens, it provides early clues that can guide preventive intervention. Partner with a qualified naturopathic doctor or functional medicine practitioner to interpret your results in the context of your complete health picture, and use the information to take proactive steps toward optimal well-being.
Research Papers and References
The following are curated PubMed literature searches covering the evidence base for complete blood count testing, interpretation, and clinical management. Each link opens a live, filtered PubMed query so the results stay current as new studies are indexed.
- Complete blood count interpretation — PubMed literature search
- Neutrophil lymphocyte ratio prognosis — PubMed literature search
- MCV macrocytosis causes — PubMed literature search
- Red cell distribution width — PubMed literature search
- Thrombocytopenia evaluation — PubMed literature search
- Eosinophilia differential — PubMed literature search
- Leukocytosis clinical — PubMed literature search
- Microcytic anemia iron deficiency — PubMed literature search
- Lymphocytosis viral infection — PubMed literature search
- Mean platelet volume cardiovascular — PubMed literature search
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — Clinical Laboratory Reference
Connections
- All Lab Tests
- Anemia
- Relationship Between Hemoglobin and Ceruloplasmin — why ceruloplasmin (the copper ferroxidase) is required to load iron into hemoglobin, and why "iron-deficiency anemia" is often functional copper deficiency.
- Iron Panel
- Vitamin B12
- Inflammatory Markers
- Iron
- Homocysteine
- Thrombocytopenia
- Polycythemia Vera
- Thalassemia
- Liver Disease
- Kidney Function
- Hemoglobin A1C
- Vitamin B12 (Vitamin)
- Vitamin C
- Hemochromatosis
- Fatigue
- Full Body MRI
- Sepsis