Iron-Deficiency Anemia: Hair Loss
If you have noticed more hair than usual circling the shower drain, collecting in your brush, or thinning across the crown and around the part, low iron is one of the most common — and most fixable — reasons to consider. Iron-deficiency hair shedding usually takes the form of telogen effluvium: a diffuse, all-over thinning rather than bald patches, often noticed two to three months after iron stores ran low. The single most useful number here is not your hemoglobin but your ferritin, the blood marker of stored iron, which can be depleted long before you are formally anemic. This page explains what iron-related shedding feels like, the “hair grows last” biology behind it, the honest fact that many other things also cause diffuse shedding, when low iron is the likely culprit, and how correcting iron brings hair back.
Interactive Visualization Hair Growth & Loss — shrink a follicle with DHT, or shed on a three-month delay Cycle a scalp of follicles through anagen, catagen and telogen, then miniaturize them with DHT year by year — or dump them all into shedding three months after a stressor. Launch →
Table of Contents
- What Iron-Related Hair Loss Feels Like
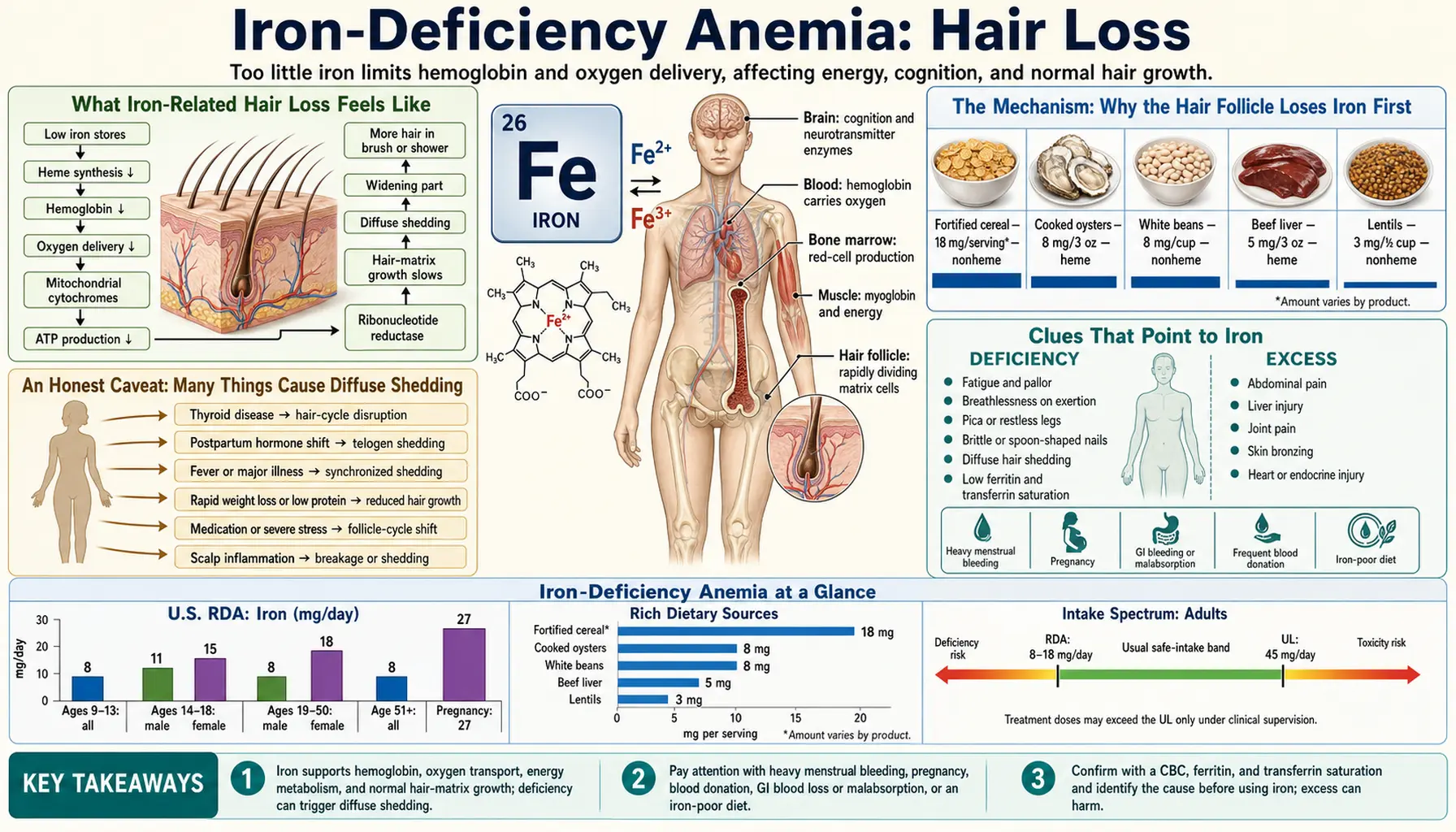
- The Mechanism: Why the Hair Follicle Loses Iron First
- An Honest Caveat: Many Things Cause Diffuse Shedding
- Clues That Point to Iron
- Why Iron Runs Low in the First Place
- Getting Tested: Ferritin Is the Key Number
- Correcting Iron — and How Long Regrowth Takes
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Iron-Related Hair Loss Feels Like
The hair loss of iron deficiency has a recognizable signature, and knowing it helps separate it from other kinds of hair loss. It is almost always diffuse — a general, even thinning across the whole scalp — rather than the distinct round patches of alopecia areata or the receding hairline of male-pattern balding. People describe it in very consistent ways:
- More shedding than usual, everywhere. It is normal to lose roughly 50–100 hairs a day. With iron-related telogen effluvium, that number climbs — sometimes to several hundred a day — and you notice it on the pillow, in the shower drain, on your clothes, and as a brush that fills up far faster than it used to.
- A thinner ponytail and a wider part. Rather than going bald in one spot, the scalp simply shows more. A common early sign is that a hair tie now wraps an extra turn, or that the part line and the crown look more “see-through” in bright light.
- Handfuls when you wash or comb. Telogen shedding is often most dramatic during washing and brushing, because those actions release hairs that had already let go at the root and were only loosely held in place.
- A delay you can almost date. Many people can trace the shedding back to a stressor two to three months earlier — heavy periods, a pregnancy, a crash diet, surgery, or a long stretch of poor eating — because the follicles were pushed into their resting phase back then and are only now letting the old hairs fall.
Two reassuring features are worth stating plainly. First, iron-related telogen effluvium is a non-scarring hair loss: the follicles are still alive and intact, just temporarily switched off, which is exactly why the hair can come back once iron is restored. Second, it usually does not produce a shiny, smooth bald scalp or visible scarring — if you see those, the cause is something else and needs a dermatologist. The shedding can be genuinely distressing, and that distress is valid; the good news threaded through this whole page is that this particular cause is one of the few that is straightforward to test for and to reverse.
The Mechanism: Why the Hair Follicle Loses Iron First
To understand iron and hair, it helps to know that each hair follicle is one of the most metabolically demanding little factories in the body. The cells at the base of an actively growing follicle (the matrix) divide faster than almost any other cells you have — they have to, in order to push out a continuously lengthening fiber of hair. Rapid cell division needs a steady supply of iron, both to make new DNA (through an iron-dependent enzyme called ribonucleotide reductase) and to keep the cell's energy factories running.
Here is the part that explains the timing. Hair grows in cycles: a long growing phase (anagen, lasting years), a brief transition, and a resting phase (telogen, lasting a few months) after which the old hair is shed and a new one begins. At any moment, roughly 85–90% of your hairs are growing and about 10–15% are resting. When the body runs short of iron, it triages: iron is rationed to the organs you cannot live without — the bone marrow making red blood cells, the heart, the brain — and non-essential tissues are pushed to the back of the line. Hair is the very definition of a tissue the body can survive without. So when iron stores fall, a wave of follicles is nudged out of their growing phase and into the resting phase early. Two to three months later, those resting hairs are released all at once, and you experience it as a sudden burst of shedding. That delayed, lagging mass shed is the textbook picture of telogen effluvium.
An analogy makes the rationing concrete. Imagine a city in a drought, with a limited water supply that must be allocated. The hospitals, the fire department, and the drinking-water taps get served first, no matter what. The decorative fountains in the park — lovely, but not life-sustaining — are the first thing the city shuts off. Your hair follicles are those fountains. When iron is scarce, the body turns them off to protect the essentials, and the “fountains” go quiet (shedding) until the reservoir — your iron stores, measured as ferritin — is refilled. Crucially, the fountain's plumbing is undamaged; restore the water and it flows again.
This rationing logic also explains why ferritin matters more than hemoglobin for hair. Hemoglobin (and a formal diagnosis of anemia) only drops once iron has been depleted for some time; ferritin — the storage form — falls first, while hemoglobin is still normal. By the time you are anemic, your hair has often been starved of iron for months. That is why a person can have “normal” blood counts and still be shedding from low iron stores, and why ferritin is the number to ask for.
An Honest Caveat: Many Things Cause Diffuse Shedding
It would be misleading to tell you that diffuse hair shedding equals low iron. It does not. Telogen effluvium — that delayed, all-over shedding — is a final common pathway that can be triggered by many stresses, and iron is only one of them. Being honest about this matters, because chasing iron alone can leave the real cause untreated. The other common drivers of diffuse shedding include:
- Thyroid disease. Both an underactive thyroid (hypothyroidism) and an overactive one can cause diffuse hair loss, and thyroid problems frequently coexist with iron deficiency — so a thyroid panel is part of any sensible work-up.
- The months after pregnancy. Postpartum telogen effluvium is extremely common — the hormonal drop after delivery sends many follicles into the resting phase at once. It often overlaps with low iron from the demands of pregnancy and any blood loss at birth.
- Crash diets and rapid weight loss. Sudden severe calorie restriction, very low protein intake, or bariatric surgery can all trigger shedding, sometimes independent of iron.
- Major physical or emotional stress. A high fever, a serious illness, surgery, or a profound life stress can each set off a telogen shed two to three months later.
- Medications. Some blood thinners, retinoids, certain antidepressants and anticonvulsants, beta-blockers, and others list hair shedding as a side effect.
- Female- and male-pattern hair loss (androgenetic alopecia). This is a different process — a gradual miniaturization of follicles, genetically driven — but it can be unmasked or worsened by a telogen shed, and the two often occur together, which is part of why the iron-and-hair research has been hard to untangle.
The scientific literature itself is genuinely mixed on iron and hair. Several studies link low ferritin to increased shedding, and a number of reviews and a meta-analysis support an association — but other well-designed studies have not found that iron status differs between women with hair loss and women without it, and there is no universal agreement on the exact ferritin level at which hair suffers. The pragmatic, evidence-based position most dermatologists take is this: iron deficiency does not cause hair loss in everyone, but in someone who is genuinely iron-deficient and shedding, correcting the iron is reasonable, low-risk, and often helps — while you also look for the other causes above. Iron is a box worth checking, not the only box.
Clues That Point to Iron
So when is low iron the likely culprit behind a diffuse shed, rather than a coincidence? A few clues raise the odds considerably, especially when several appear together:
- Other signs of iron deficiency alongside the shedding. Iron-deficiency hair loss rarely travels alone. People who are iron-depleted often also have unusual fatigue and weakness, breathlessness on exertion and pale skin, or the distinctive cluster of restless legs and odd cravings (pica) such as a powerful urge to chew ice. When hair shedding sits inside that pattern, iron jumps up the list.
- Brittle nails and spoon-shaped nails. Nails, like hair, are made by rapidly dividing cells. Iron deficiency can leave nails brittle, ridged, or — in more advanced cases — concave and spoon-shaped (koilonychia). Nail changes plus shedding is a suggestive combination.
- A heavy-periods or blood-loss history. Heavy or prolonged menstrual bleeding is the single most common reason women become iron-deficient. A woman with heavy periods who is shedding has iron deficiency as a leading explanation until proven otherwise.
- A vegetarian or vegan diet, or known poor iron intake. Plant (non-heme) iron is absorbed less efficiently than the heme iron in meat, so diets low in well-absorbed iron raise the risk.
- The shedding improves when iron is restored. This one is retrospective, but telling: if ferritin was low, iron was replenished, and the shedding settled while regrowth came in, iron was very likely contributing.
The single most decisive clue, though, is not a symptom at all — it is a blood test. A low ferritin turns suspicion into something actionable, which is why the next two sections focus on getting the right test and acting on it.
Why Iron Runs Low in the First Place
Iron-related hair loss is a downstream symptom; the real question is always why the iron is low. Pinning that down matters, because the fix depends entirely on the cause — replacing iron without addressing ongoing blood loss is like bailing a boat without patching the leak. The common causes fall into three groups:
- Blood loss (the most common cause overall). Every milliliter of blood lost carries iron out with it. In menstruating women, heavy or prolonged periods are by far the leading cause. In men and post-menopausal women, unexplained iron deficiency must prompt a look at the gastrointestinal tract for slow, often invisible bleeding — from an ulcer, inflammation, or, importantly, a colon polyp or cancer. This is why new iron deficiency in those groups is taken seriously rather than just treated with pills.
- Not enough iron coming in, or not being absorbed. Diets low in well-absorbed iron — including some vegetarian and vegan diets — can fall short over time. Pregnancy and breastfeeding dramatically increase demand. And several conditions impair absorption: celiac disease, inflammatory bowel disease, prior stomach or bowel surgery, the bacterium H. pylori, and the long-term use of acid-reducing medications (which the gut needs stomach acid to absorb non-heme iron well).
- Increased need. Beyond pregnancy, periods of rapid growth (children and teenagers) and the demands of endurance training can outpace intake — athletes, in particular, can run low through a mix of higher needs, foot-strike red-cell breakdown, and losses.
For hair specifically, the practical implication is that two people can have identical shedding for very different reasons — one a teenager with heavy periods and a low-meat diet, another a 60-year-old man with a slowly bleeding polyp. Both need iron, but the second one needs his gut investigated far more than he needs a hair-growth product.
Getting Tested: Ferritin Is the Key Number
Confirming iron as a cause of hair loss is inexpensive and decisive, but it hinges on ordering the right test. A plain complete blood count (CBC) can be completely normal in early iron deficiency, because hemoglobin is the last thing to fall. The number that matters for hair is ferritin, which reflects your stored iron and drops first. An iron panel — ferritin plus serum iron, total iron-binding capacity (TIBC), and transferrin saturation — gives the fullest picture.
Two practical points about interpreting ferritin:
- A “normal” ferritin may still be too low for hair. Many labs flag ferritin as abnormal only below about 10–15 ng/mL, but a number of dermatologists treat toward a higher target (often cited as 40–70 ng/mL) when hair loss is the concern, on the reasoning that follicles are sensitive to low stores even before frank deficiency. This target is not universally agreed upon — the evidence is genuinely mixed, as noted above — so it is a conversation to have with your clinician rather than a hard rule.
- Ferritin is also an inflammation marker. Ferritin rises with infection, inflammation, or liver inflammation, so a falsely “reassuring” normal ferritin can mask true iron deficiency when inflammation is present. That is one reason the full iron panel (with transferrin saturation) is useful, and why context matters.
Because diffuse shedding has so many causes, a sensible work-up does not stop at iron. Clinicians commonly check thyroid function (a thyroid panel), look for other nutritional gaps, and review medications, recent illnesses, pregnancy, and rapid weight changes. A blood count also screens for anemia and clues to its cause. If the scalp shows redness, scaling, or any sign of scarring rather than simple thinning, that points away from iron and toward a primary scalp or autoimmune condition — a reason to see a dermatologist.
Correcting Iron — and How Long Regrowth Takes
The encouraging reality of iron-related telogen effluvium is that the follicles are alive and the process is reversible — but it asks for patience, because hair grows slowly. Correction works on two fronts: refilling iron stores and managing expectations about timing.
- Food first, where the deficiency is mild. Well-absorbed heme iron comes from animal foods — red meat and especially organ meats, poultry, and fish. Plant (non-heme) sources include lentils and beans, spinach and other dark leafy greens, tofu, and fortified grains. Pairing plant iron with vitamin C (citrus, peppers, tomatoes — see Vitamin C) markedly improves absorption, while tea, coffee, and calcium taken at the same meal reduce it. The iron-rich foods list goes into detail.
- Oral iron supplements are the mainstay when diet alone cannot rebuild stores. They are effective but can cause constipation, dark stools, and stomach upset; taking them on alternate days, or every day at a lower dose, is increasingly favored because it can improve absorption and is gentler on the gut. Replenishing stores enough to help hair typically takes several months, not weeks. Iron supplements should be kept away from children — iron overdose is a serious poisoning in young kids — and not started long-term without testing, since the body has no good way to excrete excess iron.
- Intravenous (IV) iron or further work-up is used when oral iron is not tolerated, not absorbed, or not keeping up with ongoing loss, or when the deficiency is severe. Treating the underlying cause — managing heavy periods, treating celiac disease, finding a source of gut bleeding — is what makes the fix last.
What to expect with the hair, honestly: shedding from telogen effluvium often continues for a little while even after iron is being replaced, because the hairs that were already committed to the resting phase still have to fall. Regrowth then comes in gradually — you may first notice a fringe of short new hairs along the hairline and part. Because scalp hair grows only about a centimeter a month, it commonly takes three to six months after iron stores normalize to see meaningful thickening, and longer to fully recover length. That slow timeline is normal and is not a sign of failure.
A word on the supplements often marketed for hair: biotin is heavily promoted, but true biotin deficiency is rare, and there is little evidence that biotin helps hair in people who are not deficient — meanwhile high-dose biotin can interfere with several lab tests (including thyroid and cardiac tests). Zinc can be relevant when it is genuinely low, but supplementing minerals you are not short of is not harmless. The most reliable move is to correct a documented deficiency — iron when iron is low — rather than to layer on unproven products.
When to Seek Care / Red Flags
Most iron-related shedding is corrected calmly with testing, diet, and a clinician's guidance. But certain features mean you should be evaluated promptly rather than self-treating:
- Sudden, severe, or rapidly worsening shedding, or hair loss in distinct patches, a receding line, or with a smooth, shiny, or scarred scalp — these suggest a cause other than simple iron-related telogen effluvium and need a dermatologist.
- Iron deficiency in a man or a post-menopausal woman. Outside of menstruation, unexplained iron deficiency must be investigated for a source of bleeding — including the gastrointestinal tract — rather than just treated with pills.
- Heavy or prolonged menstrual bleeding driving the iron loss — worth addressing in its own right, both for your iron and your quality of life.
- Symptoms of significant anemia — marked fatigue and weakness, breathlessness, a racing heart, or pallor, dizziness, or chest pain — which need timely assessment.
- Scalp redness, scaling, pain, or itching with the hair loss, which points toward a scalp or autoimmune condition.
- No regrowth after several months of corrected, normalized iron stores — a sign to revisit the diagnosis, because another cause (thyroid, pattern hair loss, a medication) may be at work.
Hair loss can carry a real emotional weight, and seeking help is reasonable even when nothing on this list applies. The reassuring bottom line: when low iron is the cause, it is testable and treatable, and the follicles are waiting to grow again.
Key Research Papers
- Camaschella C (2015). Iron-Deficiency Anemia. New England Journal of Medicine;372(19):1832-1843. — DOI: 10.1056/NEJMra1401038
- Trost LB, Bergfeld WF, Calogeras E (2006). The diagnosis and treatment of iron deficiency and its potential relationship to hair loss. Journal of the American Academy of Dermatology;54(5):824-844. — DOI: 10.1016/j.jaad.2005.11.1104
- St. Pierre SA, Vercellotti GM, Donovan JC, Hordinsky MK (2010). Iron deficiency and diffuse nonscarring scalp alopecia in women: more pieces to the puzzle. Journal of the American Academy of Dermatology;63(6):1070-1076. — DOI: 10.1016/j.jaad.2009.05.054
- Olsen EA, Reed KB, Cacchio PB, Caudill L (2010). Iron deficiency in female pattern hair loss, chronic telogen effluvium, and control groups. Journal of the American Academy of Dermatology;63(6):991-999. — DOI: 10.1016/j.jaad.2009.12.006
- Kantor J, Kessler LJ, Brooks DG, Cotsarelis G (2003). Decreased serum ferritin is associated with alopecia in women. Journal of Investigative Dermatology;121(5):985-988. — DOI: 10.1046/j.1523-1747.2003.12540.x
- Gowda D, Premalatha V, Imtiyaz DB (2021). Iron Deficiency and Nonscarring Alopecia in Women: Systematic Review and Meta-Analysis. Skin Appendage Disorders;8(2):83-92. — DOI: 10.1159/000519952
- Rushton DH (2002). Nutritional factors and hair loss. Clinical and Experimental Dermatology;27(5):396-404. — DOI: 10.1046/j.1365-2230.2002.01076.x
- Malkud S (2002). Telogen effluvium: a review. Clinical and Experimental Dermatology;27(5):389-395. — DOI: 10.1046/j.1365-2230.2002.01080.x
- Harrison S, Bergfeld W (2009). Diffuse hair loss: its triggers and management. Cleveland Clinic Journal of Medicine;76(6):361-367. — DOI: 10.3949/ccjm.76a.08080
- Kil MS, Kim CW, Kim SS (2013). Analysis of serum zinc and copper concentrations in hair loss. Annals of Dermatology;25(4):405-409. — DOI: 10.5021/ad.2013.25.4.405
- Patel DP, Swink SM, Castelo-Soccio L (2017). A review of the use of biotin for hair loss. Skin Appendage Disorders;3(3):166-169. — DOI: 10.1159/000462981
PubMed Topic Searches
- PubMed — Iron deficiency, hair loss, and telogen effluvium
- PubMed — Serum ferritin and alopecia in women
- PubMed — Telogen effluvium causes and management
- PubMed — Ferritin threshold and hair-loss treatment
- PubMed — Nutritional deficiency and diffuse alopecia
Connections
- Hair Growth, Thinning & Why Hair Falls Out — interactive animation
- Iron-Deficiency Symptom Hub
- Iron Deficiency and Fatigue & Weakness
- Iron Deficiency: Breathlessness & Pallor
- Iron Deficiency: Restless Legs & Pica
- Iron Overview
- Iron Deficiency Anemia
- Iron-Rich Foods
- Heme vs. Non-Heme Iron
- Iron Panel (Ferritin)
- Complete Blood Count
- Vitamin C (Iron Absorption)
- Zinc
- Hypothyroidism
- Celiac Disease
- Beef
- Spinach
- Hair Loss — the general symptom page covering the full differential, including the non-iron causes of diffuse shedding.