Iron Panel
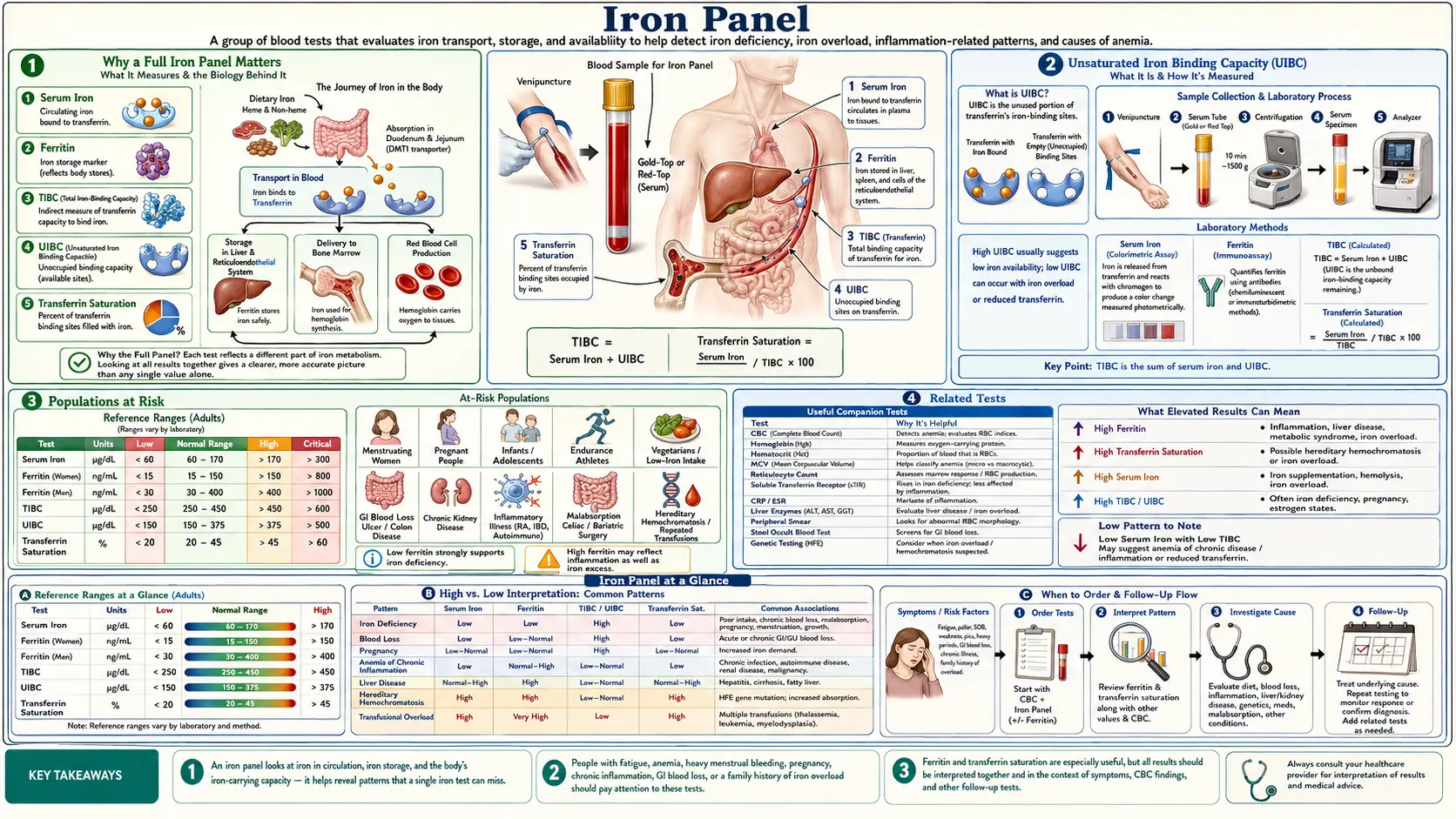
Table of Contents
- Why a Full Iron Panel Matters
- Serum Iron
- Ferritin: Iron Storage Protein
- Total Iron Binding Capacity (TIBC)
- Transferrin Saturation Percentage
- Unsaturated Iron Binding Capacity (UIBC)
- Common Iron Panel Patterns
- Symptoms of Iron Deficiency
- Symptoms of Iron Overload
- Populations at Risk
- Iron Absorption Factors
- Natural Strategies for Improving Iron Status
- Iron Supplementation Guidelines
- When to Retest
- Related Tests
- Featured Videos
Why a Full Iron Panel Matters
Iron is one of the most critical minerals in human physiology, serving as the central atom in hemoglobin for oxygen transport, playing essential roles in mitochondrial energy production, and supporting thyroid hormone synthesis, neurotransmitter metabolism, and immune function. Despite its importance, iron status is frequently assessed with only a single marker, most often ferritin alone, which can be profoundly misleading.
A comprehensive iron panel includes serum iron, ferritin, TIBC (total iron binding capacity), transferrin saturation percentage, and UIBC (unsaturated iron binding capacity). Evaluating all of these markers together provides a three-dimensional picture of iron metabolism: how much iron is circulating right now, how much is stored, how much capacity the body has to carry more, and whether iron is being appropriately mobilized from storage into active use.
Relying on ferritin alone is especially problematic because ferritin is an acute phase reactant, meaning it rises during infection, inflammation, liver disease, and metabolic stress regardless of actual iron stores. A patient with chronic inflammation may show a normal or even elevated ferritin while being functionally iron deficient at the tissue level. Conversely, early iron overload can be missed if only ferritin is checked without transferrin saturation. The full panel catches what individual markers miss.
Serum Iron
Serum iron measures the amount of iron currently circulating in the bloodstream, bound to the transport protein transferrin. This marker reflects iron that is in transit between sites of absorption (the small intestine), storage (the liver, spleen, and bone marrow), and utilization (the bone marrow for red blood cell production, muscles, and other tissues).
The conventional reference range for serum iron is typically 60 to 170 mcg/dL for men and 50 to 170 mcg/dL for women. From a functional medicine perspective, optimal serum iron generally falls in the range of 85 to 130 mcg/dL.
One of the most important characteristics of serum iron is its significant daily fluctuation. Serum iron levels can vary by as much as 30 to 50 percent within a single day. Levels tend to be highest in the morning and lowest in the late afternoon and evening. They are also influenced by recent meals, particularly iron-rich meals consumed within the previous 12 to 24 hours. For this reason, serum iron should always be drawn fasting and in the morning for the most consistent results, and it should never be interpreted in isolation.
A low serum iron may indicate iron deficiency, but it can also be seen in acute or chronic inflammation, infection, or chronic disease states where the body deliberately sequesters iron away from the bloodstream as a defense mechanism against pathogens. An elevated serum iron may suggest iron overload, hemochromatosis, hemolytic anemia, or excessive supplementation.
Ferritin: Iron Storage Protein
Ferritin is the primary iron storage protein in the body. Each ferritin molecule can store up to 4,500 atoms of iron in a safe, non-toxic form. Ferritin is found primarily in the liver, spleen, bone marrow, and skeletal muscle, and a small amount circulates in the bloodstream. Serum ferritin levels generally correlate with total body iron stores, making it a valuable screening marker when interpreted correctly.
Conventional laboratory reference ranges for ferritin are extremely broad, typically listed as 12 to 150 ng/mL for women and 12 to 300 ng/mL for men. These ranges are designed to capture roughly 95 percent of the tested population, not to define optimal health. From a functional and integrative medicine perspective, the optimal ferritin range is considerably narrower:
- Women (premenopausal): 50 to 100 ng/mL optimal; below 30 ng/mL is associated with hair loss, fatigue, and restless legs even without frank anemia
- Women (postmenopausal): 50 to 120 ng/mL optimal
- Men: 50 to 150 ng/mL optimal
- Below 20 ng/mL: Virtually diagnostic of iron deficiency regardless of other markers
- Above 200 ng/mL (women) or 300 ng/mL (men): Warrants investigation for iron overload or inflammatory causes
The critical caveat with ferritin is that it behaves as an acute phase reactant. Ferritin levels rise in response to inflammation, infection, liver damage, autoimmune conditions, obesity, metabolic syndrome, and even intense physical exercise. This means a patient with significant systemic inflammation may have a ferritin of 80 ng/mL that appears normal but actually masks underlying iron deficiency. In such cases, transferrin saturation becomes especially important because it is not an acute phase reactant and more accurately reflects functional iron availability.
When ferritin is elevated, it is essential to consider whether the elevation reflects true iron overload or is an inflammatory artifact. Checking CRP (C-reactive protein) alongside the iron panel helps distinguish these two scenarios. If CRP is elevated, the ferritin value must be interpreted with great caution.
Total Iron Binding Capacity (TIBC)
TIBC measures the maximum amount of iron that can be bound by proteins in the blood, primarily transferrin. Transferrin is the main transport protein that carries iron through the bloodstream from sites of absorption and storage to sites of utilization. TIBC is essentially an indirect measurement of transferrin levels.
The conventional reference range for TIBC is typically 250 to 400 mcg/dL. Functional optimal ranges are generally considered to be 275 to 375 mcg/dL.
TIBC has an inverse relationship with iron stores. When the body is iron deficient, the liver produces more transferrin in an attempt to capture and transport whatever iron is available, causing TIBC to rise. Conversely, when iron stores are adequate or excessive, transferrin production decreases, and TIBC falls.
- Elevated TIBC: Suggests iron deficiency, as the body is making more transferrin to scavenge available iron. Also elevated in pregnancy and with oral contraceptive use.
- Low TIBC: Suggests iron overload, chronic inflammation, chronic disease, liver disease, malnutrition, or nephrotic syndrome. In inflammation, the body downregulates transferrin production as part of the innate immune response to restrict iron availability to pathogens.
Because TIBC reflects transferrin production, it provides valuable information about the body's perception of its iron status and its attempt to regulate iron transport accordingly.
Transferrin Saturation Percentage
Transferrin saturation is calculated by dividing serum iron by TIBC and multiplying by 100. It represents the percentage of transferrin molecules that are currently carrying iron. Of all the individual markers on an iron panel, transferrin saturation is often considered the single most clinically useful marker for assessing functional iron status.
The conventional reference range is 20 to 50 percent. Functional optimal ranges are typically 25 to 35 percent for women and 30 to 40 percent for men.
- Below 20 percent: Strongly suggestive of iron deficiency, even if ferritin appears normal. Tissues are not receiving adequate iron delivery.
- Below 16 percent: Iron-deficient erythropoiesis is likely occurring, meaning the bone marrow does not have enough iron to produce red blood cells efficiently.
- Above 45 percent: Raises concern for iron overload. In the context of hereditary hemochromatosis screening, a transferrin saturation above 45 percent is the most sensitive early marker.
- Above 60 percent: Strongly suggestive of hemochromatosis or significant iron overload, warranting further genetic testing and evaluation.
Transferrin saturation is particularly valuable because it is not significantly affected by inflammation in the way that ferritin is. When inflammation is present, transferrin saturation helps reveal whether the body actually has enough iron available for metabolic needs, regardless of what ferritin shows. This makes it indispensable in patients with chronic inflammatory conditions, autoimmune diseases, obesity, or chronic infections.
Unsaturated Iron Binding Capacity (UIBC)
UIBC measures the reserve capacity of transferrin that is not currently occupied by iron. It represents the portion of total iron binding capacity that remains available to bind additional iron. UIBC is calculated as TIBC minus serum iron, or it may be measured directly by some laboratories.
The conventional reference range for UIBC is typically 110 to 370 mcg/dL.
- Elevated UIBC: Indicates that a large proportion of transferrin is unoccupied and hungry for iron. This pattern is characteristic of iron deficiency, where the body has produced abundant transferrin but does not have enough iron to fill it.
- Low UIBC: Indicates that most transferrin is already saturated with iron. This is seen in iron overload conditions, hemochromatosis, or excessive iron supplementation. It may also be seen in chronic inflammation and liver disease.
While UIBC is sometimes considered redundant because it can be derived from TIBC and serum iron, including it on the panel provides a useful cross-check and makes it easier to spot laboratory errors or inconsistencies in the data.
Common Iron Panel Patterns
Interpreting an iron panel requires pattern recognition. The following are the three most commonly encountered clinical patterns, each with distinct marker profiles:
Iron Deficiency Anemia
- Serum iron: Low
- Ferritin: Low (typically below 20 ng/mL)
- TIBC: High (the body is making more transferrin to capture scarce iron)
- Transferrin saturation: Low (below 20 percent)
- UIBC: High
This is the classic depletion pattern. Iron stores are exhausted, and the body is actively trying to compensate by increasing its iron-carrying capacity. If the CBC shows a low hemoglobin with microcytic (small) and hypochromic (pale) red blood cells, iron deficiency anemia is confirmed.
Anemia of Chronic Disease / Inflammation
- Serum iron: Low
- Ferritin: Normal to High (elevated as an acute phase reactant, not reflecting true stores)
- TIBC: Low to Normal (the body deliberately downregulates transferrin)
- Transferrin saturation: Low to Normal
- UIBC: Variable
This pattern is driven by the inflammatory cytokine hepcidin, which the liver produces in response to inflammation. Hepcidin blocks iron absorption from the gut and traps iron inside storage cells, effectively sequestering iron away from the bloodstream. This is an evolutionary defense mechanism designed to starve invading bacteria of iron. However, in chronic inflammatory conditions, this mechanism becomes counterproductive and leads to functional iron deficiency even though total body iron stores may be adequate. The key distinguishing feature from true iron deficiency is the normal or elevated ferritin combined with low TIBC.
Hemochromatosis / Iron Overload
- Serum iron: High
- Ferritin: High (often above 300 ng/mL, and in advanced cases above 1,000 ng/mL)
- TIBC: Low to Normal
- Transferrin saturation: High (above 45 percent, often above 60 percent)
- UIBC: Low
Iron overload can be hereditary (hemochromatosis, most commonly the HFE gene C282Y mutation) or acquired through repeated blood transfusions, chronic liver disease, or excessive supplementation. Excess iron is highly toxic because it generates free radicals through the Fenton reaction, causing oxidative damage to the liver, heart, pancreas, joints, and endocrine glands. Early detection through transferrin saturation screening is critical because organ damage from iron overload is preventable with timely treatment through therapeutic phlebotomy.
Symptoms of Iron Deficiency
Iron deficiency is the most common nutritional deficiency worldwide, affecting an estimated two billion people. Symptoms often develop gradually and may be present long before laboratory values reach the threshold for diagnosing frank anemia. Many practitioners recognize that symptoms of iron depletion begin when ferritin drops below 30 to 50 ng/mL, well above the lower limit of most conventional reference ranges.
Common symptoms of iron deficiency include:
- Fatigue and low energy: Often the earliest and most prominent symptom. Iron is essential for mitochondrial energy production via the electron transport chain. Patients often describe a bone-deep exhaustion that is not relieved by rest.
- Hair loss: Iron deficiency is one of the most common and underdiagnosed causes of diffuse hair shedding (telogen effluvium). Many dermatologists now recommend maintaining ferritin above 40 to 70 ng/mL for optimal hair growth.
- Restless legs syndrome: A compelling urge to move the legs, especially at rest and in the evening. Research consistently shows that low ferritin, particularly below 50 ng/mL, is a significant risk factor for restless legs. Iron supplementation can provide dramatic improvement.
- Pica: Unusual cravings for non-food substances such as ice (pagophagia), dirt, clay, starch, or chalk. Ice chewing is an especially common and specific sign of iron deficiency.
- Pale skin, nail beds, and conjunctivae: Reduced hemoglobin leads to decreased red coloration of the skin and mucous membranes.
- Brittle nails (koilonychia): Nails may become thin, brittle, ridged, or spoon-shaped (concave). Spoon nails are a classic physical exam finding of iron deficiency.
- Shortness of breath on exertion: Reduced oxygen-carrying capacity from low hemoglobin leads to dyspnea with physical activity.
- Cold intolerance: Iron is necessary for thyroid hormone production and thermoregulation.
- Poor concentration and brain fog: Iron is required for dopamine and serotonin synthesis, and iron deficiency impairs cognitive function.
- Frequent infections: Iron supports immune cell proliferation and function.
- Angular cheilitis: Cracking at the corners of the mouth.
- Glossitis: A smooth, sore, swollen tongue.
Symptoms of Iron Overload
Iron overload is far less common than iron deficiency but can be equally or more dangerous because excess iron acts as a potent oxidant. The classic triad of hereditary hemochromatosis is sometimes described as bronze diabetes because of the combination of skin bronzing, diabetes mellitus, and liver cirrhosis. However, symptoms of iron overload are often subtle in the early stages and frequently misattributed to other conditions.
- Fatigue and weakness: Paradoxically, both iron deficiency and iron overload cause fatigue, which is one reason the full panel is important for proper differential diagnosis.
- Joint pain: Particularly in the knuckles of the index and middle fingers (the second and third metacarpophalangeal joints). Iron deposits in joint cartilage cause an arthropathy that mimics osteoarthritis.
- Abdominal pain: Typically right upper quadrant, reflecting liver involvement.
- Liver damage: Ranging from elevated liver enzymes to fibrosis, cirrhosis, and increased risk of hepatocellular carcinoma.
- Skin bronzing or hyperpigmentation: A grayish-bronze discoloration of the skin.
- Diabetes mellitus: Iron deposition in the pancreas damages beta cells and impairs insulin secretion.
- Cardiac problems: Iron deposition in the heart can cause cardiomyopathy, arrhythmias, and heart failure.
- Hypogonadism and decreased libido: Iron deposition in the pituitary gland disrupts gonadotropin secretion.
- Hypothyroidism: Iron deposition in the thyroid gland impairs hormone production.
- Increased susceptibility to certain infections: Some bacteria thrive in iron-rich environments.
Populations at Risk
Certain groups are disproportionately affected by iron imbalances and should be screened more proactively:
Populations at Risk for Iron Deficiency
- Menstruating women: Monthly blood loss is the single largest cause of iron deficiency in premenopausal women. Women with heavy menstrual bleeding (menorrhagia) are at particularly high risk and may lose 30 to 40 mg of iron per cycle compared to the average 15 to 20 mg.
- Pregnant women: Iron requirements increase dramatically during pregnancy to support expanded blood volume, placental development, and fetal growth. The total iron cost of pregnancy is approximately 1,000 mg, and most women enter pregnancy with insufficient stores.
- Vegetarians and vegans: Plant-based diets provide only non-heme iron, which has significantly lower bioavailability (2 to 20 percent absorption) compared to heme iron from animal sources (15 to 35 percent absorption). Vegetarians may need up to 1.8 times more dietary iron than omnivores.
- Endurance athletes: Athletes experience iron losses through foot-strike hemolysis (mechanical destruction of red blood cells), gastrointestinal blood loss from exercise-induced gut permeability, and sweat losses. Female endurance athletes are at the highest risk.
- Frequent blood donors: Each whole blood donation removes approximately 200 to 250 mg of iron. Regular donors who give every 8 weeks can rapidly deplete their iron stores without supplementation.
- Individuals with gastrointestinal conditions: Celiac disease, inflammatory bowel disease, H. pylori infection, low stomach acid (hypochlorhydria), and gastric bypass surgery all impair iron absorption.
- Growing children and adolescents: Rapid growth increases iron demands significantly.
- Elderly individuals: Reduced stomach acid production and dietary changes contribute to iron deficiency in older adults.
Populations at Risk for Iron Overload
- Individuals of Northern European descent: The HFE gene mutation causing hereditary hemochromatosis is most prevalent in populations of Celtic, Scandinavian, and Northern European ancestry, with a carrier frequency of approximately 1 in 8 to 10 individuals.
- Men and postmenopausal women: Without regular blood loss through menstruation, iron accumulates over time.
- Patients receiving frequent blood transfusions: Each unit of packed red blood cells contains approximately 200 to 250 mg of iron.
- Individuals with chronic liver disease: Impaired hepatic regulation of iron metabolism can lead to iron accumulation.
Iron Absorption Factors
Understanding the factors that enhance or inhibit iron absorption is essential for optimizing iron status through dietary and supplementation strategies.
Heme vs. Non-Heme Iron
Dietary iron exists in two forms. Heme iron is found exclusively in animal-derived foods (red meat, poultry, fish, organ meats) and is absorbed through a dedicated intestinal transporter at a rate of 15 to 35 percent. Its absorption is relatively resistant to dietary inhibitors. Non-heme iron is found in plant foods (legumes, leafy greens, fortified grains, nuts, seeds) and is absorbed at a much lower rate of 2 to 20 percent. Non-heme iron absorption is highly sensitive to the presence of enhancers and inhibitors consumed at the same meal.
Absorption Enhancers
- Vitamin C (ascorbic acid): The most potent enhancer of non-heme iron absorption. Vitamin C reduces ferric iron (Fe3+) to ferrous iron (Fe2+), the form that is absorbed by intestinal enterocytes. Consuming as little as 25 to 75 mg of vitamin C with a meal can increase non-heme iron absorption by 3 to 6 fold. Practical sources include citrus fruits, bell peppers, strawberries, tomatoes, and broccoli.
- Organic acids: Citric acid, malic acid, and lactic acid (from fermented foods) also enhance non-heme iron absorption.
- Heme iron: Consuming small amounts of meat alongside plant-based iron sources enhances non-heme iron absorption, known as the meat factor.
- Cooking in cast iron: Acidic foods cooked in cast iron cookware can absorb significant amounts of iron from the pan.
- Stomach acid: Adequate hydrochloric acid in the stomach is necessary to solubilize and reduce iron for absorption. Low stomach acid, often caused by proton pump inhibitors or aging, significantly impairs iron absorption.
Absorption Inhibitors
- Tannins: Found in tea (especially black tea), coffee, red wine, and dark chocolate. Tannins bind iron in the gut and can reduce absorption by 50 to 70 percent. Tea and coffee should be consumed at least one hour before or after iron-rich meals.
- Phytates (phytic acid): Found in whole grains, legumes, nuts, and seeds. Phytates chelate iron and reduce its bioavailability. Soaking, sprouting, and fermenting these foods significantly reduces phytate content and improves iron absorption.
- Calcium: Doses above 300 mg inhibit both heme and non-heme iron absorption. Calcium supplements and dairy products should be separated from iron-rich meals by at least two hours.
- Polyphenols: Found in many plant foods and beverages, polyphenols can bind iron. While these compounds have many health benefits, they should be separated from iron supplementation.
- Oxalates: Found in spinach, Swiss chard, rhubarb, and beet greens. Despite being rich in total iron, spinach has poor iron bioavailability due to its high oxalate content.
- Proton pump inhibitors and antacids: By reducing stomach acid, these medications significantly impair iron absorption.
Natural Strategies for Improving Iron Status
Before reaching for supplements, a functional medicine approach prioritizes identifying and addressing root causes of iron deficiency and optimizing dietary iron intake and absorption.
- Identify and address the root cause: Investigate why iron is low. Heavy menstrual bleeding may point to hormonal imbalances, fibroids, or copper deficiency. Poor absorption may indicate celiac disease, H. pylori, low stomach acid, or inflammatory bowel disease. Chronic blood loss may stem from gastrointestinal sources including ulcers or polyps.
- Increase heme iron intake: Organ meats, particularly liver, are the most iron-dense foods available. Beef liver provides approximately 6 mg of highly bioavailable heme iron per 3-ounce serving. Red meat, dark poultry meat, oysters, clams, mussels, and sardines are also excellent sources.
- Pair plant iron sources with vitamin C: Add lemon juice to lentil soup, eat bell peppers alongside beans, or serve tomato sauce with iron-fortified pasta. This simple strategy can dramatically improve non-heme iron absorption.
- Optimize stomach acid: Consider apple cider vinegar or digestive bitters before meals to stimulate hydrochloric acid production. Address any H. pylori infection. Review proton pump inhibitor use with a healthcare provider.
- Separate iron inhibitors from iron-rich meals: Drink tea and coffee between meals rather than with them. Take calcium supplements at a different meal than iron-rich foods.
- Soak, sprout, and ferment grains and legumes: These traditional food preparation methods reduce phytate content and significantly improve mineral bioavailability.
- Cook with cast iron: Particularly effective with acidic foods like tomato sauce, which can leach meaningful amounts of iron from cast iron cookware.
- Support gut health: A healthy intestinal lining is essential for iron absorption. Address intestinal permeability, dysbiosis, and any inflammatory conditions that may impair absorption.
Iron Supplementation Guidelines
When dietary strategies are insufficient, iron supplementation may be necessary. However, indiscriminate iron supplementation carries risks and should be guided by laboratory testing.
Forms of Iron Supplements
- Ferrous bisglycinate (iron bisglycinate chelate): Generally the best-tolerated oral form with good bioavailability and significantly fewer gastrointestinal side effects than other forms. This is the preferred form in functional medicine practice.
- Ferrous sulfate: The most commonly prescribed form and the least expensive. However, it frequently causes nausea, constipation, and abdominal cramping. Bioavailability is adequate but gastrointestinal tolerance is poor for many patients.
- Ferrous gluconate: Somewhat better tolerated than ferrous sulfate but provides less elemental iron per dose.
- Iron polysaccharide complex: Better tolerated but lower bioavailability.
- Ferrous fumarate: High elemental iron content but similar side effect profile to ferrous sulfate.
- Lactoferrin with iron: Lactoferrin is a glycoprotein that enhances iron absorption and may improve tolerance. Some studies show lactoferrin alone can raise ferritin levels.
Dosing Considerations
- Typical therapeutic doses range from 25 to 60 mg of elemental iron per day for mild to moderate deficiency. Severe deficiency may require higher doses initially.
- Alternate-day dosing: Emerging research suggests that taking iron every other day rather than daily may improve absorption. Oral iron triggers a hepcidin surge that suppresses absorption for approximately 24 hours. By dosing every 48 hours, the hepcidin levels normalize, and the next dose is absorbed more efficiently.
- Take on an empty stomach with vitamin C for maximum absorption, or take with a small amount of food if gastrointestinal side effects occur.
- Avoid taking iron with: Calcium supplements, dairy products, tea, coffee, antacids, proton pump inhibitors, zinc supplements, or thyroid medications. Separate by at least two hours.
- Duration: Hemoglobin typically begins to improve within 2 to 4 weeks. Replenishing ferritin stores requires 3 to 6 months of supplementation after hemoglobin normalizes.
Important Cautions
- Never supplement iron without testing: Iron overload is dangerous and supplementation in someone with undiagnosed hemochromatosis can cause serious organ damage.
- Iron is the leading cause of fatal poisoning in children: All iron supplements must be kept in child-proof containers and stored safely out of reach.
- Intravenous iron may be necessary when oral supplementation is poorly tolerated, malabsorption is present, or rapid repletion is required. IV iron infusions should be administered under medical supervision.
When to Retest
Timing follow-up testing appropriately is important to assess whether interventions are working and to avoid premature adjustments.
- After starting iron supplementation: Recheck the full iron panel and CBC in 8 to 12 weeks. Hemoglobin may begin rising within 2 to 4 weeks, but ferritin repletion takes much longer.
- After achieving target ferritin: Recheck in 3 to 4 months to ensure levels are maintained, then every 6 to 12 months for ongoing monitoring.
- During pregnancy: Iron panel should be checked at the first prenatal visit, at the start of the second trimester, and at the start of the third trimester at minimum.
- If symptoms recur: Retest promptly if symptoms of iron deficiency or overload return, regardless of the scheduled monitoring timeline.
- For hemochromatosis patients: Transferrin saturation and ferritin should be monitored every 2 to 3 months during active phlebotomy treatment, then every 3 to 6 months during maintenance.
- Testing conditions: For the most accurate and consistent results, draw the iron panel fasting, in the morning, and after avoiding iron supplements for at least 24 hours before the blood draw. Some practitioners recommend discontinuing iron supplements for 48 to 72 hours before testing.
Related Tests
A comprehensive iron panel provides valuable information, but it is most powerful when interpreted alongside several related tests:
- Complete Blood Count (CBC): The CBC reveals hemoglobin, hematocrit, red blood cell count, and red blood cell indices (MCV, MCH, MCHC, RDW). In iron deficiency, the CBC typically shows microcytic (low MCV) and hypochromic (low MCH and MCHC) red blood cells with an elevated RDW (red cell distribution width), reflecting the production of smaller, paler red blood cells with greater variability in size. The CBC is essential for determining whether iron deficiency has progressed to actual anemia.
- Reticulocyte count: Reticulocytes are immature red blood cells recently released from the bone marrow. A low reticulocyte count in the context of anemia suggests the bone marrow is not producing red blood cells adequately, which may be due to iron deficiency, B12 or folate deficiency, or bone marrow disorders. An elevated reticulocyte count after starting iron supplementation is a positive early sign that the bone marrow is responding and producing new red blood cells.
- C-Reactive Protein (CRP): CRP is a general marker of systemic inflammation. When CRP is elevated, ferritin levels must be interpreted with extreme caution because ferritin rises as part of the acute phase response regardless of iron stores. A high ferritin with a high CRP does not rule out iron deficiency. Some practitioners use an adjusted ferritin threshold of 100 ng/mL (rather than 30 ng/mL) to diagnose iron deficiency when inflammation is present.
- Soluble transferrin receptor (sTfR): This marker rises in true iron deficiency and is not affected by inflammation, making it valuable for distinguishing iron deficiency from anemia of chronic disease when ferritin is unreliable.
- Peripheral blood smear: Visual examination of red blood cell morphology can reveal target cells, pencil cells, or other abnormal shapes associated with iron deficiency or other anemias.
- HFE gene testing: Recommended when iron overload is suspected based on elevated transferrin saturation and ferritin. Tests for the C282Y and H63D mutations associated with hereditary hemochromatosis.
- Vitamin B12 and folate: Should be assessed alongside iron because combined deficiencies are common and can mask each other on the CBC. A combined iron and B12 deficiency may produce a normal MCV because microcytosis from iron deficiency and macrocytosis from B12 deficiency cancel each other out.
- Copper and ceruloplasmin: Copper is required for iron metabolism through the enzyme ceruloplasmin, which converts ferrous iron to ferric iron for loading onto transferrin. Copper deficiency can cause iron deficiency anemia that is refractory to iron supplementation.
Research Papers and References
The following are curated PubMed literature searches covering the evidence base for iron panel testing, interpretation, and clinical management. Each link opens a live, filtered PubMed query so the results stay current as new studies are indexed.
- Iron deficiency anemia diagnosis — PubMed literature search
- Ferritin inflammation — PubMed literature search
- Hereditary hemochromatosis HFE — PubMed literature search
- Transferrin saturation clinical — PubMed literature search
- Iron absorption hepcidin — PubMed literature search
- Anemia of chronic disease — PubMed literature search
- Iron deficiency restless legs — PubMed literature search
- Iron supplementation oral — PubMed literature search
- Intravenous iron therapy — PubMed literature search
- Iron overload cardiac — PubMed literature search
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — Clinical Laboratory Reference
Connections
- Iron Absorption & the Hepcidin Gate — interactive animation
- Iron
- Relationship Between Hemoglobin and Ceruloplasmin — why ceruloplasmin (the copper ferroxidase) is required to load iron into hemoglobin, and why "iron-deficiency anemia" is often functional copper deficiency.
- Anemia
- Hemochromatosis
- Complete Blood Count
- Iron Deficiency Anemia
- Heme vs Non-Heme Iron
- Berberine and Iron Overload
- Copper-Iron Dysregulation
- Iron Overload Hidden Toxicity
- Copper
- Vitamin C
- Liver Disease
- Fatigue
- Hair Loss
- Diabetes
- Methemoglobinemia and G6PD Deficiency