Iron-Deficiency Anemia
Interactive Visualization Iron Absorption & the Hepcidin Gate Watch vitamin C unlock plant iron and hepcidin slam the gate shut — then see why inflammation makes ferritin lie. Launch → Interactive Visualization Hemoglobin & the O₂ Curve — bend the oxygen curve Load oxygen onto hemoglobin one cooperative step at a time to draw the S-curve — then shift it with exercise, watch carbon monoxide lock it shut, or switch to fetal hemoglobin. Launch →
Table of Contents
- What is Iron-Deficiency Anemia?
- Stages of Iron Deficiency
- Causes and Risk Factors
- Symptoms
- Diagnosis and Lab Tests
- Conventional Treatment
- Nutritional and Natural Approaches
- Complications
- Prognosis
- Prevention
- Key Research Papers
- Connections
- Featured Videos
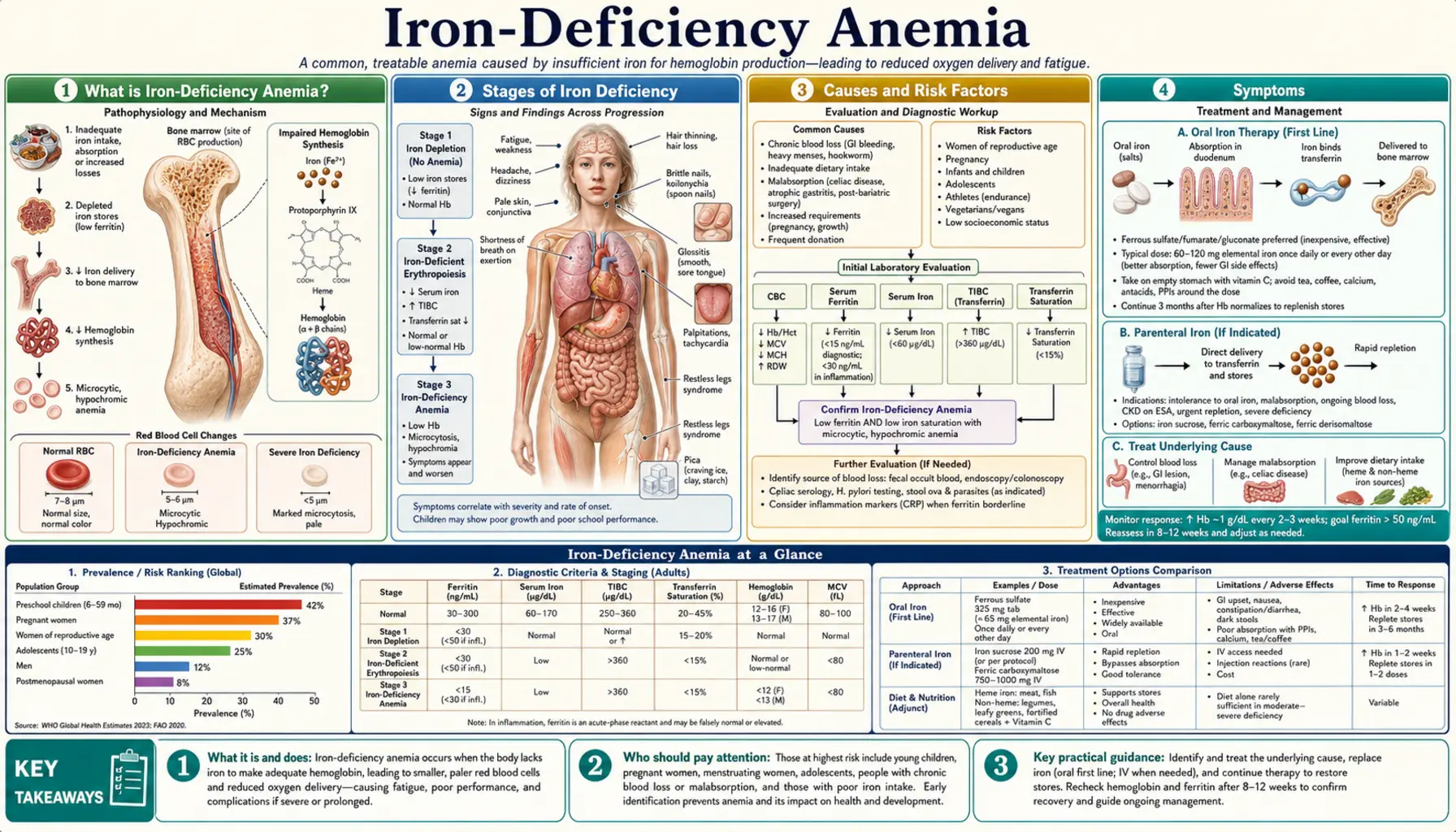
What is Iron-Deficiency Anemia?
Iron-deficiency anemia (IDA) is the most common nutritional deficiency and the leading cause of anemia worldwide. The World Health Organization estimates that approximately 1.6 billion people — roughly 24% of the global population — are affected, with the highest burden falling on preschool-age children, pregnant women, and women of reproductive age in low- and middle-income countries. In the United States alone, IDA affects around 10 million people, though iron deficiency without overt anemia is even more prevalent.
At its core, iron-deficiency anemia results from an insufficient supply of iron to meet the body's demands for hemoglobin synthesis. Hemoglobin is the iron-containing protein inside red blood cells (RBCs) that binds and transports oxygen from the lungs to every tissue in the body. Iron also forms the active center of myoglobin (oxygen storage in muscle), cytochromes (mitochondrial electron transport), and dozens of iron-dependent enzymes involved in DNA synthesis, neurotransmitter production, and immune function.
When iron stores fall below a critical threshold, the bone marrow cannot produce enough functional hemoglobin. The resulting red blood cells are smaller than normal (microcytic) and contain less hemoglobin than normal (hypochromic), reducing the blood's oxygen-carrying capacity. Tissues starved of oxygen produce the cardinal symptoms: persistent fatigue, pallor, and shortness of breath on exertion.
Despite being highly treatable — often within weeks of starting iron replacement — IDA frequently goes undiagnosed for months or years. Its symptoms overlap with dozens of other conditions, and mild deficiency produces subtle cognitive and physical impairment that patients may normalize as "just being tired." Understanding its causes, staged progression, and full symptom profile is essential for prompt recognition and treatment.
Stages of Iron Deficiency
Iron deficiency progresses through three distinct stages before clinical anemia becomes apparent. Recognizing the earlier stages matters because cognitive impairment, fatigue, and other functional consequences can begin before hemoglobin drops below diagnostic thresholds.
Stage 1 — Iron Depletion (Pre-Latent Deficiency)
In the first stage, iron stores in the bone marrow, liver, and spleen become depleted. Serum ferritin falls below 30 ng/mL (some guidelines use 12 ng/mL as the lower cutoff, but functional deficiency often begins at higher levels). Hemoglobin remains normal. Red blood cell size and morphology are also still normal at this stage. Most patients are entirely asymptomatic, and routine complete blood counts (CBCs) appear unremarkable — making ferritin the key screening test when iron deficiency is suspected before anemia develops.
Stage 2 — Iron-Deficient Erythropoiesis (Latent Deficiency)
As stores continue to fall, the supply of iron to the bone marrow becomes insufficient to fully meet erythropoietic demand, even though hemoglobin has not yet dropped below diagnostic thresholds. Hallmark lab findings at this stage include:
- Serum iron: decreased (typically below 60 mcg/dL)
- Total iron-binding capacity (TIBC) and transferrin: elevated (the body upregulates transferrin production to scavenge more iron)
- Transferrin saturation: falls below 20%
- Zinc protoporphyrin: elevated (the enzyme ferrochelatase incorporates zinc instead of iron into protoporphyrin when iron is scarce)
- Reticulocyte hemoglobin content (CHr or RetHe): falls — an early, sensitive marker of functional iron deficiency
- Hemoglobin: still normal or at the low end of normal
Subtle fatigue, reduced exercise tolerance, and mild cognitive changes may already be present in Stage 2, even without overt anemia.
Stage 3 — Iron-Deficiency Anemia (Frank Deficiency)
In the final stage, iron supply to the marrow is so depleted that newly produced red blood cells are smaller and paler than normal. The CBC now shows:
- Hemoglobin below 13 g/dL in adult men, below 12 g/dL in adult non-pregnant women, and below 11 g/dL in pregnant women and children under 5
- Mean corpuscular volume (MCV) below 80 fL (microcytosis)
- Mean corpuscular hemoglobin (MCH) below 27 pg
- Mean corpuscular hemoglobin concentration (MCHC) below 32 g/dL
- Peripheral smear: microcytic, hypochromic red blood cells, pencil cells (elongated RBCs), occasional target cells
The full constellation of IDA symptoms — profound fatigue, pallor, pica, koilonychia — typically emerges in Stage 3.
Causes and Risk Factors
Iron-deficiency anemia arises when iron losses or demands chronically exceed dietary intake and absorption. The three broad mechanisms — inadequate intake, impaired absorption, and excess loss — often overlap in the same patient.
Inadequate Dietary Intake
Dietary iron comes in two forms with very different bioavailability. Heme iron (found in red meat, poultry, and fish) is absorbed at 15–35% efficiency regardless of concurrent meal composition. Non-heme iron (found in legumes, grains, fortified foods, and vegetables) is absorbed at only 2–20% efficiency, and its absorption is heavily influenced by enhancers (vitamin C, organic acids) and inhibitors (phytates, polyphenols, calcium, oxalates) in the same meal.
Groups at risk for inadequate intake include strict vegans and vegetarians who do not carefully plan iron-rich plant-food intake, infants fed cow's milk before age 1 (cow's milk is iron-poor and can cause occult GI bleeding), toddlers and young children with limited dietary variety, elderly individuals with poor appetite or restricted diets, and individuals with food insecurity.
Impaired Absorption
Even with adequate dietary iron, certain conditions dramatically impair intestinal uptake:
- Celiac disease: Autoimmune damage to the duodenal villae — the primary site of iron absorption — is a frequently overlooked cause of refractory IDA. IDA may be the presenting symptom of silent celiac disease, particularly in adults without classic GI symptoms.
- Helicobacter pylori infection: H. pylori consumes iron for its own metabolism, reduces gastric acid (impairing conversion of ferric to ferrous iron), and causes occult gastric bleeding. H. pylori eradication alone can resolve IDA in some patients.
- Achlorhydria and proton pump inhibitor (PPI) use: Gastric acid is needed to reduce dietary ferric iron (Fe³⁺) to the absorbable ferrous form (Fe²⁺). Long-term PPI use significantly impairs non-heme iron absorption.
- Gastric bypass surgery: Roux-en-Y gastric bypass bypasses the duodenum, dramatically reducing iron absorption surface area. IDA affects 30–50% of patients within 2–5 years after surgery.
- Inflammatory bowel disease: Both Crohn's disease and ulcerative colitis cause IDA through a combination of intestinal blood loss and inflammation-driven hepcidin elevation that blocks iron absorption and release from stores.
- Hepcidin dysregulation: Hepcidin, the liver-derived master regulator of iron homeostasis, blocks ferroportin channels on enterocytes and macrophages. Chronic inflammation, infection, or obesity elevates hepcidin and can cause "functional" iron deficiency even with adequate stores.
Chronic Blood Loss
Even modest chronic bleeding can outpace the body's capacity to absorb replacement iron from the diet. One mL of blood contains approximately 0.5 mg of iron. Key sources of chronic blood loss include:
- Menorrhagia (heavy menstrual bleeding): The single most common cause of IDA in premenopausal women. Menstrual blood loss exceeding 80 mL per cycle increases iron demand to levels that dietary intake alone often cannot meet.
- Gastrointestinal bleeding: Occult GI bleeding is the most important cause to exclude in postmenopausal women and all men. Sources include peptic ulcers, gastritis, colorectal polyps, colorectal cancer, angiodysplasia (vascular malformations), esophageal varices, and diverticular disease.
- NSAID use: Aspirin and other non-steroidal anti-inflammatory drugs cause chronic gastric mucosal erosion and microbleeding, even without symptomatic ulcers.
- Parasitic infections: Hookworm (Necator americanus, Ancylostoma duodenale) is one of the leading causes of IDA globally, particularly in tropical regions. Each adult worm consumes 0.03–0.15 mL of blood per day; heavy infections of hundreds of worms produce significant daily iron loss.
- Frequent blood donation: Regular donors who do not compensate with increased dietary iron intake can develop iron depletion over time.
- Intravascular hemolysis: Mechanical heart valves, paroxysmal nocturnal hemoglobinuria (PNH), and march hemoglobinuria can produce IDA through urinary loss of hemoglobin-bound iron.
Increased Demand
- Pregnancy: Total iron requirements during pregnancy increase by approximately 1,000 mg to support fetal development, placenta growth, and the 40–50% expansion of maternal blood volume. Most women begin pregnancy with suboptimal iron stores.
- Infancy: Rapid growth from birth to 2 years requires substantial iron. Term infants exhaust maternal iron stores by 4–6 months; premature infants deplete stores even sooner.
- Adolescence: Growth spurts and, in girls, the onset of menstruation simultaneously increase iron demand during adolescence.
- Endurance athletes: Distance runners experience iron losses through foot-strike hemolysis, GI microbleeding, and sweat losses, and have higher iron turnover due to elevated erythropoiesis.
Restless Leg Syndrome Association
Iron deficiency — even without frank anemia — is strongly associated with restless leg syndrome (RLS). Iron is a cofactor for tyrosine hydroxylase, the rate-limiting enzyme in dopamine synthesis, and dopaminergic dysfunction in the substantia nigra and spinal cord is central to RLS pathophysiology. Brain iron imaging studies consistently show reduced iron in the substantia nigra of RLS patients, and iron supplementation reduces RLS severity independent of anemia status.
Symptoms
The symptoms of iron-deficiency anemia span from the classical triad of anemia to highly specific signs that reflect iron's broader roles in cellular metabolism, neurotransmitter production, and epithelial integrity.
Classical Triad
- Fatigue and weakness: The most universal symptom. Reduced oxygen delivery to muscles and tissues impairs aerobic metabolism and ATP production. Fatigue in IDA is typically disproportionate to activity level — patients describe exhaustion from tasks they previously found effortless.
- Pallor: Reduced hemoglobin causes pallor of the skin, conjunctivae, nail beds, and mucous membranes. Pallor of the conjunctival mucosa (inner lower eyelid) is a particularly reliable clinical sign.
- Exertional dyspnea: Shortness of breath on exertion reflects the cardiovascular system's compensatory effort — increased heart rate and cardiac output — to deliver adequate oxygen to tissues despite reduced hemoglobin.
Cardiovascular Symptoms
As anemia worsens, the heart must work harder to maintain oxygen delivery. Patients may experience palpitations, tachycardia at rest, dizziness, and lightheadedness (particularly on standing, producing orthostatic hypotension). Severe IDA can precipitate high-output heart failure, especially in patients with underlying cardiac disease.
Neurological and Cognitive Symptoms
Iron is essential for myelination, neurotransmitter synthesis (dopamine, serotonin, norepinephrine), and mitochondrial function in neurons. Iron deficiency — even without anemia — impairs attention, working memory, and processing speed. In children, iron deficiency during critical developmental windows causes lasting cognitive deficits, reduced school performance, and behavioral changes (irritability, reduced attention span) that may not fully reverse even after iron repletion. Adults report brain fog, difficulty concentrating, and mood disturbances.
Pica
Pica — the compulsive craving for non-nutritive substances — is a hallmark symptom of iron deficiency that often predates overt anemia. Three forms predominate:
- Pagophagia: Compulsive ice chewing or crunching. The most common and specific form associated with IDA. Some patients consume several cups of ice per day. The mechanism is unclear but may involve the cooling effect reducing oral inflammation or a sensory-seeking behavior driven by altered dopamine signaling.
- Geophagia: Craving for clay, dirt, or soil. More common in pregnant women and children in certain cultural contexts. Soil can paradoxically worsen IDA by introducing phytates and other iron chelators.
- Amylophagia: Craving for raw starch (cornstarch, raw pasta, raw rice). Also associated with IDA and zinc deficiency.
Pica resolves rapidly — often within days — after iron supplementation begins, suggesting a direct neurochemical relationship.
Epithelial and Mucosal Signs
- Koilonychia (spoon nails): The fingernails become thin, brittle, and concave — they lose their normal convex curve and can hold a drop of water. This reflects impaired keratinocyte iron metabolism. Koilonychia is highly specific for severe or long-standing IDA.
- Angular cheilitis: Painful cracking and fissuring at the corners of the mouth. Also associated with B-vitamin deficiencies and oral candidiasis, but iron deficiency is a common underlying cause.
- Glossitis: Smooth, red, painful tongue due to atrophy of the filiform papillae. Also associated with B12 and folate deficiency.
- Brittle hair and nails: Hair may become thin, dull, and break easily. Telogen effluvium (diffuse hair shedding) can occur when iron falls below optimal levels for hair follicle metabolism, even without frank anemia.
Restless Leg Syndrome
An irresistible urge to move the legs, particularly at night or at rest, relieved by movement. RLS affects up to 15% of IDA patients and may be the presenting complaint. It is caused by brain iron deficiency impairing dopaminergic circuits in the basal ganglia — even when serum markers of IDA are only mildly abnormal, cerebrospinal fluid ferritin may be profoundly low.
POTS-Like Symptoms
Postural orthostatic tachycardia syndrome (POTS) — excessive heart rate increase upon standing — overlaps significantly with IDA. Iron deficiency impairs both red cell mass (reducing venous return) and peripheral vasoconstriction (through nitric oxide dysregulation). Many patients with IDA experience significant orthostatic symptoms that improve dramatically with iron repletion.
Impaired Immune Function
Iron is required for the proliferation of T-lymphocytes and the oxidative burst of neutrophils that kills pathogens. IDA is associated with increased susceptibility to infections, impaired vaccine responses, and delayed wound healing.
Diagnosis and Lab Tests
Diagnosing IDA requires integrating multiple laboratory tests, since no single value is both perfectly sensitive and specific across all clinical contexts. The goal is to confirm iron deficiency as the cause of anemia and then identify the underlying etiology — particularly to exclude serious pathology such as GI malignancy.
Complete Blood Count (CBC)
The CBC is the standard first step. Key findings in established IDA include:
- Hemoglobin: Below 13 g/dL in adult men; below 12 g/dL in non-pregnant adult women; below 11 g/dL in pregnant women and children under 5 years (WHO thresholds)
- MCV (Mean Corpuscular Volume): Below 80 fL (microcytosis). Note that early IDA may show a normal MCV; mixed deficiency (iron + B12 or folate) can produce a "normal" MCV from averaging microcytic and macrocytic cells.
- MCH (Mean Corpuscular Hemoglobin): Below 27 pg (hypochromia)
- MCHC (Mean Corpuscular Hemoglobin Concentration): Below 32 g/dL
- RDW (Red Cell Distribution Width): Elevated (above 14.5%) — reflects anisocytosis (variation in RBC size) as the marrow produces a mixed population of iron-deficient and residual normal cells
- Reticulocyte count: Low or inappropriately normal for the degree of anemia (hypoproliferative pattern)
- Platelet count: May be elevated (reactive thrombocytosis) — a common but underappreciated finding in IDA, reflecting shared thrombopoietin signaling
Iron Studies
- Serum ferritin: The most sensitive and specific single marker of iron stores. Below 30 ng/mL is suggestive; below 10–12 ng/mL is diagnostic of iron depletion. Critical caveat: ferritin is an acute-phase reactant and rises sharply with inflammation, infection, liver disease, or malignancy, masking true iron deficiency. In the setting of chronic inflammation, a ferritin up to 100 ng/mL may still be compatible with iron deficiency.
- Serum iron: Total iron circulating bound to transferrin. Below 60 mcg/dL in IDA. Highly variable across the day (diurnal variation up to 30%) and falls acutely with infection or inflammation.
- Total iron-binding capacity (TIBC) / Transferrin: TIBC above 400 mcg/dL (transferrin above 380 mg/dL) in IDA — the body upregulates transferrin production to capture more iron. Elevated TIBC in the context of low serum iron strongly supports IDA.
- Transferrin saturation: Serum iron divided by TIBC, expressed as a percentage. Below 20% (some labs use 15%) is characteristic of IDA. Below 10% indicates severe depletion. Transferrin saturation is low in IDA but also low in anemia of chronic inflammation — ferritin level helps distinguish the two (low in IDA, elevated in ACI).
Advanced Markers
- Reticulocyte hemoglobin content (CHr or RetHe): Reflects real-time iron availability to the marrow over the preceding 1–2 days. Below 28–29 pg indicates functional iron deficiency and is particularly useful in diagnosing iron-restricted erythropoiesis in the setting of inflammation or after IV iron treatment.
- Soluble transferrin receptor (sTfR): Elevated in IDA (elevated demand for iron uptake increases receptor expression) but remains normal in anemia of chronic disease. The sTfR-to-log ferritin ratio (Thomas plot) helps distinguish the two when both conditions may coexist.
- Zinc protoporphyrin (ZPP): When iron is unavailable, ferrochelatase substitutes zinc for iron in protoporphyrin IX, producing zinc protoporphyrin. Elevated ZPP is a sensitive marker of iron-restricted erythropoiesis and lead poisoning.
Peripheral Blood Smear
Direct microscopic examination of a stained blood smear provides morphological confirmation. In IDA, smears show microcytic hypochromic RBCs with an enlarged central pallor zone (normally less than one-third of cell diameter; in IDA it may exceed two-thirds), pencil cells (elongated elliptocytes specific to IDA), and occasional target cells. The smear also helps exclude thalassemia (which shows similar microcytosis but with different morphological pattern) and sideroblastic anemia.
Bone Marrow Biopsy
The gold standard for assessing iron stores — absence of iron-staining (Prussian blue/Perls' stain) in marrow macrophages confirms iron deficiency with 100% specificity. However, bone marrow biopsy is invasive and rarely required for diagnosing straightforward IDA. It is reserved for complex cases where non-invasive tests are inconclusive, where refractory anemia requires further investigation, or when a marrow disorder is suspected.
Investigating the Cause
Identifying why a patient is iron-deficient is at least as important as confirming the diagnosis. In adult men and postmenopausal women, IDA must be presumed to originate from GI blood loss until proven otherwise — fecal occult blood testing, upper endoscopy, and colonoscopy are standard. In premenopausal women, menstrual history is paramount. Celiac serology (IgA anti-tissue transglutaminase antibody) should be checked when malabsorption is suspected. H. pylori testing (stool antigen or urea breath test) is appropriate in many adults with unexplained IDA.
Conventional Treatment
Treatment of IDA has two simultaneous goals: replace iron stores to restore hemoglobin and tissue iron, and identify and treat the underlying cause to prevent recurrence.
Oral Iron Supplementation
Oral iron remains the first-line therapy for most patients with IDA due to its efficacy, low cost, and safety profile. The three most widely used oral iron salts are:
- Ferrous sulfate: 325 mg tablets contain 65 mg elemental iron. The standard regimen is 325 mg two to three times daily (yielding 130–195 mg elemental iron/day), though evidence increasingly supports that lower, less frequent dosing (e.g., 40–60 mg elemental iron every other day) may achieve equivalent absorption with significantly fewer GI side effects by reducing hepcidin induction between doses.
- Ferrous gluconate: 325 mg tablets contain 36 mg elemental iron. Slightly better GI tolerability than ferrous sulfate due to lower elemental iron per dose.
- Ferrous fumarate: 200 mg tablets contain 66 mg elemental iron. Higher elemental iron per tablet but similar tolerability to ferrous sulfate.
Optimizing Oral Iron Absorption
- Take with vitamin C: 100–200 mg of vitamin C (ascorbic acid) taken simultaneously with iron reduces ferric iron (Fe³⁺) to the more absorbable ferrous form (Fe²⁺) and forms a soluble chelate that resists precipitation at intestinal pH. This is one of the most effective ways to enhance non-heme iron absorption.
- Take on an empty stomach: Iron absorption is highest when taken 30–60 minutes before meals. Food — particularly dairy, eggs, tea, coffee, and high-phytate grains — substantially reduces absorption. However, GI tolerability is better with food; a reasonable compromise for patients with significant nausea is to take iron with a small amount of food while avoiding the highest-inhibitor foods.
- Avoid concurrent medications: Antacids, proton pump inhibitors, H2 blockers, calcium supplements, and magnesium supplements should be separated from iron by at least 2 hours. Tetracycline antibiotics, fluoroquinolones, and levodopa chelate iron and must be spaced apart.
- Alternate-day dosing: Research by Moretti et al. (2015) demonstrated that oral iron acutely raises serum hepcidin for approximately 24 hours, suppressing absorption of the next dose. Dosing every other day (or even every third day) may paradoxically result in higher cumulative absorption than daily dosing by taking advantage of the hepcidin-free window.
Managing GI Side Effects
Nausea, constipation, diarrhea, dark stools, and abdominal cramping affect 10–40% of patients on oral iron and are the leading cause of non-adherence. Strategies include:
- Starting at a lower dose and titrating up over 1–2 weeks
- Switching to a better-tolerated salt (ferrous gluconate, ferric maltol, or iron bisglycinate)
- Taking with a small amount of food
- Switching to alternate-day dosing
- Using liquid formulations to allow dose titration
- Adding a stool softener (docusate sodium) for constipation
Monitoring Response
A rise in reticulocyte count within 7–10 days of starting oral iron confirms the diagnosis and adequate response. Hemoglobin typically begins rising after 2–4 weeks and reaches near-normal values within 6–8 weeks. However, iron supplementation must continue for 3–6 months after hemoglobin normalizes to replenish depleted tissue stores (reflected by normalization of serum ferritin). Stopping supplementation prematurely when hemoglobin normalizes but ferritin remains low invariably leads to relapse.
Intravenous Iron
IV iron bypasses the GI tract entirely and is preferred when oral iron is ineffective, not tolerated, or when rapid iron repletion is needed. Indications include:
- Malabsorption syndromes (celiac disease, gastric bypass, inflammatory bowel disease)
- Intolerance of multiple oral iron preparations
- Severe anemia requiring rapid response (e.g., pre-operative preparation)
- Chronic kidney disease on hemodialysis (hepcidin levels make oral iron largely ineffective)
- Heart failure with IDA (IV iron improves functional capacity independent of hemoglobin)
Available IV iron formulations include ferric carboxymaltose (FCM, can deliver up to 1,000 mg in a single infusion over 15 minutes), ferumoxytol (approved for CKD, off-label for other causes), iron sucrose, ferric gluconate, and low-molecular-weight iron dextran. The older high-molecular-weight iron dextran carries higher anaphylaxis risk and is rarely used. Modern preparations have an excellent safety profile; infusion reactions are uncommon and typically mild (flushing, transient hypotension).
Blood Transfusion
Packed red blood cell (PRBC) transfusion is reserved for hemodynamically unstable patients or those with severe symptomatic anemia (typically Hb below 7–8 g/dL) who cannot wait for iron supplementation to work. Each unit of PRBCs raises hemoglobin by approximately 1 g/dL and provides about 200–250 mg of iron. Transfusion does not replenish iron stores and does not address the underlying cause — iron replacement therapy must still follow.
Treating the Underlying Cause
Without addressing the root cause of iron deficiency, replacement therapy will need to continue indefinitely or anemia will recur. Key interventions include: H. pylori eradication, gluten-free diet for celiac disease, hormonal or surgical management of menorrhagia, endoscopic or surgical treatment of GI bleeding sources, albendazole/mebendazole for hookworm, and stopping NSAIDs when safe to do so.
Nutritional and Natural Approaches
Dietary strategies and complementary approaches can meaningfully support iron repletion and help maintain iron balance after medical treatment — though they cannot substitute for supplementation or IV iron in established deficiency.
Heme vs. Non-Heme Iron Sources
Heme iron is bound within the porphyrin ring of hemoglobin and myoglobin in animal tissues. It enters intestinal enterocytes via the HCP1 (heme carrier protein 1) transporter and is absorbed at 15–35% efficiency, largely unaffected by inhibitors or enhancers in the same meal. Non-heme iron — the form in plant foods and fortified products — must be reduced to Fe²⁺ by duodenal cytochrome B (DcytB) and then transported into cells by the divalent metal transporter 1 (DMT1). Its absorption is highly variable (2–20%) and strongly influenced by concurrent food components.
The richest heme iron sources per serving include beef liver (6.2 mg/100g), chicken liver (11.6 mg/100g), oysters (7.2 mg/100g cooked), clams, sardines, beef, lamb, and dark turkey meat. These represent the most bioavailable dietary iron available.
Rich non-heme sources include white beans (8.0 mg/100g cooked), lentils (3.3 mg/100g), tofu, fortified breakfast cereals, pumpkin seeds, spinach, blackstrap molasses, dark chocolate, and quinoa. Combining these with heme iron sources or vitamin C dramatically improves absorption.
Vitamin C Co-Ingestion
Vitamin C (ascorbic acid) is the most potent dietary enhancer of non-heme iron absorption. As little as 25–50 mg of vitamin C (roughly half an orange or a small handful of strawberries) can increase non-heme iron absorption two- to threefold by maintaining iron in its soluble Fe²⁺ form and countering the inhibitory effects of phytates and polyphenols. Practical applications: squeeze lemon over spinach salad, eat strawberries with fortified oatmeal, or pair lentils with tomato-based sauces.
Copper's Essential Role
Copper is an often-overlooked but metabolically essential partner for iron utilization. The copper-containing enzyme ceruloplasmin (a ferroxidase) is required to oxidize Fe²⁺ back to Fe³⁺ so iron can be loaded onto transferrin for transport through the bloodstream. Without adequate ceruloplasmin activity, iron absorbed by the gut becomes trapped in enterocytes and macrophages and cannot enter the circulation — producing an "iron sequestration" anemia that mimics IDA and does not respond to iron supplementation alone. Liver, oysters, shellfish, nuts, and seeds are the richest copper sources. Excessive zinc supplementation (above 50 mg/day) competitively blocks copper absorption and can produce copper-deficiency-mediated anemia.
Reducing Iron Inhibitors
For individuals relying heavily on plant iron sources, minimizing inhibitors at the same meal makes a meaningful difference:
- Phytates: Found in grains, legumes, and seeds. Soaking, sprouting, and fermentation (e.g., sourdough bread) significantly reduce phytate content and improve iron bioavailability.
- Polyphenols: Tea, coffee, red wine, and dark chocolate contain polyphenols (including tannins) that bind iron in the gut. Avoiding tea and coffee within 1 hour of meals can improve iron absorption by 30–50% in iron-deficient individuals.
- Calcium: Both heme and non-heme iron absorption are inhibited by calcium at the same meal. Separate calcium supplements and dairy-heavy foods from iron-rich meals when possible.
- Egg whites: Contain phosvitin, a potent iron chelator. Despite their overall nutritional value, egg whites inhibit iron absorption from a shared meal.
Cooking in Cast Iron Cookware
Cooking acidic foods (tomato sauce, lemon-based dishes, applesauce) in cast iron pots and pans leaches small but meaningful amounts of iron into the food. Studies show that using cast iron for acidic, liquid-containing dishes can increase iron content two- to tenfold compared to cooking in other materials. While not a substitute for supplementation, it provides a consistent daily boost that can matter at the margins.
Lactoferrin
Lactoferrin is an iron-binding glycoprotein naturally found in human breast milk, saliva, and other secretions. Oral bovine lactoferrin supplements have shown promise in small trials as an alternative to ferrous sulfate for mild-to-moderate IDA, with reported similar hemoglobin recovery but significantly better GI tolerability. Lactoferrin may also modulate hepcidin expression and have anti-inflammatory effects that secondarily improve functional iron availability. It is particularly worth considering for pregnant women or individuals who cannot tolerate standard iron salts, though evidence from large randomized trials is still accumulating.
Beetroot and Folate-Rich Foods
While beets contain relatively modest iron (0.8 mg/100g), they are rich in folate and nitrates that support erythropoiesis and vascular health. Folate is required for DNA synthesis in rapidly dividing red blood cell precursors; folate deficiency can co-exist with IDA and impair the hematological response to iron treatment. Dark leafy greens (spinach, kale, Swiss chard) deliver both non-heme iron and folate, though cooking is needed to reduce oxalates that inhibit mineral absorption from raw leaves.
Complications
When iron-deficiency anemia goes untreated or is inadequately managed, it produces systemic consequences that extend far beyond reduced hemoglobin. Many of these complications — particularly those affecting children and pregnant women — can have permanent, irreversible effects.
Cardiac Complications
The heart compensates for reduced oxygen-carrying capacity by increasing heart rate and stroke volume, raising cardiac output. Sustained high-output state leads to cardiac remodeling: chamber dilation, left ventricular hypertrophy, and eventually high-output heart failure. Even mild anemia increases cardiovascular mortality in patients with existing heart disease, and IDA independently predicts worse outcomes in heart failure independent of anemia itself — because cardiac myocytes require iron for mitochondrial function and energy production beyond what hemoglobin delivers.
Adverse Pregnancy Outcomes
IDA during pregnancy is a major driver of maternal and infant mortality worldwide:
- Preterm birth (before 37 weeks gestation) — risk increased 1.5- to 2-fold with maternal IDA
- Low birth weight (below 2,500 g) — iron-deficient placental function impairs fetal growth
- Increased maternal mortality — severe IDA during and after delivery dramatically increases the risk of death from hemorrhagic shock, as there is no reserve hemoglobin to tolerate even modest blood loss
- Impaired fetal iron stores — the fetal brain accumulates most of its iron supply in the third trimester; maternal IDA depletes these stores, placing infants at risk of brain iron deficiency from birth
- Postpartum depression — iron deficiency impairs serotonin and dopamine synthesis, increasing risk of postpartum mood disorders
Cognitive and Developmental Impairment in Children
This is arguably the most consequential complication of IDA at the population level. Iron is critical for myelination of axons, synaptic development, and the dopaminergic circuits of the basal ganglia during early childhood. Infants and toddlers with IDA show reduced scores on Bayley Scales of Infant Development, impaired language acquisition, reduced attention span, and behavioral abnormalities including increased fearfulness and reduced social engagement. Studies of children who had IDA in infancy show lasting cognitive disadvantage at age 10 and beyond — even after iron was repleted — suggesting there is a window of vulnerability during early development when iron deficiency causes irreversible harm.
Impaired Immune Function
Iron-deficient lymphocytes proliferate poorly after antigenic stimulation, natural killer cell cytotoxicity is reduced, and neutrophil myeloperoxidase activity is impaired. IDA patients have increased susceptibility to bacterial and viral infections and reduced seroconversion rates after vaccination. However, an important counterintuitive principle: iron supplementation in malaria-endemic regions should be done cautiously and ideally combined with malaria prophylaxis, as free iron promotes Plasmodium falciparum growth.
Reduced Exercise Capacity and Work Performance
Even when anemia is corrected, iron deficiency impairs mitochondrial function in skeletal muscle through reduced iron-sulfur cluster enzyme activity and cytochrome c oxidase activity. Studies of iron-deficient non-anemic adults show measurable reductions in VO₂ max, endurance, and work productivity that improve with iron supplementation independent of hemoglobin changes.
Restless Leg Syndrome Progression
Untreated iron deficiency perpetuates RLS, which causes chronic sleep disruption, daytime fatigue, and significantly impairs quality of life. Severe RLS is associated with increased cardiovascular disease risk, likely mediated by sleep deprivation and sympathetic nervous system activation.
Prognosis
The prognosis for iron-deficiency anemia is excellent when the underlying cause is identified and treated, and iron repletion is adequate and sustained. Most patients experience complete resolution of symptoms and normalization of all laboratory parameters with appropriate therapy.
Hematological Recovery Timeline
The sequence and timing of laboratory recovery follows a predictable pattern:
- Days 7–10: Reticulocytosis — an increase in newly produced reticulocytes in the blood, signaling that the marrow has responded to iron replacement. This reticulocyte peak is both diagnostic confirmation and the earliest measurable treatment response.
- Weeks 4–8: Hemoglobin rises by approximately 1–2 g/dL per week in a well-responding patient. Most patients reach target hemoglobin (above 12 g/dL in women, above 13 g/dL in men) within 4–8 weeks of starting treatment.
- Months 3–6: Serum ferritin normalizes as tissue stores are replenished. This is the critical endpoint for stopping supplementation — not hemoglobin recovery alone. Premature discontinuation is the most common reason for relapse.
Factors Affecting Prognosis
Failure to respond — defined as a hemoglobin rise of less than 1 g/dL after 4 weeks of appropriate oral iron — warrants reassessment. Common reasons include:
- Non-adherence due to GI side effects (switch formulation, adjust timing, consider IV iron)
- Ongoing blood loss exceeding replacement (inadequate treatment of underlying cause)
- Malabsorption (celiac disease, achlorhydria, post-bariatric anatomy)
- Incorrect diagnosis — thalassemia trait, anemia of chronic disease, or sideroblastic anemia may produce a similar CBC picture and do not respond to iron
- Concurrent nutrient deficiency (copper, B12, folate) impairing erythropoiesis
- Inflammation suppressing erythropoietin response
Long-Term Outlook
In children who developed IDA before age 2, some cognitive disadvantage may persist despite adequate iron repletion — highlighting the importance of prevention in early life rather than reliance on treatment after deficiency occurs. In adults, all functional consequences of IDA — including fatigue, pica, RLS, cognitive impairment, koilonychia, and exercise intolerance — resolve with successful iron repletion, though some epithelial changes (koilonychia) take months to fully reverse as nail growth completes.
Prevention
Prevention strategies for iron-deficiency anemia operate at the individual, clinical, and population levels. Because the risk profile varies dramatically by age, sex, and physiological state, targeted interventions are far more effective than uniform supplementation.
Dietary Counseling
Practical dietary guidance for individuals at risk includes: regularly consuming heme iron sources (red meat 2–3 times per week, poultry, fish), pairing non-heme iron sources with vitamin C, soaking or sprouting legumes and grains to reduce phytates, limiting tea and coffee within 1 hour of meals, avoiding calcium supplements at meal times, and not giving cow's milk as the primary drink to infants under 12 months. Dietitian referral is particularly valuable for vegans, vegetarians, and individuals with food insecurity or restricted diets.
Prenatal Iron Supplementation
The WHO recommends daily oral iron supplementation (30–60 mg elemental iron) plus folic acid for all pregnant women throughout pregnancy and for 6–12 weeks postpartum. In regions with high IDA prevalence (above 40%), higher doses (120 mg elemental iron daily) may be appropriate. Many women begin pregnancy with depleted stores due to prior menstrual losses, making first-trimester initiation of supplementation — rather than waiting for documented deficiency — the recommended standard of care.
Infant and Child Interventions
- Delayed umbilical cord clamping (at least 1–3 minutes after birth) transfers 75–100 mL of placental blood to the newborn, providing an additional 30–55 mg of iron — enough to support 4–6 months of healthy development
- Exclusive breastfeeding for 6 months (breast milk iron bioavailability is exceptionally high at 50%); term breastfed infants should begin iron supplementation (1 mg/kg/day) at 4 months until iron-rich complementary foods are well established
- Iron-fortified infant formulas for formula-fed infants
- Introduction of iron-rich solid foods (puréed meats, fortified cereals) at 6 months
- Avoiding cow's milk before 12 months of age
Iron Fortification of Foods
Population-level iron fortification of staple foods (wheat flour, rice, salt, infant formula) is a cost-effective public health strategy that has reduced IDA prevalence in both high- and low-income countries. In the United States, mandatory fortification of enriched flour has contributed to improved iron status across the population.
Screening in At-Risk Groups
Clinical guidelines recommend periodic screening for IDA in:
- Pregnant women — CBC and ferritin at first prenatal visit and again at 24–28 weeks
- Infants — hemoglobin or hematocrit at 12 months, earlier for premature infants
- Premenopausal women with heavy periods — ferritin annually if symptoms are present
- Adults with symptoms of GI blood loss (hematochezia, melena, iron deficiency without clear cause) — fecal occult blood testing, endoscopy as indicated
- Regular blood donors — ferritin check every 1–2 years
- Post-bariatric surgery patients — CBC, iron studies, ferritin at 6 months, then annually
Treating Underlying Conditions Proactively
Effective management of heavy menstrual bleeding (hormonal therapy, IUD, uterine fibroid treatment), eradication of H. pylori in those with a documented infection, and gluten-free diet adherence in celiac disease are among the highest-yield preventive interventions for reducing the burden of recurrent IDA.
Key Research Papers
- Camaschella C. Iron-deficiency anemia. N Engl J Med. 2015;372(19):1832–43 — Search PubMed. DOI 10.1056/NEJMra1401038
- Lopez A, Cacoub P, Macdougall IC, Peyrin-Biroulet L. Iron deficiency anaemia. Lancet. 2016;387(10021):907–16 — Search PubMed. DOI 10.1016/S0140-6736(15)60865-0
- Pasricha SR, Tye-Din J, Muckenthaler MU, Swinkels DW. Iron deficiency. Lancet. 2021;397(10270):233–248 — Search PubMed. DOI 10.1016/S0140-6736(20)32594-0
- Moretti D, Goede JS, Zeder C, et al. Oral iron supplements increase hepcidin and decrease iron absorption from daily or twice-daily doses in iron-depleted young women. Blood. 2015;126(17):1981–9. PMID 26289639. DOI 10.1182/blood-2015-05-642223
- Tolkien Z, Stecher L, Mander AP, Pereira DI, Powell JJ. Ferrous sulfate supplementation causes significant gastrointestinal side-effects in adults: a systematic review and meta-analysis. PLoS One. 2015;10(2):e0117383. PMID 25700159. DOI 10.1371/journal.pone.0117383
- Alleyne M, Horne MK, Miller JL. Individualized treatment for iron-deficiency anemia in adults. Am J Med. 2008;121(11):943–8. PMID 18954837. DOI 10.1016/j.amjmed.2008.07.012
- Daru J, Zamora J, Fernández-Félix BM, et al. Risk of maternal mortality in women with severe anaemia during pregnancy and post partum: a multilevel analysis. Lancet Glob Health. 2018;6(5):e548–e554. PMID 29571592. DOI 10.1016/S2214-109X(18)30078-0
- Zimmermann MB, Hurrell RF. Nutritional iron deficiency. Lancet. 2007;370(9586):511–20 — Search PubMed. DOI 10.1016/S0140-6736(07)61235-5
- Muñoz M, Acheson AG, Auerbach M, et al. International consensus statement on the peri-operative management of anaemia and iron deficiency. Anaesthesia. 2017;72(2):233–247. PMID 27996086. DOI 10.1111/anae.13773
- Ganz T, Nemeth E. Iron homeostasis in host defence and inflammation. Nat Rev Immunol. 2015;15(8):500–10 — Search PubMed. DOI 10.1038/nri3863
- Lozoff B, Jimenez E, Smith JB. Double burden of iron deficiency in infancy and low socioeconomic status: a longitudinal analysis of cognitive test scores to age 19 years. Arch Pediatr Adolesc Med. 2006;160(11):1108–13. PMID 17088512. DOI 10.1001/archpedi.160.11.1108
- Allen RP, Earley CJ. The role of iron in restless legs syndrome. Mov Disord. 2007;22 Suppl 18:S440–8 — Search PubMed. DOI 10.1002/mds.21607
PubMed topic searches:
- Iron deficiency anemia treatment
- Iron deficiency anemia diagnosis
- Iron deficiency anemia pregnancy
- Iron deficiency anemia children
- Oral vs intravenous iron therapy
- Iron deficiency and restless leg syndrome
- Ferritin, hepcidin, and iron absorption
- Iron deficiency cognitive development
Connections
- Hematology
- Iron Deficiency — the same anemia from the nutrition side — why low iron produces so many unrelated-looking symptoms, the vitamin C, copper and B12 cofactors, food sources, and what repletion actually feels like.
- Hemoglobin & the Oxygen Dissociation Curve — interactive animation
- Iron Absorption & the Hepcidin Gate — interactive animation
- Iron
- Anemia
- Pernicious Anemia
- Aplastic Anemia
- Hemochromatosis
- Thalassemia
- Thrombocytopenia
- Sickle Cell Disease
- Von Willebrand Disease
- Deep Vein Thrombosis
- Complete Blood Count
- Iron — Deficiency Anemia
- Fatigue
- Celiac Disease
- Hair Loss
- Vitamin C
- Copper
- Hookworm Blood Loss & Anemia — how much blood each worm drains and how that becomes anemia, the leading parasitic cause worldwide.
- Hookworm Symptoms & Diagnosis — when unexplained iron deficiency should prompt a stool exam for hookworm eggs.