Iron-Deficiency Anemia: Breathlessness and Pallor
Two of the most telling signs that iron has run low are things other people may notice before you do: you get winded doing ordinary things — a flight of stairs, a brisk walk to catch a bus, carrying laundry up to the bedroom — and your skin looks pale, especially the lips, the inner eyelids, the palms, and the beds of the fingernails. Neither symptom is glamorous and both are easy to wave away as being unfit, tired, or “just my colouring,” but together they point to a very specific problem: not enough healthy red blood cells to carry oxygen, because the body has run short of the iron it needs to build them. This page explains why low iron specifically causes breathlessness and pallor, how to tell when these signs point to iron deficiency rather than something else, and how the problem is confirmed and corrected.
Table of Contents
- What Breathlessness and Pallor Feel and Look Like
- The Mechanism: Iron, Hemoglobin, and the Oxygen Delivery Truck
- Honest Talk: These Signs Are Not Unique to Iron
- Clues That Point to Iron Deficiency
- What Drains Iron in the First Place
- Getting Tested
- Correcting Low Iron Safely
- How Fast the Breathlessness and Colour Come Back
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Breathlessness and Pallor Feel and Look Like
The breathlessness of iron-deficiency anemia is almost always exertional — it shows up when you move, not when you sit still. The technical name is dyspnea on exertion, and what people actually describe is remarkably consistent:
- Getting winded on stairs. A staircase you climbed without thinking now leaves you puffing at the top, having to pause on the landing to “catch your breath.”
- Having to slow down on the flat. Walking with friends or to catch a bus, you find yourself dropping back, unable to talk and walk briskly at the same time.
- A racing or pounding heart with the breathlessness. Many people feel their heart thumping (palpitations) at the same time, sometimes with a swooshing sound in the ears — the body's attempt to push more blood around faster.
- Light-headedness when standing or after effort, and an outsized sense of being “puffed” for the small amount of work done.
Pallor is the visible companion. Because red blood cells give blood — and therefore skin — its colour, running short of them drains the warmth from the complexion. The most reliable places to see it are where the skin is thin or the surface is naturally red:
- The conjunctiva — the inner lining of the lower eyelid. Pull the lower lid down gently: in a person with enough red cells it is a healthy salmon-pink; in significant anemia it looks pale, almost the colour of the white of the eye. This is the single most useful spot to check.
- The lips and gums, which lose their deep pink and look washed-out.
- The palms and the creases of the palm — normally the creases stay pink even when the surrounding skin pales; when even the creases lose colour, anemia is usually marked.
- The nail beds, which turn pale rather than their usual rosy pink.
Pallor is genuinely hard to judge in yourself in a mirror, and it is influenced by natural skin tone, lighting, and temperature — which is exactly why the inner eyelid and the nail beds, rather than the face, are the places clinicians look. It is also why a friend, partner, or pharmacist saying “you look pale” is worth taking seriously rather than dismissing.
The Mechanism: Iron, Hemoglobin, and the Oxygen Delivery Truck
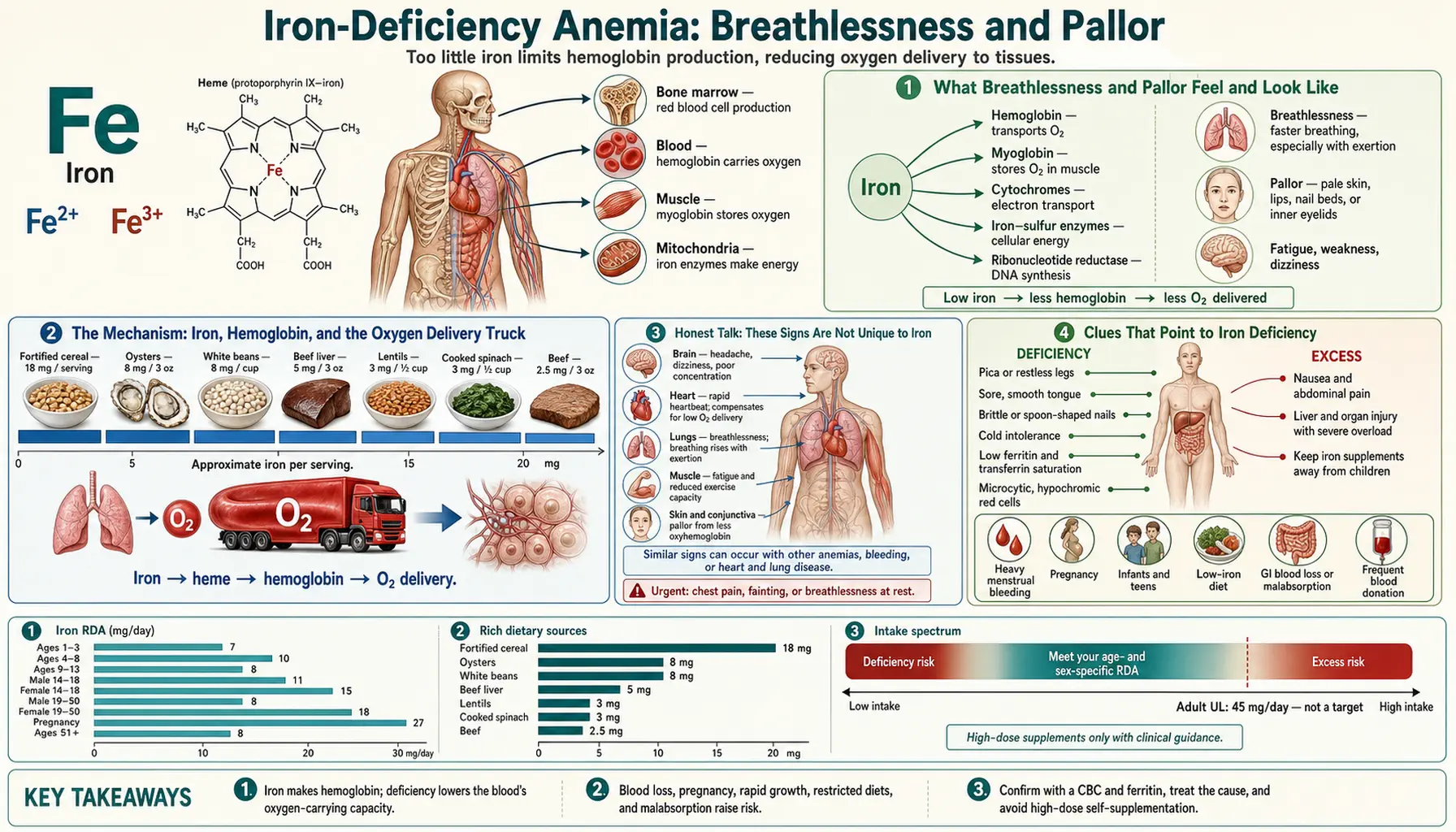
To understand why low iron causes these two signs, it helps to follow the oxygen. Every cell in the body burns oxygen to make energy, and oxygen has to be carried to them from the lungs. It does not dissolve well in blood on its own, so it hitches a ride on a protein inside red blood cells called hemoglobin. At the heart of every hemoglobin molecule sit four atoms of iron, and it is the iron that actually grips the oxygen in the lungs and releases it in the tissues. No iron, no hemoglobin; no hemoglobin, no way to move oxygen in any quantity.
When iron stores run down, the bone marrow keeps trying to make red blood cells but cannot fill them with enough hemoglobin. The result is fewer red cells, and the ones that are made are smaller and paler than normal — what a lab report calls microcytic (small) and hypochromic (low in colour). The blood's total capacity to carry oxygen falls. This is anemia: not a shortage of oxygen in the air, but a shortage of the trucks that move it.
An analogy. Picture the bloodstream as a fleet of delivery trucks running oxygen from the lungs (the warehouse) to every tissue in the body. Hemoglobin is the truck; iron is the loading hook that lets each truck pick up its cargo. In iron deficiency you have fewer trucks on the road, and the ones still running are half-empty. At rest, when the city's demand for deliveries is low, the reduced fleet just about copes and you may feel almost normal. But the moment demand spikes — you climb stairs, walk fast, or exercise, and your muscles suddenly want far more oxygen — the depleted fleet cannot keep up. The body's only options are to run the remaining trucks faster (a racing heart) and to demand more loads from the warehouse (faster, deeper breathing). That frantic compensation is exactly what you experience as a pounding heart and breathlessness on exertion.
Pallor comes from the very same shortage, seen from the outside. Skin and mucous membranes look pink because of the red blood flowing through their tiny vessels. With fewer, paler red cells, and with the body also diverting blood away from the skin toward the vital organs, the surface loses its colour. Breathlessness and pallor, in other words, are two faces of one underlying fact: not enough oxygen-carrying capacity in the blood.
This is also why iron deficiency without full-blown anemia can already cause symptoms. Iron is needed not only for hemoglobin but for the oxygen-using machinery inside muscle and brain cells, so work capacity and stamina can fall even before the hemoglobin count itself drops below normal — a point covered more in Iron Deficiency Anemia and on the fatigue and weakness page.
Honest Talk: These Signs Are Not Unique to Iron
It is important to be straight about this: breathlessness on exertion and pale skin are not proof of iron deficiency. Both are produced by the body's response to reduced oxygen delivery, and many conditions can do that. Treating either sign as a sure diagnosis — and self-prescribing iron on that basis — can be a real mistake, because some of the alternative causes are serious and a few are made worse by extra iron.
Other common causes of exertional breathlessness include:
- Anemia from a different cause. Iron deficiency is the most common, but anemia can also come from vitamin B12 or folate deficiency, from chronic kidney or inflammatory disease, from thyroid disease, or from inherited conditions such as thalassemia. See the broader anemia overview.
- Heart conditions — heart failure, coronary artery disease, and rhythm disturbances such as atrial fibrillation all cause breathlessness on effort and must not be missed.
- Lung conditions — asthma, chronic obstructive pulmonary disease (COPD), and other lung disease limit how much oxygen reaches the blood in the first place.
- Deconditioning, weight, anxiety, and simply being unfit — all real, all common, and all able to mimic the picture.
Pallor, similarly, has its own list of explanations beyond anemia: cold exposure (which is the body deliberately shutting down skin blood flow), low blood pressure or a faint, shock, and naturally fair skin that simply looks pale. There are also people who are constitutionally pale and perfectly healthy.
The honest bottom line is that these two signs are a strong reason to get checked, not a diagnosis in themselves. The good news is that the test that sorts it out is cheap, fast, and definitive (see Getting Tested).
Clues That Point to Iron Deficiency
While breathlessness and pallor alone do not seal the diagnosis, certain accompanying features make iron deficiency much more likely — especially when several appear together:
- A gradual onset. Iron-deficiency anemia usually creeps in over weeks or months as stores slowly deplete, so the body adapts and people often function with surprisingly low counts. Breathlessness that came on suddenly over hours or a day points away from simple iron deficiency and toward an urgent cause.
- The classic companion symptoms. Iron deficiency has a recognizable cluster: fatigue and weakness, restless legs and pica (a craving to chew ice or non-food items), hair shedding, brittle or spoon-shaped nails, a sore or smooth tongue, and cracks at the corners of the mouth. The more of these that travel together with the breathlessness and pallor, the stronger the case.
- A plausible source of iron loss or low intake. Heavy menstrual periods, pregnancy, a vegetarian or vegan diet, recent blood donation, known digestive disease, or being an older adult who might be losing small amounts of blood from the gut (see causes below) all raise the prior probability.
- Ice craving (pagophagia) deserves a special mention: a sudden, intense compulsion to crunch ice is so specific to iron deficiency that it is worth flagging to a clinician on its own.
None of these prove iron deficiency — only the blood test does — but a person who is pale, breathless on the stairs, perpetually tired, craving ice, and having heavy periods has, in effect, written the diagnosis on the wall. The clinician's job is then to confirm it and, crucially, to find out why.
What Drains Iron in the First Place
Iron-deficiency anemia is always a clue, never just a label, because the body guards iron jealously and loses very little of it normally. When iron runs short, one of three things is usually going on: too little is coming in, too little is being absorbed, or — most importantly — blood (and therefore iron) is being lost.
- Blood loss is the leading cause in adults, and the one that matters most to chase down. In women of reproductive age, heavy menstrual bleeding is the commonest culprit by far. In men and in women past menopause, unexplained iron deficiency is treated as possible gastrointestinal blood loss until proven otherwise — from an ulcer, inflammation, or sometimes a bowel cancer — which is why guidelines recommend investigating the gut in these groups even when symptoms are mild. Slow, hidden blood loss can lower iron without any visible bleeding at all.
- Increased demand — pregnancy roughly doubles iron requirements, and infants, young children, and adolescents in growth spurts also need a great deal. Endurance athletes lose iron through several routes and are commonly affected.
- Low intake or poor absorption. Diets very low in the readily absorbed heme iron found in meat rely on the less-absorbable non-heme iron in legumes and leafy greens, which raises the risk if intake is not managed. Absorption is impaired by conditions such as celiac disease, by infection with Helicobacter pylori, after some weight-loss surgery, and by long-term acid-suppressing medication (stomach acid helps free up dietary iron).
Because the consequences of missing a serious cause are real, the rule clinicians follow is firm: do not just refill the tank, find the leak. Replacing iron without investigating the reason it dropped can mask a treatable — occasionally dangerous — underlying problem.
Getting Tested
Confirming iron-deficiency anemia is one of the most reliable and inexpensive things in medicine, done with two simple blood tests:
- A Complete Blood Count (CBC) measures the hemoglobin level (which defines anemia) and the average size of the red cells (the MCV). In iron deficiency the hemoglobin is low and the cells are characteristically small (low MCV) and pale — the microcytic, hypochromic pattern. Anemia is generally defined as a hemoglobin below about 13 g/dL in men and below about 12 g/dL in non-pregnant women, though thresholds vary a little by source and by pregnancy.
- An Iron Panel, and above all the ferritin level, tells you whether the cause is genuinely low iron. Ferritin reflects the body's iron stores, and a low ferritin is the most specific single test for iron deficiency — it is the empty fuel gauge. (One caveat: ferritin also rises with inflammation, infection, and liver disease, so a normal or high ferritin does not always rule iron deficiency out; clinicians interpret it alongside other markers such as transferrin saturation.)
Together these answer two questions at once: is the person anemic, and is iron the reason. If both confirm iron-deficiency anemia, attention turns to the cause — which may mean asking in detail about periods and diet, testing for celiac disease, checking the stool for hidden blood, and, in adults where gut blood loss is a concern, arranging endoscopy of the upper and/or lower digestive tract. The investigation is matched to the person: a teenager with heavy periods and a vegetarian diet needs a very different workup from a 65-year-old man with no obvious source of loss.
Correcting Low Iron Safely
Treatment has two halves that go together: refill the iron and fix the cause. Doing only the first is a temporary patch if blood is still being lost.
- Food, as the foundation and for prevention. The most readily absorbed iron is heme iron from animal foods — red meat, poultry, and fish. Plant (non-heme) iron from lentils and beans, tofu, spinach and other greens, and fortified grains is absorbed less efficiently, but pairing it with a source of vitamin C (citrus, peppers, tomatoes) at the same meal markedly improves uptake, while tea, coffee, and calcium-rich foods taken with the meal reduce it. Diet alone, however, is usually too slow to correct an established anemia — it is the long game and the prevention, not the rescue.
- Oral iron supplements are the mainstay of treatment for most people: ferrous sulfate, ferrous gluconate, or ferrous fumarate. A practical point backed by recent research is that iron is absorbed better when doses are not crowded together — taking a single daily dose, or even alternate-day dosing, can absorb as well as or better than splitting it through the day, and tends to cause fewer side effects. Constipation, nausea, and dark stools are common with oral iron; taking it with vitamin C and adjusting the schedule helps tolerance. Replenishing stores after the hemoglobin recovers usually takes several months, so finishing the full course matters.
- Intravenous (IV) iron is used when oral iron is not tolerated or not absorbed (for example in inflammatory bowel disease), when losses outpace what tablets can replace, or when iron must be restored quickly — in advanced pregnancy, before surgery, or in certain heart and kidney conditions. It is given in a clinic and corrects stores faster than tablets.
- Treat the cause. Managing heavy periods, healing an ulcer, treating celiac disease or H. pylori, or removing a bleeding lesion is what makes the correction last.
An important caution that runs the other way: iron is not a harmless tonic to take “just in case.” The body has no efficient way to get rid of excess iron, and taking supplements without a confirmed deficiency can cause harm — particularly in people with the genetic iron-overload condition hemochromatosis. Iron tablets are also a leading cause of serious accidental poisoning in young children, so they must be stored well out of reach. Supplement on the basis of a blood test and a clinician's advice, not on a hunch.
How Fast the Breathlessness and Colour Come Back
One of the more encouraging things about iron-deficiency anemia is how reliably people improve once iron is replaced. The bone marrow responds to iron within days, ramping up the production of new red cells; on a blood test this shows as a rise in young red cells (reticulocytes) within about a week. The hemoglobin itself then climbs steadily, and most people see a meaningful rise of roughly 2 g/dL over three to four weeks of effective treatment, with the count returning to normal in about two months.
Symptoms usually track that recovery, and often run a little ahead of it. As oxygen-carrying capacity rebuilds, the breathlessness on stairs eases, the racing heart settles, energy returns, and the colour comes back to the lips, eyelids, and nail beds. It is worth keeping expectations realistic, though: the deeper the anemia and the longer it built up, the longer full recovery takes, and stores need to be topped up for months after the hemoglobin normalizes to prevent a relapse. If breathlessness and pallor do not improve as expected on treatment, that is itself a useful signal — it suggests either that iron is still being lost faster than it is replaced, that absorption is failing, or that something other than iron is contributing, and it warrants another look rather than simply more iron.
When to Seek Care / Red Flags
Most iron-deficiency anemia develops slowly and is sorted out calmly through a routine appointment and a blood test. But certain features mean seek medical help promptly — and some mean emergency care, not a routine visit:
- Breathlessness that comes on suddenly (over minutes to hours), breathlessness at rest, or that wakes you from sleep or forces you to sit up to breathe — call emergency services. This pattern points to a heart or lung emergency, not gradual anemia.
- Chest pain or pressure, particularly with the breathlessness, or breathlessness with fainting or near-fainting.
- A very fast or irregular heartbeat that does not settle with rest.
- Signs of active, significant bleeding — black, tarry, or bloody stools; vomiting blood or material like coffee grounds; or menstrual bleeding so heavy it soaks through protection hourly. These need urgent assessment.
- Severe pallor with rapid breathing, confusion, or collapse — signs the anemia may be profound or dropping fast.
- Any unexplained iron deficiency in a man or a postmenopausal woman — not an emergency, but it should always be investigated for a source of gut blood loss rather than simply treated with iron.
The guiding principle is the contrast between gradual and sudden: slowly progressive breathlessness with pallor over weeks fits iron deficiency and deserves an unhurried evaluation, whereas breathlessness that appears abruptly, occurs at rest, or comes with chest pain is treated as an emergency until proven otherwise. When in doubt, be seen — a single blood test, and where needed an ECG, quickly tells the difference.
Key Research Papers
- Camaschella C (2015). Iron-Deficiency Anemia. New England Journal of Medicine;372(19):1832-1843. — DOI: 10.1056/NEJMra1401038
- Lopez A, Cacoub P, Macdougall IC, Peyrin-Biroulet L (2016). Iron deficiency anaemia. The Lancet;387(10021):907-916. — DOI: 10.1016/S0140-6736(15)60865-0
- Pasricha SR, Tye-Din J, Muckenthaler MU, Swinkels DW (2021). Iron deficiency. The Lancet;397(10270):233-248. — DOI: 10.1016/S0140-6736(20)32594-0
- DeLoughery TG (2017). Iron Deficiency Anemia. Medical Clinics of North America;101(2):319-332. — DOI: 10.1016/j.mcna.2016.09.004
- Auerbach M, Adamson JW (2016). How we diagnose and treat iron deficiency anemia. American Journal of Hematology;91(1):31-38. — DOI: 10.1002/ajh.24201
- Camaschella C (2015). Iron deficiency: new insights into diagnosis and treatment. Hematology (ASH Education Program);2015(1):8-13. — DOI: 10.1182/asheducation-2015.1.8
- Camaschella C (2019). Iron deficiency. Blood;133(1):30-39. — DOI: 10.1182/blood-2018-05-815944
- Goddard AF, James MW, McIntyre AS, Scott BB (2011). Guidelines for the management of iron deficiency anaemia. Gut;60(10):1309-1316. — DOI: 10.1136/gut.2010.228874
- Stoffel NU, Cercamondi CI, Brittenham G, et al. (2017). Iron absorption from oral iron supplements given on consecutive versus alternate days. The Lancet Haematology;4(11):e524-e533. — DOI: 10.1016/S2352-3026(17)30182-5
- Haas JD, Brownlie T (2001). Iron Deficiency and Reduced Work Capacity: A Critical Review of the Research to Determine a Causal Relationship. The Journal of Nutrition;131(2):676S-690S. — DOI: 10.1093/jn/131.2.676S
- Lozoff B, Georgieff MK (2006). Iron Deficiency and Brain Development. Seminars in Pediatric Neurology;13(3):158-165. — DOI: 10.1016/j.spen.2006.08.004
- Short MW, Domagalski JE (2013). Iron deficiency anemia: evaluation and management. American Family Physician;87(2):98-104. — PubMed
PubMed Topic Searches
- PubMed — Iron-deficiency anemia and exertional dyspnea
- PubMed — Conjunctival pallor and the diagnosis of anemia
- PubMed — Oral iron and alternate-day dosing
- PubMed — Iron deficiency and gastrointestinal blood loss
- PubMed — Ferritin, iron deficiency, and inflammation
Connections
- Iron Deficiency Symptom Hub
- Iron Deficiency and Fatigue & Weakness
- Iron Deficiency and Hair Loss
- Iron Deficiency, Restless Legs & Pica
- Iron Overview
- Iron Benefits Deep Dive
- Iron and Iron-Deficiency Anemia
- Anemia
- Hemochromatosis (Iron Overload)
- Complete Blood Count
- Iron Panel
- Vitamin C (Iron Absorption)
- Vitamin B12
- Vitamin B9 (Folate)
- Heart Failure
- Beef
- Lentils
- Spinach