Hair Loss
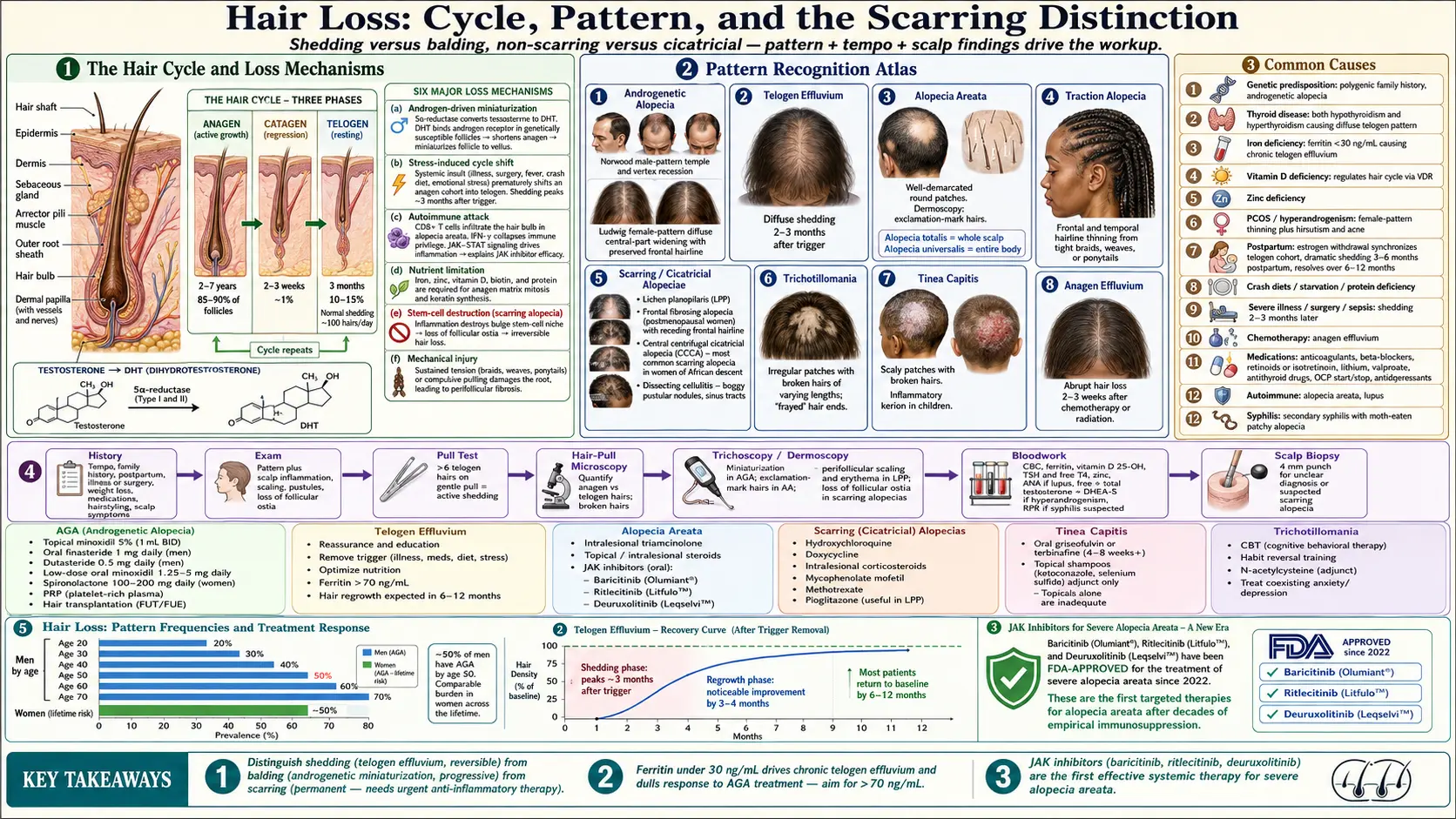
Table of Contents
- Overview
- Types
- Common Causes
- Mechanisms
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Hair loss (alopecia) is one of the most common dermatologic complaints, affecting roughly half of men by age 50 and a comparable proportion of women across a lifetime. Clinically it is essential to distinguish shedding from balding: shedding is loss of hair fibers that have completed their cycle, often diffuse and reversible; balding (miniaturization) is progressive thinning where individual follicles shrink and produce finer, shorter hairs. Equally important is the distinction between non-scarring alopecia, where the follicle is preserved and regrowth is possible, and scarring (cicatricial) alopecia, where the follicular stem cells are destroyed and loss is permanent.
Hair grows in cycles. At any moment about 85–90 percent of scalp follicles are in anagen (active growth, lasting 2–7 years), roughly 1 percent in catagen (a brief regression phase of 2–3 weeks), and 10–15 percent in telogen (resting, lasting about 3 months before the hair sheds). Losing about 100 hairs per day is normal. Disorders of hair loss reflect either a shift in this cycle (more follicles pushed into telogen), miniaturization of anagen hairs, autoimmune attack on the follicle, or destruction of the follicle itself.
Types
- Androgenetic alopecia (AGA) — the most common form. Male-pattern loss begins at the temples and vertex; female-pattern loss is typically a diffuse widening of the central part with preservation of the frontal hairline. Driven by androgen-mediated miniaturization in genetically susceptible follicles.
- Telogen effluvium — diffuse shedding 2–3 months after a trigger (severe illness, surgery, childbirth, crash diet, new medication, major stress). May be acute (resolves in 6–12 months) or chronic (persists beyond 6 months, often without an obvious single trigger).
- Alopecia areata — autoimmune T-cell attack on the hair bulb producing well-demarcated round patches of complete hair loss. Can progress to alopecia totalis (whole scalp) or alopecia universalis (entire body, including eyebrows and lashes).
- Traction alopecia — mechanical loss from tight hairstyles (braids, weaves, ponytails, extensions). Often begins at the frontal/temporal hairline. Reversible early; permanent if chronic.
- Scarring (cicatricial) alopeciae — destroy follicular stem cells and produce permanent loss. Includes lichen planopilaris, frontal fibrosing alopecia (a slowly receding frontal hairline most often in postmenopausal women), central centrifugal cicatricial alopecia (CCCA, most common in women of African descent), and dissecting cellulitis of the scalp.
- Trichotillomania — compulsive hair-pulling producing irregular patches with broken hairs of varying lengths.
- Tinea capitis — dermatophyte infection of the scalp, mostly in children. Produces scaly patches with broken-off hairs and sometimes an inflammatory kerion.
- Anagen effluvium — abrupt loss of actively growing hairs from chemotherapy or radiation, often within 2–3 weeks of exposure.
Common Causes
- Genetic predisposition — the dominant driver of androgenetic alopecia, with polygenic inheritance and a strong family history.
- Thyroid disease — both hypothyroidism and hyperthyroidism produce diffuse telogen-pattern shedding. See Thyroid Disorders.
- Iron deficiency — ferritin below 30 ng/mL is associated with chronic telogen effluvium and reduced response to AGA treatment. Iron is required for follicle anagen maintenance.
- Vitamin D deficiency — low vitamin D is associated with telogen effluvium and alopecia areata; the vitamin-D receptor regulates the hair cycle.
- Zinc deficiency — impairs anagen and is correctable with supplementation.
- PCOS / hyperandrogenism — polycystic ovary syndrome drives female-pattern thinning along with hirsutism and acne.
- Postpartum telogen effluvium — estrogen withdrawal after delivery shifts a synchronized cohort of follicles into telogen, producing dramatic shedding 3–6 months postpartum that resolves over the next 6–12 months.
- Crash diets and starvation — rapid weight loss, very low-calorie diets, and protein deficiency precipitate telogen effluvium.
- Severe illness or surgery — high fevers, sepsis, hospitalization, and major operations are classic triggers, with shedding appearing 2–3 months later.
- Chemotherapy — cytotoxic agents abruptly halt anagen (anagen effluvium), with regrowth usually beginning within months of treatment ending.
- Medications — anticoagulants (heparin, warfarin), beta-blockers, retinoids and isotretinoin, lithium, valproate, antithyroid drugs, oral contraceptives (start or stop), and some antidepressants are well-documented triggers.
- Autoimmune disease — alopecia areata; lupus can produce both non-scarring telogen-pattern loss and scarring discoid lesions.
- Syphilis — secondary syphilis can produce a characteristic moth-eaten patchy alopecia.
- Scarring inflammatory diseases — lichen planopilaris, frontal fibrosing alopecia, CCCA, and dissecting cellulitis destroy follicles permanently and require early anti-inflammatory treatment.
Mechanisms
Hair loss arises through several distinct pathways, often in combination:
- Androgen-driven miniaturization — in androgenetic alopecia, the enzyme 5-alpha-reductase converts testosterone to dihydrotestosterone (DHT) in scalp follicles. DHT binds androgen receptors in genetically susceptible follicles, progressively shortening anagen and miniaturizing the follicle until it produces only fine vellus hair.
- Stress-induced cycle shift — in telogen effluvium, a systemic insult (illness, surgery, childbirth, severe diet) prematurely shifts a large cohort of anagen hairs into telogen. Because telogen lasts about 3 months, shedding peaks roughly 3 months after the trigger.
- Autoimmune attack — in alopecia areata, autoreactive CD8+ T cells infiltrate the hair bulb and produce interferon-gamma, collapsing the immune privilege of the anagen follicle. JAK-STAT signaling drives this inflammation, which is why JAK inhibitors are effective.
- Nutrient limitation — iron, zinc, vitamin D, biotin, and protein are required for the high mitotic rate of anagen matrix cells. Deficiency reduces anagen synthesis and prolongs telogen, manifesting as diffuse shedding and reduced hair quality.
- Stem-cell destruction — in scarring alopeciae, lymphocytic or neutrophilic inflammation destroys the follicular bulge stem-cell niche. Once gone, the follicle cannot regenerate and the loss is permanent.
- Mechanical injury — sustained tension from hairstyles or compulsive pulling damages the follicle root and, if chronic, leads to perifollicular fibrosis and permanent loss.
Evaluation
Workup is guided by pattern (diffuse vs. patterned vs. patchy vs. scarring) and tempo (acute shedding vs. slow miniaturization).
- History — tempo and timing, family history, postpartum status, recent illness or surgery, weight loss or dieting, new or stopped medications, hairstyling practices, scalp symptoms (itch, pain, burning).
- Examination — identify the pattern (frontal/vertex thinning, diffuse, patchy, scarring), look for scalp inflammation, scaling, pustules, or loss of follicular ostia (suggests scarring).
- Pull test — gentle traction on a small bundle of hairs; more than 6 telogen hairs extracted suggests active shedding.
- Hair-pull microscopy — look for telogen club hairs vs. anagen hairs vs. broken shafts vs. dystrophic forms.
- Trichoscopy / dermoscopy — identifies miniaturization (varying shaft diameters in AGA), exclamation-mark hairs (alopecia areata), perifollicular scaling and erythema (lichen planopilaris), and loss of follicular ostia (scarring).
- Bloodwork — CBC, ferritin, vitamin D 25-OH, TSH and free T4, zinc; ANA if lupus is suspected; free testosterone, total testosterone, and DHEA-S in suspected hyperandrogenism; RPR or treponemal antibody for suspected syphilis.
- Scalp biopsy — 4 mm punch (often two specimens, one for horizontal and one for vertical sectioning) when the pattern is unclear, scarring is suspected, or the diagnosis remains uncertain after non-invasive workup.
Management
- Androgenetic alopecia — topical minoxidil (5% solution or foam in men, 2% or 5% in women), oral finasteride 1 mg/day (men), oral dutasteride 0.5 mg/day, low-dose oral minoxidil (typically 1.25–5 mg/day, off-label), spironolactone 100–200 mg/day in women, platelet-rich plasma (PRP) injections, low-level laser therapy, and surgical hair transplantation (FUE or FUT) for stable patients with adequate donor density.
- Telogen effluvium — reassurance is the cornerstone; identify and remove the trigger (taper offending medications, repleat ferritin to >70 ng/mL, correct vitamin D and zinc, restore adequate calorie and protein intake). Acute cases resolve over 6–12 months. Chronic telogen effluvium may benefit from low-dose oral minoxidil.
- Alopecia areata — intralesional triamcinolone (5–10 mg/mL) for limited patches, topical or short-course oral corticosteroids, JAK inhibitors (baricitinib, ritlecitinib, and deuruxolitinib are FDA-approved for severe disease), topical minoxidil as adjunct, and contact immunotherapy (squaric acid, diphenylcyclopropenone) for resistant disease.
- Scarring alopecia — aggressive early anti-inflammatory therapy: hydroxychloroquine, doxycycline, intralesional and topical corticosteroids, mycophenolate, methotrexate, and pioglitazone (in lichen planopilaris). The goal is to halt progression; lost follicles cannot be restored.
- Postpartum telogen effluvium — reassurance and time. Most women regrow normally within 6–12 months. Address ferritin, thyroid status, and protein intake.
- Traction alopecia — remove the offending hairstyle; topical minoxidil can support regrowth in early disease. Late traction alopecia is scarring and irreversible.
- Tinea capitis — oral antifungal (griseofulvin or terbinafine); topical antifungals alone are inadequate.
- Trichotillomania — cognitive-behavioral therapy with habit-reversal training is first-line; N-acetylcysteine and SSRIs are adjuncts.
- Nutrition — address ferritin (target >70 ng/mL), vitamin D, zinc, vitamin B12, and adequate protein in any patient with shedding.
- Cosmetic strategies — volumizing products, scalp camouflage powders and fibers, microblading for eyebrows, scalp micropigmentation, and well-fitted wigs or hair systems. These are legitimate and can substantially improve quality of life.
When to Seek Medical Care
- Sudden patchy hair loss, especially with well-defined round patches.
- Scarring, scaling, redness, pustules, or loss of follicular openings on the scalp.
- Scalp pain, burning, or persistent itch accompanying hair loss.
- Painful pustules or boggy nodules (suspect dissecting cellulitis or kerion).
- Hair loss accompanied by systemic symptoms — rash, joint pain, fatigue, fever, weight change, or menstrual irregularity.
- Rapidly progressive shedding or visible thinning over weeks rather than months.
- Hair loss in a child, especially with scaling or broken hairs.
- A receding frontal hairline in a postmenopausal woman (consider frontal fibrosing alopecia).
Connections
- Zinc
- Vitamin B12
- Thyroid Disorders
- Lupus
- Polycystic Ovary Syndrome
- Hashimoto's Thyroiditis
- Vitamin D3
- Alopecia
- Iron
- Diabetes
- Anemia
- Testosterone
- Fatigue
- Inflammatory Markers
- Selenium
- Rosemary
- Saw Palmetto
- Iron Panel
References & Research
Historical Background
Modern hair-loss therapeutics begin in 1979 with the incidental observation that minoxidil, an oral vasodilator developed for severe hypertension, produced unwanted hair growth in patients — a side effect the dermatology community quickly repurposed into a topical treatment, FDA-approved for AGA in 1988. Finasteride, a selective 5-alpha-reductase type II inhibitor, was approved for male androgenetic alopecia in 1997 after benign prostatic hyperplasia trials revealed the same hair-growth signal. The most consequential recent shift came in 2022, when the FDA approved baricitinib, an oral JAK1/2 inhibitor, as the first systemic therapy for severe alopecia areata — followed by ritlecitinib in 2023 and deuruxolitinib in 2024 — finally giving clinicians effective targeted treatment for an autoimmune disease that had resisted decades of empirical immunosuppression.
Key Research Papers
- Olsen EA, Messenger AG, Shapiro J, et al. Evaluation and treatment of male and female pattern hair loss. Journal of the American Academy of Dermatology. 2005;52(2):301-311.
- King B, Ohyama M, Kwon O, et al. Two phase 3 trials of baricitinib for alopecia areata. New England Journal of Medicine. 2022;386(18):1687-1699.
- King B, Zhang X, Harcha WG, et al. Efficacy and safety of ritlecitinib in adults and adolescents with alopecia areata: a randomised, double-blind, multicentre, phase 2b-3 trial. The Lancet. 2023;401(10387):1518-1529.
- Phillips TG, Slomiany WP, Allison R. Hair loss: common causes and treatment. American Family Physician. 2017;96(6):371-378.
- Trueb RM. Diffuse hair loss. In: Hair Growth and Disorders. 2008. Review of telogen effluvium pathophysiology and management.
- Mirmirani P, Willey A, Headington JT, Stenn K, McCalmont TH, Price VH. Primary cicatricial alopecia: histopathologic findings do not distinguish clinical variants. Journal of the American Academy of Dermatology. 2005;52(4):637-643.
- Strazzulla LC, Wang EHC, Avila L, et al. Alopecia areata: disease characteristics, clinical evaluation, and new perspectives on pathogenesis. Journal of the American Academy of Dermatology. 2018;78(1):1-12.
- Patel P, Nessel TA, Kumar DD. Minoxidil. StatPearls / Journal of the American Academy of Dermatology review of low-dose oral minoxidil. 2021.
- Kanti V, Messenger A, Dobos G, et al. Evidence-based (S3) guideline for the treatment of androgenetic alopecia in women and men. British Journal of Dermatology. 2018;32(1):11-22.
- Suchonwanit P, Thammarucha S, Leerunyakul K. Minoxidil and its use in hair disorders: a review. Drug Design, Development and Therapy. 2019;13:2777-2786.
PubMed Topic Searches
- Androgenetic alopecia treatment
- Telogen effluvium
- Alopecia areata and JAK inhibitors
- Frontal fibrosing alopecia
- Ferritin and hair loss
- Low-dose oral minoxidil