Aura and Visual Disturbances in Migraine
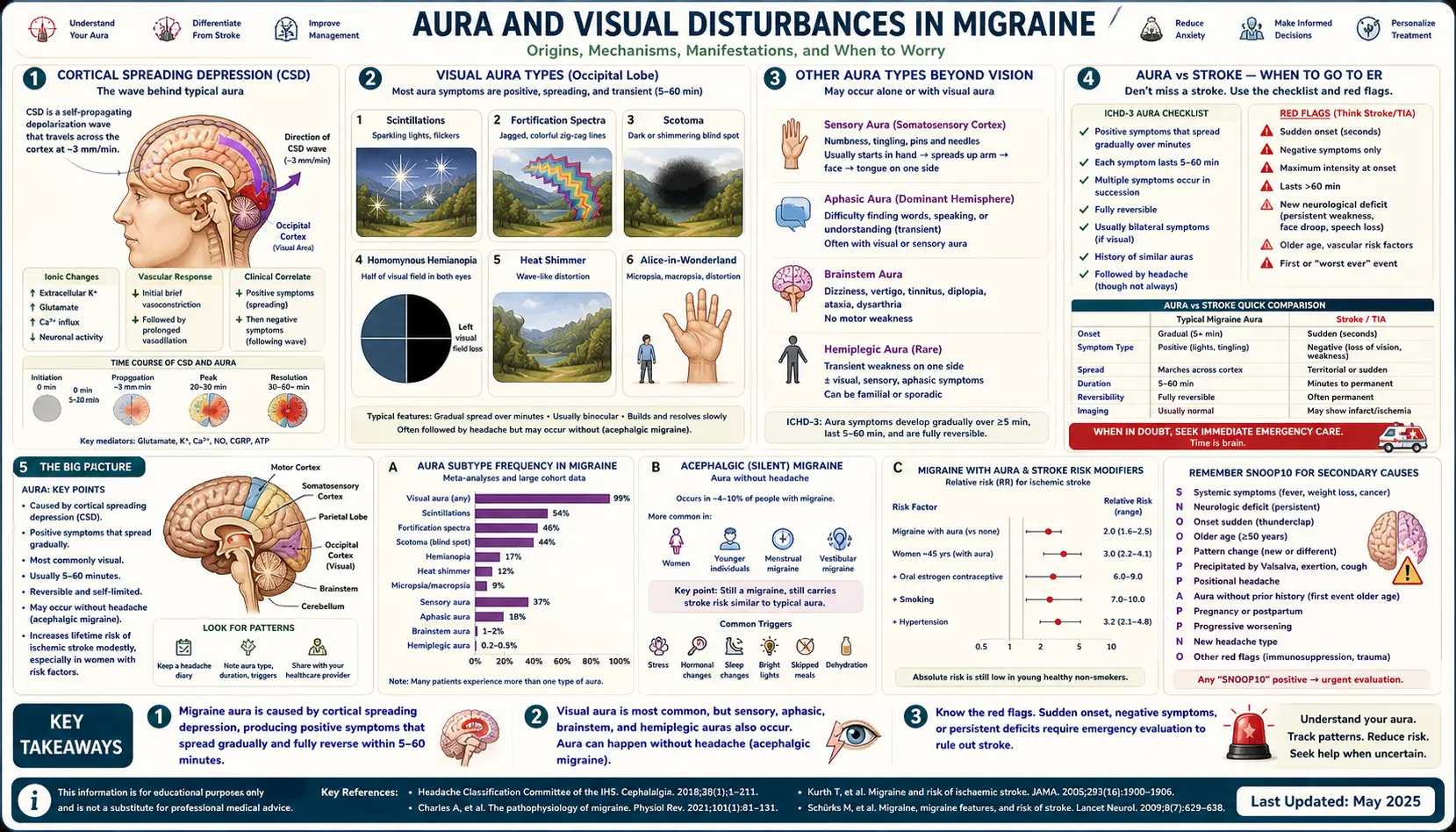
Table of Contents
- What Aura Actually Is
- Cortical Spreading Depression — The Wave Under the Symptoms
- Positive Versus Negative Symptoms
- Visual Aura Types
- Sensory Aura — The March Up the Arm
- Aphasic Aura — When Words Disappear
- Brainstem Aura
- Hemiplegic and Familial Hemiplegic Migraine
- Retinal Migraine — One-Eyed Aura
- Aura Without Headache
- Mimics and When to Go to the ER
- ICHD-3 Diagnostic Criteria
- Imaging — When You Actually Need an MRI
- Aura and Stroke Risk
- Treating an Attack That Starts With Aura
- Lasmiditan and Gepants — When Triptans Are Off the Table
- Key Research Papers
- Connections
- Featured Videos
What Aura Actually Is
About one-third of people with migraine experience aura. The word itself comes from the Greek for "breeze" — the sense that something is coming. Aura is a set of focal neurological symptoms that develop gradually over 5 to 20 minutes and last less than 60 minutes, usually preceding (but sometimes accompanying or following) the headache phase.
Aura is not "just seeing spots." It is your cerebral cortex transiently misfiring in a specific, mappable pattern. The symptoms depend on which patch of cortex is involved: visual (occipital lobe), sensory (parietal lobe), speech (language cortex in the dominant hemisphere), and motor or brainstem in rarer forms. Once you understand the underlying mechanism, every one of these experiences becomes predictable rather than frightening.
Aura matters clinically for three reasons. First, it is a diagnostic feature — "migraine with aura" is its own ICHD-3 category, not just a variation. Second, it changes treatment: some migraine subtypes (hemiplegic, brainstem) have historically been considered contraindications to triptans and ergotamines. Third, aura doubles the long-term risk of ischemic stroke, especially in women who smoke or use combined oral contraceptives — a number you deserve to have in hand when making birth-control and lifestyle decisions.
Cortical Spreading Depression — The Wave Under the Symptoms
The neurological event under every form of aura is cortical spreading depression (CSD), first described by Brazilian physiologist Araístides Leão in 1944. CSD is a slow-moving wave of intense neuronal and glial depolarization that crosses the cortex at roughly 3 millimeters per minute. Behind the wave, cells go silent for minutes to tens of minutes as they work to re-establish their ionic gradients.
The chemistry is dramatic. Potassium pours out of cells, glutamate floods the extracellular space, calcium rushes in, blood flow transiently increases then drops, and the blood-brain barrier becomes temporarily leaky. The result, for the person living inside that cortex, is a moving band of over-excited tissue (positive symptoms: flashing lights, tingling) followed by a moving band of silenced tissue (negative symptoms: blind spots, numbness, weakness).
In 2001, Hadjikhani and colleagues at Massachusetts General Hospital used functional MRI to watch this wave in real time in migraineurs. They saw exactly what Leão had predicted from animal experiments half a century earlier: a slow-moving front of cortical activation sweeping across the visual cortex at 3–5 mm per minute, matching the patient's progression of visual symptoms. That study settled the argument — aura is CSD in humans, not a vascular spasm as older textbooks claimed.
CSD also explains why aura marches. A wave crossing the visual cortex moves through retinotopic coordinates, so what you see shifts gradually across your visual field. A wave crossing sensory cortex moves across somatotopic coordinates, so tingling marches from fingertip to hand to forearm to face. The hand and face sit close together on the sensory homunculus, which is why sensory aura famously "jumps" from the arm to the lips.
Positive Versus Negative Symptoms
Every aura has two phases, though you may notice only one:
- Positive symptoms are additions — things that are there when they should not be. Flashing lights, zig-zag lines, sparkles, tingling, pins and needles, musical tones, the sense of a smell that nobody else can smell. These come from the depolarized, over-firing front edge of the CSD wave.
- Negative symptoms are subtractions — things that should be there and are not. Blind spots, numbness, weakness, loss of speech. These come from the silenced cortex behind the wave.
A textbook migraine aura goes positive-then-negative: zig-zags first, blind spot second. A textbook stroke, by contrast, tends to be negative from the start — a sudden blind field, sudden numbness, sudden weakness, with no preceding flicker or tingle. This distinction is one of the single most useful at-home rules of thumb for deciding whether a new visual or sensory event belongs in the ER.
Visual Aura Types
Visual aura is the most common form, occurring in roughly 90% of auras. Several stereotyped patterns show up:
- Scintillations. Tiny flashing dots, sparkles, or "TV snow" — small points of light that flicker in the visual field.
- Fortification spectra (teichopsia). The classic migraine zig-zag: a slowly expanding arc of shimmering, angular, sometimes rainbow-colored lines that resembles the aerial plan of a medieval fortress. The arc grows outward from a small starting point over 15–20 minutes. In the center of the arc is usually a blind spot.
- Scotoma. A blind spot, often crescent- or C-shaped, that enlarges and drifts across the visual field. A scotoma can be absolute (total black) or relative (greyed-out, scintillating).
- Tunnel vision or hemianopia. Loss of vision on one side of each eye — a curtain pulling across the left or right half of the world. This is a homonymous hemianopia, reflecting occipital cortex involvement on the opposite side.
- Heat-shimmer or water-ripple distortion. The world looks like it is seen through a heat haze rising off summer pavement.
- Alice-in-Wonderland phenomena. Rarer: objects appear too large, too small, too near, or too far. More common in children.
Visual auras affect both eyes even though they may feel like they are only in one. If you cover one eye and the symptom is still there, the source is cortical. If the symptom disappears when you cover one eye, the source is in that eye itself — and that is a different beast (see retinal migraine).
Sensory Aura — The March Up the Arm
About 30–40% of auras involve sensation. The classical pattern is a cheiro-oral march: tingling (pins and needles) starts in the fingertips, climbs over 10–20 minutes up the hand, forearm, upper arm, shoulder — and then, astonishingly, jumps to the lips and tongue on the same side, skipping the trunk entirely.
That jump is not magic; it reflects the layout of the sensory cortex. The homunculus puts the hand and the face right next to each other, with the trunk's representation tucked away elsewhere. A CSD wave crossing sensory cortex passes through those adjacent regions in sequence, so the symptoms march through the body parts they represent. The speed (3 mm/minute, taking 20–30 minutes to cross from hand to mouth) is the diagnostic signature.
A stroke or TIA, by contrast, causes numbness that is maximal from the instant it begins. Sudden face-plus-arm numbness with no march, no preceding tingle, and no headache history is a stroke until proven otherwise. Call 911.
Aphasic Aura — When Words Disappear
Roughly 20% of auras involve speech or language. You may know exactly what you want to say and find that the words will not come out, or come out jumbled. You may lose the ability to understand what others are saying. You may read a sign and see only meaningless shapes. These symptoms reflect CSD crossing Broca's or Wernicke's area in the dominant (usually left) hemisphere.
Aphasic aura is terrifying the first time it happens, and it is the single symptom that most often sends migraineurs to the emergency room. The reassuring feature is that it resolves within an hour and is typically followed by the migraine headache you already know. The concerning feature is that isolated language loss with no history of migraine aura is identical to a small stroke in the language cortex — which is why a first-ever episode of aphasia at any age warrants urgent evaluation, even if the rest of the picture looks migrainous.
Brainstem Aura
Previously called "basilar-type migraine," migraine with brainstem aura involves at least two of the following fully reversible brainstem symptoms, alongside typical visual, sensory, or aphasic aura:
- Vertigo — the room spinning, not just lightheadedness.
- Dysarthria — slurred speech, distinct from aphasia (you know the words; your mouth will not shape them).
- Diplopia — double vision in both eyes.
- Ataxia — loss of coordination, staggering gait, inability to do finger-to-nose smoothly.
- Tinnitus or decreased hearing.
- Decreased level of consciousness — drowsiness or near-syncope.
Brainstem aura is uncommon, runs in families, and looks alarming because these are the same symptoms caused by strokes in the posterior circulation. Diagnosis requires a neurologist and, on a first episode, imaging to exclude a posterior stroke or structural lesion. Once established, brainstem aura is generally benign in terms of tissue damage — but it has historically been a contraindication to triptans and ergotamines because those drugs constrict vessels and theoretically worsen brainstem ischemia.
There is overlap with vestibular migraine, in which vertigo is the dominant feature. The distinction matters for treatment.
Hemiplegic and Familial Hemiplegic Migraine
Hemiplegic migraine is aura that includes actual motor weakness on one side of the body — not just numbness, but a weak or paralyzed arm, leg, or face. Weakness develops gradually over minutes to an hour (not instantly like a stroke), lasts minutes to hours or rarely days, and then resolves fully. The headache that follows is usually severe.
When it runs in families with at least one other affected first- or second-degree relative, it is called familial hemiplegic migraine (FHM). Three specific genes have been identified:
- CACNA1A (FHM type 1) — codes a voltage-gated calcium channel subunit. Also implicated in episodic ataxia and spinocerebellar ataxia.
- ATP1A2 (FHM type 2) — codes a sodium-potassium ATPase pump subunit. Without proper pump function, neurons cannot clear the potassium they release, which is exactly the setup for runaway CSD.
- SCN1A (FHM type 3) — codes a voltage-gated sodium channel subunit. Also implicated in certain epilepsies.
Notice the theme: every known FHM gene regulates the ion balance that determines how easily CSD can start and spread. These families essentially have a lowered threshold for the cortical spreading wave.
Non-familial ("sporadic") hemiplegic migraine looks clinically identical but without an affected relative and without a consistent known mutation. Management overlaps.
A first episode of unilateral weakness is always a stroke workup, full stop. Even patients with long-established hemiplegic migraine are advised to seek urgent evaluation if an attack is noticeably different from their usual pattern, lasts longer than usual, or fails to resolve completely.
Retinal Migraine — One-Eyed Aura
Retinal migraine is rare and easily confused with visual aura but arises in the eye itself, not the cortex. The tell is that the symptom is monocular — present in one eye and gone when that eye is closed. Visual aura from the cortex is always binocular, even when it looks like it is only on one side.
Symptoms include a curtain of blindness descending over one eye, scintillations confined to one eye, or a gray-out in one eye lasting minutes. The headache may follow on the same side.
Any first episode of monocular vision loss requires urgent ophthalmology and neurology evaluation because the differential includes amaurosis fugax (transient retinal ischemia from a carotid plaque), retinal vein or artery occlusion, optic neuritis, and giant cell arteritis (in patients over 50). These are not conditions to wait out.
Aura Without Headache
In a subset of migraineurs, aura happens without any headache afterward. This is called acephalgic migraine or migraine aura without headache. It is especially common in older adults, many of whom had migraine with aura in their twenties, stopped having headaches in their fifties or sixties, and now get just the zig-zags and blind spots every few months.
First-ever aura symptoms appearing after age 40 — even in someone with a long history of migraine without aura — deserve an imaging workup. The differential at that age widens to include transient ischemic attack, occipital lobe tumor, arteriovenous malformation, and occipital seizures. Most cases turn out to be benign late-onset aura, but the workup is worth doing once.
Mimics and When to Go to the ER
These are the clinical features that should send anyone to the emergency room regardless of migraine history:
- Sudden onset. Aura builds over 5–20 minutes. Stroke is instant. If symptoms hit full intensity in seconds, go now.
- Purely negative symptoms from the start. Immediate blind spot, numbness, or weakness with no preceding flicker or tingle looks more like a stroke than aura.
- No march. Aura moves across a body part or visual field. Stroke lights up a territory all at once.
- Duration over 60 minutes. By ICHD-3, each aura symptom lasts 5–60 minutes. Prolonged aura — especially weakness or speech loss persisting past an hour — is a red flag and can indicate a "migrainous infarction" or a mislabeled stroke.
- First-ever episode, any age. A first-ever aura-like event has never been through diagnosis. Treat it as a stroke or seizure until a professional rules those out.
- New pattern in a known migraineur. If your aura is suddenly on the opposite side, or includes new motor weakness, or lasts far longer than your usual attacks, do not assume it is "just migraine."
- Occipital seizure. Seizures arising in the occipital lobe can produce colorful visual hallucinations eerily similar to aura, but they tend to be briefer (seconds to a couple of minutes), more stereotyped, and may be followed by loss of awareness. EEG is the distinguishing test.
- Thunderclap headache. Aura followed by the worst headache of your life, instantly peaking, is subarachnoid hemorrhage until proven otherwise. Call 911.
The simple patient rule: migraine aura builds and marches; stroke hits and stays. Apply that rule, err on the side of caution, and never drive yourself — call 911 or have someone drive you.
ICHD-3 Diagnostic Criteria
The International Classification of Headache Disorders, third edition (ICHD-3), is the standard for migraine diagnosis worldwide. For migraine with aura (1.2), the criteria are:
- At least two attacks fulfilling criteria B and C.
- One or more of the following fully reversible aura symptoms: visual, sensory, speech or language, motor, brainstem, or retinal.
- At least three of six characteristics:
- At least one aura symptom spreads gradually over 5 minutes or more.
- Two or more aura symptoms occur in succession.
- Each individual aura symptom lasts 5–60 minutes.
- At least one aura symptom is unilateral.
- At least one aura symptom is positive.
- Aura is accompanied, or followed within 60 minutes, by headache.
- Not better accounted for by another diagnosis, and TIA excluded.
Hemiplegic migraine, brainstem aura, and retinal migraine each have their own ICHD-3 subcodes (1.2.3, 1.2.2, 1.2.4) with additional requirements.
Imaging — When You Actually Need an MRI
Most migraineurs do not need imaging. Routine brain MRI in a young adult with a long history of typical migraine with aura is low-yield and frequently normal. Imaging is warranted when any of the following apply:
- First-ever episode of migraine-like aura.
- New or changing pattern in a known migraineur — new side, new symptom type, longer duration.
- Focal neurological deficit that persists between attacks.
- First episode after age 40, even in someone with pre-existing migraine without aura.
- Hemiplegic, brainstem, or retinal features on first evaluation.
- Thunderclap onset, fever, papilledema, seizures, or altered mental status.
- History of cancer, immunosuppression, or anticoagulation.
MRI with and without contrast is generally preferred over CT because it picks up posterior-fossa and small vessel disease that CT misses. MR angiography or venography is added if a vascular cause (dissection, cerebral venous sinus thrombosis) is suspected.
Aura and Stroke Risk
This is the least comfortable fact in the migraine literature. Migraine with aura is an independent risk factor for ischemic stroke. The relative risk is roughly doubled compared with people who do not have migraine, with the increase concentrated in certain subgroups.
The absolute risks are modest, which is important context. In a healthy 30-year-old woman with migraine with aura, the annual stroke risk is still small — on the order of 1 in 10,000 to 1 in 5,000 per year. That number climbs when combined with other factors:
- Smoking — multiplies stroke risk about threefold on top of aura.
- Combined oral contraceptives (estrogen-containing) — multiplies stroke risk by 2–4× on top of aura.
- Aura plus smoking plus combined oral contraceptives — the combined relative risk approaches 7–10× the baseline. Most guidelines (including the World Health Organization and the American College of Obstetricians and Gynecologists) treat migraine with aura as a contraindication to estrogen-containing contraception.
Practical implications for women with migraine with aura:
- Avoid combined oral contraceptives. Progestin-only options (mini-pill, IUD, implant) do not carry the same risk.
- Stop smoking. This is the single highest-leverage modifiable risk factor.
- Control blood pressure, cholesterol, and diabetes as you would for any cardiovascular risk reduction.
- Discuss the balance with a gynecologist who understands the headache medicine side — most do not, and you may have to advocate for yourself.
Men with aura have elevated stroke risk too, though the absolute numbers are smaller and the estrogen piece is absent.
Treating an Attack That Starts With Aura
For decades, triptans were considered contraindicated during aura itself because of a theoretical concern that vasoconstriction could worsen ischemia during the reduced-blood-flow phase of CSD. Labels in the United States still reflect this caution. In practice, that concern has not been borne out by the clinical data that accumulated over the twenty-plus years since triptans came to market.
Current thinking in headache medicine is more nuanced:
- Typical migraine with visual or sensory aura: most headache specialists consider triptans safe to take during aura, though the label says to wait. Taking a triptan as soon as headache begins (not during aura) remains the conservative approach and is still more effective for most people because triptans work best early in the headache phase.
- Hemiplegic and brainstem aura: triptans and ergotamines remain formally contraindicated in the United States labeling. The theoretical concern is vasoconstriction worsening posterior-circulation or motor-cortex ischemia. Some specialists use triptans in these patients off-label when the benefit outweighs the risk; many do not. This is a decision that belongs with a headache neurologist, not self-titration.
- Any aura plus cardiovascular disease: triptans are contraindicated because they constrict coronary arteries as well as cerebral vessels. Age, hypertension, diabetes, smoking, and high cholesterol all raise this concern.
For many aura patients, the easier path is to sidestep the vasoconstriction debate entirely with newer drug classes that do not constrict blood vessels at all.
Lasmiditan and Gepants — When Triptans Are Off the Table
Two newer drug classes have changed the calculus for aura-contraindicated patients:
- Lasmiditan (Reyvow) is a selective 5-HT1F receptor agonist. Unlike triptans, which hit 5-HT1B receptors on blood vessels and cause vasoconstriction, lasmiditan binds only the 5-HT1F subtype, which is expressed on trigeminal neurons but not on vessels. No vasoconstriction. It is approved for acute migraine and is appropriate for patients with hemiplegic migraine, brainstem aura, or known cardiovascular disease. The main drawback is that it is sedating and impairs driving for at least 8 hours after a dose.
- Gepants — ubrogepant (Ubrelvy), rimegepant (Nurtec ODT), and zavegepant (Zavzpret nasal spray) — block the CGRP receptor rather than constricting vessels. They are effective for acute migraine across the aura spectrum including hemiplegic and brainstem forms. Rimegepant uniquely doubles as both acute and preventive treatment. Gepants are well-tolerated, non-vasoactive, and do not carry the medication-overuse-headache risk of triptans taken too frequently (see the chronic migraine article).
The practical hierarchy for an aura-contraindicated patient looks something like: start with a gepant for acute treatment, reserve lasmiditan for attacks not controlled by a gepant (accepting the sedation), and use NSAIDs or antiemetics as supportive care. See the triptans and gepants article for dosing details and the CGRP inhibitors article for preventive options if your attacks are frequent.
Key Research Papers
- Hadjikhani N, et al. Mechanisms of migraine aura revealed by functional MRI in human visual cortex. Proc Natl Acad Sci USA. 2001. — The fMRI study that confirmed cortical spreading depression as the substrate of migraine aura in humans.
- Charles A. The migraine aura. Curr Pain Headache Rep. 2018. — Current clinical and mechanistic review by one of the field's leading authorities.
- Kurth T, et al. Migraine and risk of cardiovascular disease in women: prospective cohort study. JAMA (Women's Health Study analyses on migraine with aura and stroke risk). 2020. — Large prospective data quantifying aura-associated stroke and cardiovascular risk, especially in women.
- Ashina M. Migraine. N Engl J Med. 2020. — Comprehensive NEJM review covering pathophysiology, aura, and modern acute and preventive therapeutics.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on aura biology, diagnosis, and management:
- Migraine aura and cortical spreading depression
- Migraine with aura and ischemic stroke risk
- Familial hemiplegic migraine genetics
- Brainstem (basilar-type) aura
- Retinal migraine and monocular visual loss
- Acephalgic migraine in older adults
- Lasmiditan and gepants in aura-contraindicated patients
- Triptan safety during migraine aura
- ICHD-3 diagnostic criteria for migraine with aura
Connections
- Vestibular Migraine
- Chronic Migraine and Medication Overuse
- CGRP Inhibitors and Preventives
- Triptans and Gepants — Acute Treatment
- Migraine Overview
- Magnesium, Riboflavin, and Supplements
- Menstrual Migraine and Hormonal Triggers
- Diet Triggers and Elimination Protocol
- Mast Cell Activation Syndrome
- POTS
- Vertigo and Meniere's Disease
- Chronic Pain
- Chronic Fatigue Syndrome
- Fibromyalgia
- Stroke
- Headache
- Magnesium
- Migraine in Pregnancy and Breastfeeding