Diet Triggers and the Migraine Elimination Protocol
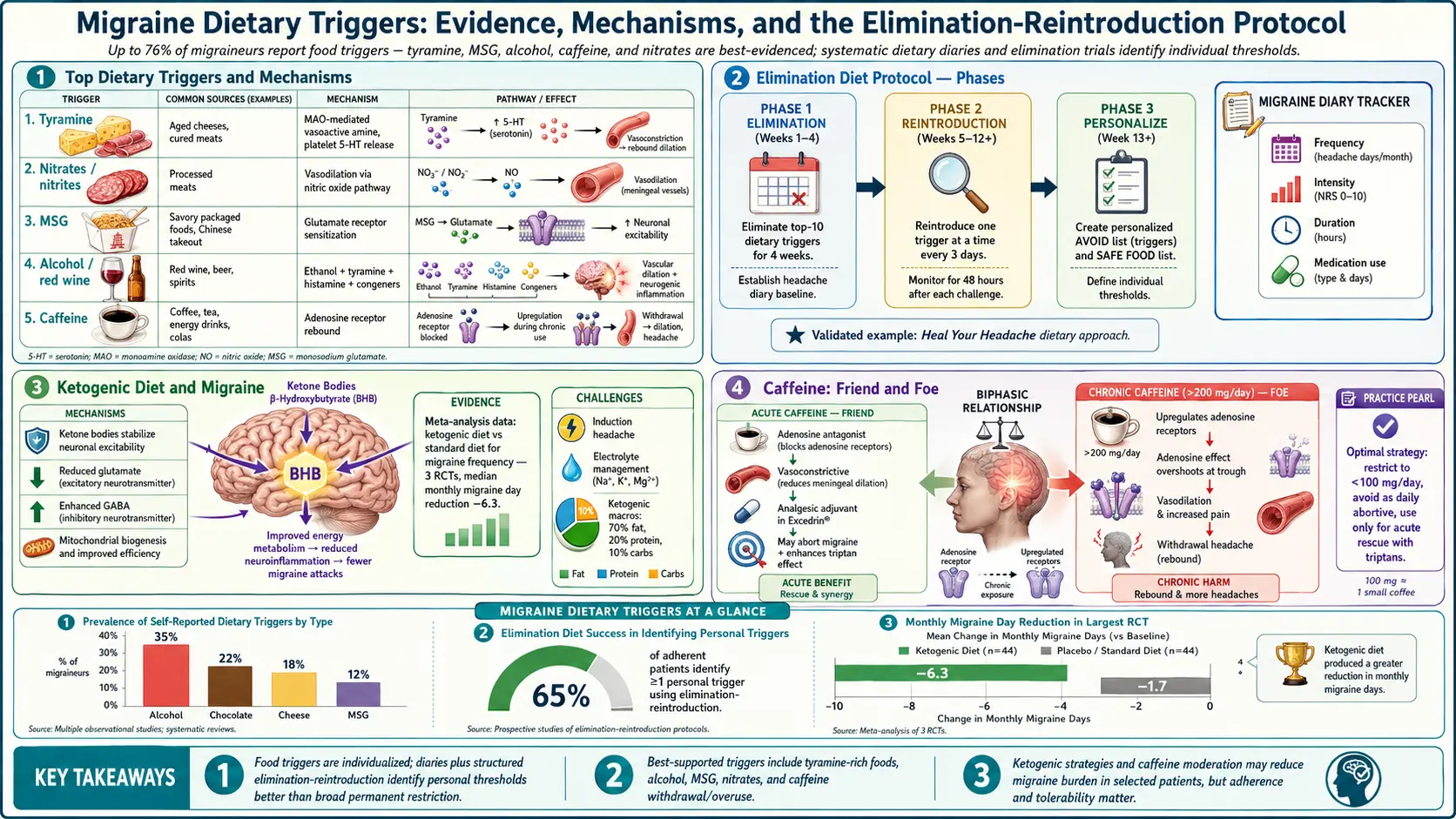
Table of Contents
- The Trigger Problem: Why Most Lists Are Wrong
- Prodromal Cravings vs. Real Triggers
- The Honest Evidence List
- Skipped Meals and Dehydration: The Real #1
- Alcohol — The One Nearly Everyone Agrees On
- Aged Cheeses, Cured Meats, and Tyramine
- MSG, Aspartame, and the Debated Additives
- Caffeine: Both Sides of the Blade
- Histamine, MCAS, and the Overlap
- The Buchholz "Heal Your Headache" Protocol
- Ketogenic and Low-Carb Therapy
- How to Run a Proper N-of-1 Elimination
- Food Sensitivity Tests — What Works and What Doesn't
- Migraine Diary Best Practices
- Sample Meal Plan for the Strict Phase
- Setting Realistic Expectations
- Key Research Papers
- Connections
- Featured Videos
The Trigger Problem: Why Most Lists Are Wrong
If you have searched "migraine food triggers," you have met The List. Every headache clinic pamphlet, every magazine article, every supplement-selling blog prints more or less the same lineup: chocolate, cheese, red wine, citrus, nuts, bananas, onions, processed meat, MSG, aspartame, caffeine. The lists are usually identical because they all copy from one another, and they all trace back to a small number of observational studies from the 1970s and 1980s in which patients reported a food had preceded an attack.
The problem is that self-reported triggers are a notoriously unreliable source of evidence. Attacks are common, cravings are common, and when the two coincide the brain builds a story. When researchers actually provoke migraine patients with suspected food triggers in blinded studies — giving capsules of chocolate extract, tyramine, or aspartame that the patient cannot distinguish from placebo — the trigger reproduces an attack only a minority of the time, and often no more often than the placebo capsule does.
This does not mean diet is irrelevant. It means the popular trigger list is wildly over-inclusive, and most patients who try to avoid twenty foods at once end up with anxiety, disordered eating, and no reduction in attacks. The honest literature supports a much shorter list, plus a careful self-experiment to find your own pattern.
Prodromal Cravings vs. Real Triggers
This is the single most important concept in food-trigger research, and the one most patients have never heard.
A migraine attack does not start with pain. It starts with the prodrome — a phase of neurological changes that begins six to forty-eight hours before the headache itself. Prodromal symptoms include yawning, neck stiffness, mood changes, increased urination, fatigue, irritability, heightened sensitivity to light and sound, and, crucially, food cravings. The hypothalamus, which is already misbehaving during the prodrome, drives cravings for sweet, salty, or fatty foods.
So the classic story — "I ate chocolate and three hours later my migraine started" — is almost always backward. The migraine had already started (prodromally) and the brain, in its prodromal state, reached for the chocolate. The chocolate is an early symptom, not the cause. Peter Goadsby and colleagues have shown this convincingly with studies where patients wore event recorders: prodromal cravings precede attacks whether the person eats the craved food or not.
The same is often true of bananas, citrus, cheese, and sweets. Before you add any food to your personal trigger list, ask: was I already feeling "off" before I ate it? If yes, the food is probably a flag, not a cause.
The Honest Evidence List
Here is what the research actually supports, ranked by the strength and consistency of evidence. Effect sizes are for responders — not everyone reacts to every item.
- Skipped meals / prolonged fasting — the most reproducible trigger across decades of studies. Attacks can follow a missed breakfast or a delayed lunch by two to six hours.
- Dehydration — consistently listed by patients and supported by provocation studies.
- Alcohol, especially red wine and dark spirits — roughly 30–60% of migraine patients identify alcohol as a trigger, and blinded studies support it for wine.
- Caffeine withdrawal — a skipped or delayed usual dose can trigger an attack within 18–24 hours.
- Excess caffeine — above roughly 200–400 mg/day, it can both trigger attacks and drive medication-overuse headache.
- Aged cheeses and cured meats (tyramine, nitrates) — plausible mechanism, modest effect size, probably real in a subset.
- MSG — contested. Blinded studies are mixed. Real in some individuals.
- Aspartame — one of the more controversial. A few provocation studies positive, others negative.
- Histamine-rich foods — matters mostly if you overlap with MCAS or histamine intolerance (see below).
- Chocolate, citrus, bananas, nuts, onions — these sit on every popular list, but blinded provocation evidence is weak-to-absent. Most are probably prodromal cravings being misread as triggers.
Skipped Meals and Dehydration: The Real #1
If you do nothing else from this article, get this one right. The brain of a migraineur runs hot and hungry. Blood glucose dipping for a few hours, or water intake running low across a morning, is enough to tip a susceptible brain toward an attack. This is consistent across every age, every country, every version of the diagnostic criteria.
Practical protocol:
- Eat within one hour of waking. Include protein (eggs, yogurt, leftovers) — not just carbs, which cause a faster dip.
- Do not go more than four to five waking hours without food. Carry a protein bar, nuts, or jerky for days when a meal slips.
- Drink roughly 2 to 2.5 liters (8–10 cups) of water daily, more in hot weather or during exercise. Electrolyte drinks help on heavy-sweat days.
- Avoid long "intermittent fasting" protocols until you have proven they don't provoke attacks. The wellness industry loves 16-hour fasts; migraine brains often don't.
Patients who get only this right often cut attack frequency by 20–30% without touching another trigger.
Alcohol — The One Nearly Everyone Agrees On
Alcohol is the most consistently reported dietary trigger in migraine, and unlike chocolate or cheese, it survives blinded provocation testing. The likely mechanisms are a mixture:
- Ethanol itself is vasoactive and a direct inducer of headache in susceptible people.
- Congeners — the chemical byproducts of fermentation and aging — are higher in darker drinks (red wine, whisky, brandy) and lower in clear spirits (vodka, gin).
- Sulfites in red wine are often blamed. The mechanism is plausible but not cleanly proven.
- Tannins and histamine in red wine may add to the effect.
- Dehydration and sleep disruption from any drinking contribute indirectly.
Practical rules: red wine is the single most common alcoholic offender. White wine, champagne, and dark spirits are intermediate. Clear spirits (vodka, gin, tequila) paired with plenty of water cause the fewest attacks in most patients. If any amount reliably triggers attacks, the honest answer is abstinence — alcohol is dispensable.
Aged Cheeses, Cured Meats, and Tyramine
Tyramine is a vasoactive amine produced when bacteria or molds break down the amino acid tyrosine. It accumulates in aged, cured, or fermented foods: cheddar, Stilton, Parmesan, blue cheese, salami, pepperoni, prosciutto, aged pâtés, soy sauce, miso, sauerkraut, and some broad beans. Nitrates and nitrites in cured meats (hot dogs, bacon, deli ham) are a separate concern and act through nitric oxide pathways, a well-known headache trigger.
A low-tyramine diet favors fresh proteins (fresh meat, fresh fish, eggs), fresh cheese (cottage cheese, ricotta, fresh mozzarella), and foods eaten within 24–48 hours of cooking. Leftovers older than two days, especially protein leftovers, are out — tyramine builds in the fridge.
Effect size is modest. Rockett and colleagues (2012) and others have shown improvement in a subset of patients on a low-tyramine plan, not a uniform benefit. If you try it, give it six weeks before judging, and focus on the biggest-hit items (aged cheese, cured meat, old leftovers) rather than chasing every trace source.
MSG, Aspartame, and the Debated Additives
Monosodium glutamate (MSG) is umami-tasting free glutamate used in Chinese and Southeast Asian cooking, many soups, bouillons, processed snacks, and fast food. Some patients react reliably; many do not. Blinded studies are mixed. If you suspect MSG, do a strict two-to-four-week avoidance, then rechallenge with a clear dose (say, a heavily seasoned broth eaten on an empty stomach). "Glutamate-free" is impossible — free glutamate occurs naturally in parmesan, tomatoes, mushrooms, and aged proteins — but added MSG is avoidable.
Aspartame (NutraSweet, Equal) is the artificial sweetener in many diet sodas and sugar-free products. One small provocation study found a significant increase in attacks on aspartame; others found no effect. The practical move: if you drink diet soda daily and have frequent migraines, drop it for a month. Water, unsweetened sparkling water, or stevia-sweetened alternatives are easy substitutes.
Sucralose (Splenda) and stevia have not been implicated consistently, though individual reactions are always possible.
Caffeine: Both Sides of the Blade
Caffeine is the most contradictory migraine substance. It is a component of acute migraine treatments (Excedrin Migraine contains 65 mg per tablet). Taken acutely, it can abort a developing attack by constricting cerebral vessels and enhancing analgesic absorption. Taken chronically at high doses, it drives medication-overuse headache and makes preventives work less well. And a missed or delayed daily dose can provoke a withdrawal headache within 18–24 hours that is indistinguishable from a migraine attack.
Workable rules:
- Cap daily intake at about 200 mg — roughly one strong mug of coffee or two cups of brewed tea.
- Keep the timing steady. Same dose, same time, every day — including weekends.
- If you want to quit, taper by about 25% per week over a month to avoid withdrawal attacks.
- Do not use caffeinated analgesics (Excedrin, Anacin) more than twice a week. That frequency tips into medication overuse. See the chronic migraine and medication-overuse article for details.
Histamine, MCAS, and the Overlap
Histamine is the chemical your mast cells release during allergic reactions — but it is also present in many foods, and a subset of migraine patients appear to be sensitive to dietary histamine. This overlaps heavily with Mast Cell Activation Syndrome (MCAS) and histamine intolerance. If your migraines come with flushing, itching, hives, GI cramping, rapid heart rate, or reactions to heat, exercise, or alcohol on top of the headache, consider the histamine angle.
High-histamine foods include aged cheese, cured meat, wine and beer, fermented foods (sauerkraut, kimchi, kombucha), tomatoes, spinach, eggplant, avocado, and leftover protein (especially fish). Some foods are not themselves high in histamine but trigger mast cells to release it — strawberries, citrus, chocolate, shellfish.
The practical intervention is a structured low-histamine diet for four to eight weeks. If migraine frequency drops meaningfully, histamine is part of your picture and staying low-histamine (or adding an H1 antihistamine like cetirizine or loratadine daily) is a reasonable long-term strategy. If nothing changes, histamine probably is not your issue and you can stop restricting.
The Buchholz "Heal Your Headache" Protocol
Neurologist David Buchholz's Heal Your Headache (2002) popularized a 6-week strict elimination diet that has become a standard first pass for motivated migraine patients. The protocol avoids, from day one:
- Caffeine (all sources, fully out — not tapered)
- Chocolate
- MSG and hydrolyzed vegetable protein
- Processed meats and anything nitrate/nitrite-cured
- Aged cheese (anything except fresh mozzarella, ricotta, cottage cheese, cream cheese)
- Nuts and peanut butter
- Certain fruits (citrus, bananas, raspberries, red plums, avocados, dried fruits with sulfites)
- Onions (small amounts of cooked onion sometimes tolerated)
- Aspartame
- Alcohol (especially red wine)
- Yogurt and sour cream (cultured dairy)
After six weeks of strict avoidance, foods are reintroduced one at a time, every three to four days, with a diary. Buchholz's reported response rate in his clinic was high, though the protocol has never been subjected to a rigorous randomized trial. It is cheap, safe, and over-inclusive — meaning many of the eliminated foods probably are not your personal triggers, but finding out takes the reintroduction phase. Think of it as a wide net you then narrow.
Ketogenic and Low-Carb Therapy
A growing body of small trials suggests that ketogenic diets — very low carbohydrate (under 50 g/day), moderate protein, high fat, enough to produce blood ketones — can reduce migraine frequency in a substantial minority of patients. The proposed mechanism is improved brain energy metabolism via ketone bodies, plus anti-inflammatory effects. Di Lorenzo and colleagues (2019) found meaningful reductions in attack frequency in episodic migraine patients on a ketogenic protocol.
The practical caveats are real. Ketogenic diets are restrictive, socially difficult, and often cause a rocky "keto flu" first week that can itself include headaches. They clash with the "never skip meals" rule unless you plan carefully. And they are hard to sustain for years. Most migraine clinicians who use keto therapeutically run it for three to six months as a trial, judge the response, then decide whether to continue, taper to a moderate low-carb pattern, or abandon it.
If you want to try it, read up first, eat enough calories, supplement sodium and magnesium, and commit to at least eight weeks before judging. Attacks often spike in week one and drop in weeks four through eight.
How to Run a Proper N-of-1 Elimination
An "N-of-1" trial means you are the only subject — you run a careful self-experiment to find your own triggers. Done right, it is the single most useful dietary tool a migraine patient owns. Done wrong, it becomes a six-month spiral of restriction with no conclusions.
The rules:
- Set a long enough baseline. Six to eight weeks of strict avoidance. Shorter trials miss the effect because migraine frequency is highly variable week-to-week.
- Restrict from a written list, not vibes. Use Buchholz, low-histamine, or low-tyramine as your starting template. Write it on paper and tape it to the fridge.
- Eat enough calories. Under-eating is itself a trigger. Most restricted phases fail because the patient is accidentally running a fast as well as an elimination.
- Hydrate and sleep. If these are off, the elimination is contaminated.
- Keep a daily diary (see below).
- Reintroduce one food every three days, not one per day. The reason is that food-triggered attacks often take 24–48 hours to appear, so back-to-back reintroductions confuse the data.
- On each reintroduction day, eat a real serving — a full wedge of aged cheese, a glass of red wine, not a nibble.
- Log outcomes for 72 hours before adding the next food.
- If an attack follows twice out of three reintroductions, consider that food a probable personal trigger and park it on the avoid list.
- If it causes no attack in three tries, put it back in your diet. It is not your trigger, and staying off it costs you quality of life for no gain.
Food Sensitivity Tests — What Works and What Doesn't
Patients frequently arrive at neurology offices with printouts from IgG food sensitivity panels (EverlyWell, YorkTest, Cyrex, Pinnertest). The bad news: IgG food sensitivity tests are not validated. The American Academy of Allergy, Asthma & Immunology and most national allergy societies recommend against them. IgG antibodies to food simply reflect exposure — if you eat eggs, you have IgG antibodies to eggs. They do not predict symptoms.
Small studies (notably Alpay 2010 in Cephalalgia) have suggested benefit from IgG-guided elimination in migraine, but the effect is most plausibly explained by the fact that any structured elimination helps a subset of people — the IgG panel is just an elaborate random-list generator. The result is often a 20-food restriction built on a shaky scientific foundation.
Skin prick testing and IgE blood testing (allergist-ordered) are different — they measure true IgE-mediated allergy. These are useful if you have suspected anaphylaxis, urticaria, or oral allergy syndrome. They are not the right tool for migraine triggers; IgE allergy and migraine food triggers are different biological mechanisms.
If you have had reactions to mammalian meat, delayed hives, unexplained GI distress, or recurrent idiopathic anaphylaxis, ask about Alpha-Gal Syndrome — a tick-induced IgE allergy to mammalian meat that can present atypically.
Migraine Diary Best Practices
The diary is the data. Without it, you will remember the attacks that fit your current theory and forget the ones that don't. A good diary has five fields per day:
- Date / day of cycle (for menstruating patients — essential for picking up menstrual patterns).
- Sleep (hours, quality).
- Meals and approximate times — with a note on any newly reintroduced food.
- Hydration (rough liters).
- Headache — yes/no, severity 0–10, duration, medication taken, prodromal symptoms noted.
Apps like Migraine Buddy, N1-Headache, or a plain paper notebook all work. What matters is consistency: daily entries, even on no-headache days. Review monthly, looking for patterns across sleep, meals, cycle, weather, and foods. Expect the pattern to take two to three months to emerge — migraine is statistical, not linear.
Sample Meal Plan for the Strict Phase
One week of Buchholz-style, low-histamine-aware, non-skipped-meal eating:
Breakfast (within one hour of waking): Scrambled eggs with fresh mozzarella and cooked spinach (skip spinach if low-histamine). Rice toast or gluten-free toast. Water with lemon (skip lemon if low-histamine). Decaf herbal tea if wanted.
Mid-morning snack: Fresh apple, rice cakes with sunflower seed butter (not peanut), or a hard-boiled egg.
Lunch: Fresh chicken breast (cooked and eaten the same day), white rice or quinoa, roasted carrots and zucchini, olive oil and fresh herbs. A small side salad with olive oil (skip tomatoes if low-histamine). Water.
Afternoon snack: Fresh pear, plain rice crackers, or a small bowl of cottage cheese with blueberries.
Dinner: Fresh-cooked salmon or turkey, sweet potato, steamed broccoli, butter or olive oil. Fresh fruit for dessert.
Evening: Chamomile or peppermint tea. No chocolate, no wine, no aged cheese, no cured meat, no leftovers from more than 24 hours ago.
Boring? Yes. That is the point — it is a diagnostic instrument, not a lifestyle. You live like this for six weeks, collect data, then reintroduce methodically.
Setting Realistic Expectations
Here is the honest forecast, based on the literature and clinical experience:
- About 30–40% of patients who do a strict elimination carefully find at least one meaningful personal trigger.
- Typical attack-frequency reduction in these responders is 20–30% — useful, not miraculous.
- A smaller subset (perhaps 10–15%) are strong responders and cut attacks in half or more.
- Another 40–50% find no reliable food triggers and gain little from dietary restriction.
- Most patients benefit more from the "structure" side — regular meals, hydration, sleep, caffeine discipline — than from eliminating specific foods.
Diet is a real lever. It is not the lever. A proper preventive strategy usually stacks: dietary structure (meals + hydration) + targeted elimination of your personal triggers + sleep hygiene + supplements like magnesium and riboflavin (see the supplements article) + a conventional preventive drug or CGRP monoclonal if frequency is still high. Anyone selling dietary change alone as a cure for frequent migraine is overselling.
Key Research Papers
- Martin VT, Vij B. Diet and headache: Part 1 and Part 2. Headache. 2016.
- Hindiyeh NA, Zhang N, Farrar M, et al. The role of diet and nutrition in migraine triggers and treatment: a systematic literature review. Curr Pain Headache Rep. 2020.
- Rockett FC, de Oliveira VR, Castro K, et al. Dietary aspects of migraine trigger factors. Arq Neuropsiquiatr. 2012.
- Di Lorenzo C, Pinto A, Ienca R, et al. A randomized double-blind, cross-over trial of very low-calorie diet in overweight migraine patients: A possible role for ketones? Front Hum Neurosci. 2019.
Live PubMed Searches
PubMed topic searches for further reading on migraine, diet, and the elimination approach:
- Migraine food triggers
- Migraine prodrome and food craving
- Migraine elimination diet
- Migraine, tyramine, and aged cheese
- Migraine and histamine intolerance
- Migraine and ketogenic diet
- Migraine and caffeine withdrawal
- Migraine and IgG food sensitivity testing
- Migraine, fasting, and skipped meals
Connections
- Mast Cell Activation Syndrome
- Alpha-Gal Syndrome
- Magnesium, Riboflavin, and Supplements
- Low-Histamine Diet
- Migraine Overview
- Elimination Diet
- Chronic Migraine and Medication Overuse
- Menstrual Migraine and Hormonal Triggers
- CGRP Inhibitors and Preventives
- Triptans and Gepants — Acute Treatment
- Vestibular Migraine
- Aura and Visual Disturbances
- SIBO
- MSG
- Aspartame
- Magnesium
- Sulfites
- Fermented Foods
- Headache — the general symptom page: primary versus secondary types, causes, and red flags.