Magnesium, Riboflavin, and Supplements for Migraine
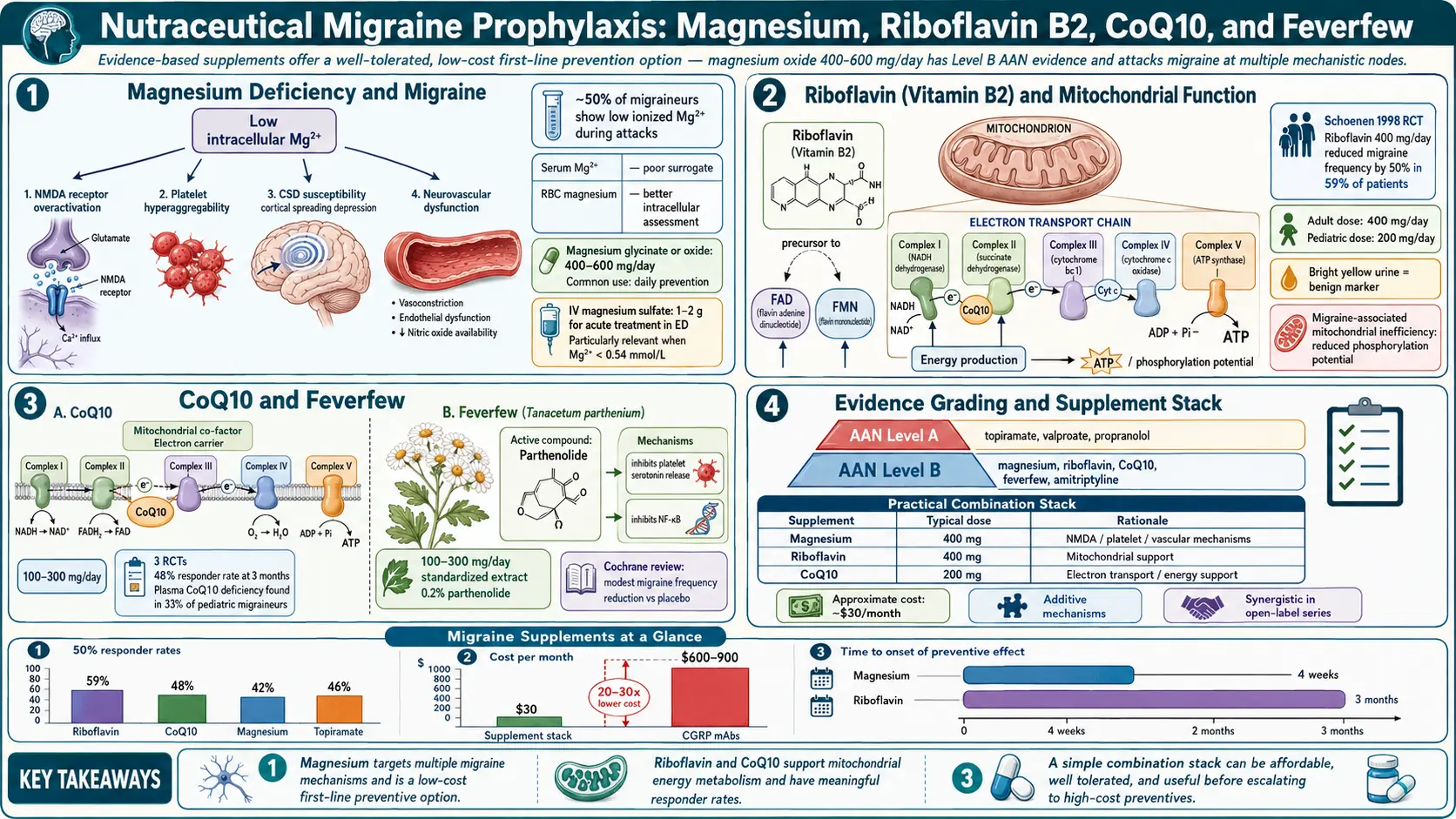
Table of Contents
- Why Supplements Are a Legitimate Part of Migraine Care
- The AAN/AHS Evidence Tiers — What the Guidelines Actually Say
- Realistic Expectations: What "Works" Means
- Magnesium — The First-Line Supplement
- Riboflavin (Vitamin B2) — The Mitochondrial Vitamin
- Feverfew — The Old Herbal with New Evidence
- CoQ10 — Mitochondrial Backup
- Butterbur — Effective, but Read This First
- Melatonin — The Sleep-Migraine Bridge
- Vitamin D, Omega-3s, B12/Folate, and Iron
- Stacking, Timing, and How to Test One at a Time
- Pregnancy, Breastfeeding, and Pediatric Dosing
- Drug Interactions Worth Knowing
- Quality Sourcing — Why the Label Matters
- Why "Natural" Does Not Equal "Safe"
- Key Research Papers
- Connections
- Featured Videos
Why Supplements Are a Legitimate Part of Migraine Care
Supplements sit in a strange corner of medicine. Some people treat them as candy; others dismiss anything without a patent as quackery. For migraine, neither extreme matches the evidence. The American Academy of Neurology (AAN) and the American Headache Society (AHS) published a joint practice guideline in 2012 that formally graded nutraceuticals and complementary therapies for migraine prevention. Several supplements cleared the bar for real, recommendable evidence. They did not top prescription medicines in head-to-head strength, but they are cheap, accessible, low-risk in most cases, and stackable with prescription therapies. For many patients, they are the quiet backbone of a 50% reduction in monthly migraine days.
This article walks through the supplements with the strongest evidence, the correct dose and form, what to expect, and where "natural" hides real dangers. Nothing here replaces a conversation with your neurologist, but by the end you should know enough to have that conversation as an informed partner rather than a passive recipient.
The AAN/AHS Evidence Tiers — What the Guidelines Actually Say
The 2012 Holland et al. guideline (updated commentary through the late 2010s) grades preventive therapies by the quality and consistency of trials supporting them:
- Level A (established effective). For nutraceuticals, no product reached Level A with consistent evidence. This is the disappointment of the field — nothing in the supplement aisle is as reliably proven as a prescription beta-blocker or topiramate. Anyone promising Level-A certainty from a bottle is overselling.
- Level B (probably effective). Magnesium, riboflavin (vitamin B2), and feverfew (MIG-99 standardized extract). Recommended by the guideline for migraine prevention.
- Level C (possibly effective). Coenzyme Q10 (CoQ10) and, controversially, butterbur. Butterbur was originally Level A but has been effectively withdrawn from clinical use because of liver toxicity risk from improperly processed products — more on this below.
- Level U (inadequate data). Most everything else your cousin on Instagram is recommending.
Translation: magnesium, riboflavin, and MIG-99 feverfew have the strongest case. CoQ10 is a reasonable addition. Butterbur works but must be used with extreme caution. Everything else is optional.
Realistic Expectations: What "Works" Means
In supplement trials for migraine prevention, "responder" is usually defined as a 50% or greater reduction in monthly migraine days. By that definition, magnesium, riboflavin, feverfew, and CoQ10 each help roughly one in three users. Not everyone. Not a cure. The typical responder sees a 20–50% drop in attack frequency, intensity, or both. Two-thirds of trial participants are non-responders and would have been better off switching.
The other hard rule: give it 8 to 12 weeks before you judge. Magnesium needs time to fill intracellular stores. Riboflavin is thought to work by gradually improving mitochondrial energy metabolism. Feverfew and CoQ10 both take a similar runway. If you quit at four weeks because "nothing happened," you will never know whether you were a responder. Keep a simple headache diary — date, severity 0 to 10, duration, rescue medication used — and compare the 4-week window before starting the supplement to weeks 9 through 12. That is the honest answer.
Magnesium — The First-Line Supplement
Mechanism. Magnesium is a cofactor for more than 300 enzymatic reactions. In migraine biology, the case for supplementing rests on several observations: migraineurs have lower serum and intracellular magnesium than non-migraineurs on average; magnesium modulates NMDA-receptor activity in the cortex (which is central to cortical spreading depression, the wave of electrical silence that underlies aura); it regulates vascular tone; it blocks calcium influx; and it stabilizes the release of neurotransmitters including serotonin and CGRP. A reasonable mental model is that magnesium raises the threshold at which the migraine cascade can fire.
Dose. Clinical trial evidence, including Peikert et al. 1996, used 600 mg of elemental magnesium per day. The practical target is 400–600 mg of elemental magnesium, usually split into two or three doses. "Elemental" matters because a 500 mg magnesium glycinate capsule is not 500 mg of magnesium — the glycine takes up most of the weight, and the elemental content may be 80–100 mg. Read the label carefully for "elemental magnesium per serving."
Form. This is where most people get it wrong:
- Magnesium glycinate (bisglycinate). Excellent absorption, gentle on the gut, rarely causes diarrhea. A sensible default.
- Magnesium malate. Well absorbed; the malate ion is a Krebs-cycle intermediate, sometimes chosen by people who also report fatigue.
- Magnesium threonate. Crosses the blood-brain barrier more efficiently in animal studies and is marketed for cognitive and neurological conditions. Expensive. Reasonable if glycinate has not helped after three months.
- Magnesium citrate. Cheap and decently absorbed, but often causes loose stools at the 400–600 mg elemental dose needed for migraine.
- Magnesium oxide. The form in most cheap drugstore bottles. Poorly absorbed (bioavailability under 5% by some measures), mostly useful as a laxative. Avoid for migraine.
Side effects. Loose stools are the main limit. If you see them, reduce the dose, split it across more doses, or switch form. True magnesium toxicity is rare in people with normal kidney function. If you have moderate-to-severe chronic kidney disease, do not self-supplement — talk to your nephrologist first.
Riboflavin (Vitamin B2) — The Mitochondrial Vitamin
Mechanism. Riboflavin is the precursor of flavin adenine dinucleotide (FAD) and flavin mononucleotide (FMN), two essential coenzymes in the mitochondrial electron transport chain. Migraine brains show evidence of impaired mitochondrial energy production between attacks — lower phosphocreatine levels on MR spectroscopy, altered ATP turnover. The hypothesis is straightforward: give the mitochondria more of the raw material they need and the energy deficit gets smaller.
Dose. The classic trial, Schoenen et al. 1998, used 400 mg once daily and reported a reduction in attack frequency from 4 to 2 per month after 3 months in responders. That single 400 mg evening dose remains the standard.
Form and timing. Plain riboflavin (not riboflavin-5-phosphate, not a B-complex with 50 mg of B2) at 400 mg. Take it with an evening meal — it is best absorbed with food, and in some people a morning dose is mildly activating.
What to expect. Your urine will turn bright fluorescent yellow. This is not a warning sign — it is the unabsorbed riboflavin coming out in the urine and is completely normal. Side effects are otherwise minimal. Rare reports of nausea or loose stools. Riboflavin has one of the cleanest safety profiles of any migraine therapy.
Timeline. Benefit emerges at 8 to 12 weeks, not earlier. A 400 mg dose for 30 days is not a fair trial.
Feverfew — The Old Herbal with New Evidence
What it is. Tanacetum parthenium, a daisy-family herb used for fevers and "head pain" in European folk medicine since at least the Middle Ages. The active compound is thought to be parthenolide, a sesquiterpene lactone that inhibits serotonin release from platelets and dampens inflammatory signaling (NF-κB).
Dose. Two preparations have evidence:
- MIG-99 (Diener et al. 2005) — a CO2-extracted, standardized feverfew extract at 6.25 mg three times daily. This is the preparation that earned Level B in the AAN/AHS guideline.
- Whole-leaf standardized extracts at 100–300 mg per day, standardized to at least 0.2% parthenolide. Less rigorous trial evidence than MIG-99 but widely used.
Side effects. Mouth ulcers and "post-feverfew syndrome" (rebound headache, anxiety, joint stiffness) on abrupt discontinuation after long use. Taper off over a week or two rather than stopping cold.
Cautions. Feverfew is in the daisy/ragweed family — if you have significant allergy to those plants, skip it. It has mild antiplatelet activity, so avoid combining with warfarin, high-dose fish oil, or other blood thinners without physician oversight. Do not use in pregnancy. Feverfew can stimulate uterine contractions and is traditionally considered an emmenagogue.
CoQ10 — Mitochondrial Backup
Mechanism. Coenzyme Q10 is an electron carrier in the mitochondrial respiratory chain, essentially working in the same system as riboflavin. The rationale for supplementing is identical: shore up mitochondrial energy in a brain that appears to run slightly energy-starved between attacks.
Evidence. Level C in AAN/AHS — one small randomized trial (Sandor et al. 2005) and several open-label studies show a roughly 50% reduction in migraine days for about half of users over three months. Not as strong as magnesium or riboflavin, but consistent enough to be worth a trial.
Dose and form. 300 mg per day is the most common trial dose, usually split as 100 mg three times daily with meals (CoQ10 is fat-soluble; take with food containing fat). The two market forms are ubiquinone (the oxidized form) and ubiquinol (the reduced, active form). Ubiquinol is better absorbed, especially over age 40, and is the preferred form despite costing more. If budget is an issue, ubiquinone with a meal that contains fat still works.
Side effects. Minimal. Occasional GI upset or mild insomnia if taken at bedtime (take with breakfast and lunch instead).
Butterbur — Effective, but Read This First
Butterbur (Petasites hybridus) is the most complicated entry in the list. The standardized extract Petadolex was originally Level A in the AAN/AHS guideline, with well-designed trials showing roughly 50% reductions in migraine frequency. Then came the problem.
Raw butterbur root contains pyrrolizidine alkaloids (PAs) — liver toxins that can cause veno-occlusive disease, hepatitis, and fatal liver failure. Manufacturing processes can remove PAs, but not all manufacturers do this reliably. Multiple cases of severe hepatotoxicity prompted regulators in Germany and the UK to withdraw butterbur products, and the AHS effectively downgraded the recommendation. Most headache specialists no longer recommend butterbur because the supply chain cannot be trusted.
If you use butterbur anyway:
- Only a product certified "pyrrolizidine-alkaloid-free" (e.g., authentic Petadolex from a European source that still makes it to a verified spec). Do not buy generic "butterbur root" from Amazon.
- 75 mg twice daily is the trial dose.
- Get baseline liver function tests (ALT, AST, bilirubin) before starting and repeat at 3 months, then every 6 months.
- Stop immediately and see your doctor if you develop abdominal pain, jaundice, dark urine, or unexplained fatigue.
For most patients, the risk-to-benefit ratio now favors choosing something else on this list. Butterbur is the clearest example of why "natural" is not a synonym for "safe."
Melatonin — The Sleep-Migraine Bridge
Melatonin is the newest serious entry in the migraine preventive toolkit. A 2016 randomized trial by Gonçalves et al. found that 3 mg of melatonin at bedtime was as effective as amitriptyline 25 mg for migraine prevention, with far fewer side effects. Subsequent studies have largely supported modest benefit, especially in patients whose migraines cluster around sleep disruption, shift work, or irregular circadian rhythm.
Dose. 3 mg at bedtime, 30–60 minutes before sleep. Higher doses (5–10 mg) are not more effective and may disrupt natural melatonin rhythms. Start lower (1 mg) and work up if 3 mg is too sedating.
Form. Immediate-release is used in the trials. Choose a USP-verified brand — melatonin products have notoriously inconsistent labeling, with independent testing finding actual contents from 17% to 478% of the label claim.
Side effects. Vivid dreams, mild morning grogginess, and occasional next-day headache paradoxically. Safe in most adults. Discuss with your doctor before using in children, teenagers, or during pregnancy.
Vitamin D, Omega-3s, B12/Folate, and Iron
These are the supplements that help if you are deficient but are not general migraine preventives for everyone.
Vitamin D. Migraine prevalence is higher in people with 25-hydroxyvitamin D below 20 ng/mL. Correcting documented deficiency with 1,000–4,000 IU/day is reasonable. Do not megadose blindly — ask your physician to check a level first and retest after 3 months.
Omega-3 fatty acids (EPA/DHA). A 2021 trial by Ramsden et al. found that increasing omega-3 intake (to about 1.5 g/day of combined EPA+DHA) while lowering linoleic acid reduced migraine days. The mechanism is thought to involve anti-inflammatory lipid mediators. 1–2 g of combined EPA+DHA from a molecularly distilled fish oil or algae-based product is a reasonable dose.
B12 and folate — the MTHFR angle. Patients with MTHFR C677T or A1298C polymorphisms have reduced methylation capacity and higher homocysteine, and several studies link this pattern to migraine with aura. If you have tested positive for MTHFR, daily methylfolate (L-5-MTHF) 400–1,000 mcg plus methylcobalamin (B12) 500–1,000 mcg is a reasonable addition. Routine MTHFR testing for everyone with migraine is not standard.
Iron. Migraine (especially in menstruating women) sometimes runs with iron deficiency. Check ferritin, not just hemoglobin. If ferritin is below 75 ng/mL, iron repletion frequently reduces both fatigue and headache load even when hemoglobin is technically normal. Oral iron bisglycinate 25–45 mg elemental every other day is well tolerated; recheck ferritin at 3 months.
Stacking, Timing, and How to Test One at a Time
It is tempting to start magnesium, riboflavin, CoQ10, and feverfew simultaneously on Monday morning. Resist this. If things improve, you will not know which supplement earned the win, and you will feel locked into a four-bottle daily ritual forever.
A better protocol:
- Start with magnesium at 400 mg elemental glycinate for 8–12 weeks. Track headache days. If clearly better, keep it and move to step 2. If no effect, keep low-dose magnesium anyway (200 mg) for its other benefits (sleep, constipation, muscle tension) and move on.
- Add riboflavin 400 mg at dinner for another 8–12 weeks. Re-evaluate.
- Consider feverfew MIG-99 or CoQ10 ubiquinol as a third agent if needed.
- Re-evaluate annually. Some supplements plateau. Some become unnecessary when prescription preventives kick in. Revisit the stack once a year and drop anything that cannot justify its place.
Stacking magnesium, riboflavin, CoQ10, and MIG-99 feverfew together is safe for most adults. Adding butterbur to the mix raises liver-monitoring needs but is not chemically incompatible.
Pregnancy, Breastfeeding, and Pediatric Dosing
Pregnancy.
- Magnesium — yes. Magnesium is used therapeutically in pregnancy (including for pre-eclampsia) and is considered safe at 300–400 mg elemental daily. Stick to glycinate or citrate.
- Riboflavin — yes. Required nutrient, safe at 400 mg. Widely used for migraine prevention in pregnancy when prescription preventives are off-limits.
- CoQ10 — probably yes. Limited data but no safety signals; often used by fertility specialists during pregnancy.
- Feverfew — no. Uterine stimulant, contraindicated in pregnancy.
- Butterbur — no. Pyrrolizidine-alkaloid concerns apply to the fetus as well as the mother.
- Melatonin — discuss. Limited data; short-term low-dose use may be acceptable but should be a shared decision with your OB.
Breastfeeding. Magnesium, riboflavin, and CoQ10 are generally considered compatible. Feverfew and butterbur are not.
Pediatric dosing. The pediatric migraine evidence is more limited but suggests:
- Magnesium oxide (yes, oxide is used in pediatric trials specifically) 9 mg/kg/day split into 2–3 doses.
- Riboflavin 100–400 mg/day depending on age and weight; many pediatric headache specialists use 200 mg in children under 12.
- CoQ10 1–3 mg/kg/day.
- Feverfew and butterbur are generally avoided in children.
Always run pediatric supplementation by a pediatric neurologist or headache specialist.
Drug Interactions Worth Knowing
- Magnesium + fluoroquinolone antibiotics (ciprofloxacin, levofloxacin) — magnesium binds the antibiotic in the gut and reduces absorption. Separate doses by at least 2 hours before or 6 hours after the antibiotic.
- Magnesium + levothyroxine (Synthroid) — same binding problem. Take levothyroxine first thing in the morning on an empty stomach; take magnesium at least 4 hours later.
- Magnesium + tetracyclines, bisphosphonates — separate by at least 2 hours.
- CoQ10 + warfarin — CoQ10 has structural similarity to vitamin K and may modestly reduce warfarin's effect. If you are on warfarin and start CoQ10, tell your anticoagulation clinic and expect INR monitoring.
- Feverfew + antiplatelet/anticoagulant drugs — additive bleeding risk. Avoid combining without physician awareness.
- Melatonin + sedatives, antihypertensives, immunosuppressants — multiple modest interactions. Mention melatonin to every prescriber.
- Riboflavin — notably interaction-free. One of the reasons it is a favorite in complex medication regimens.
Quality Sourcing — Why the Label Matters
The U.S. supplement industry is regulated far more loosely than the pharmaceutical industry. Independent testing repeatedly finds products with wrong doses, undeclared fillers, or active contamination. For migraine prevention, where you are committing to a 3-month minimum trial, the cost of a bad bottle is not just money — it is a failed trial that might have worked with a real product.
Look for these third-party certifications on the label:
- USP Verified — United States Pharmacopeia tested the actual contents.
- NSF Certified or NSF Contents Certified.
- ConsumerLab.com Approved.
- Informed Sport / Informed Choice — tested for contaminants; relevant if you are an athlete.
Brands with consistently strong independent test results (not exhaustive, not paid endorsements): Thorne, Pure Encapsulations, Nordic Naturals (omega-3), Jarrow Formulas, NOW Foods (especially their USP-verified lines), Life Extension, Designs for Health, Douglas Laboratories. For butterbur specifically, only authentic Petadolex from a pharmaceutical-grade manufacturer.
Avoid products whose primary selling point is "proprietary blend" — you cannot verify doses of individual ingredients. Avoid multi-ingredient "migraine formulas" where each individual component is sub-therapeutic. It is almost always better to take one high-quality single-ingredient product per target.
Why "Natural" Does Not Equal "Safe"
The butterbur story is the cleanest cautionary tale in migraine supplementation, but it is not alone. Kava kava, germander, comfrey, pennyroyal, and certain Chinese herbal mixes have all been linked to fatal hepatotoxicity. Feverfew interacts with anticoagulants. High-dose vitamin A is teratogenic. Excess iron causes oxidative stress and, in hemochromatosis carriers, organ damage.
"Natural" describes where a molecule came from, not what it does once it is inside you. A rattlesnake is natural. Arsenic is natural. The question worth asking for any supplement is the same question you would ask for a prescription medication:
- What is the mechanism and is it plausible?
- What does the trial evidence actually show?
- What is the dose, and does my product contain it?
- What are the realistic side effects and rare but serious risks?
- What interactions exist with my other medications?
- When will I know it is working, and how will I decide to stop?
If you can answer these six questions for every bottle in your cabinet, you are using supplements as medicine. If you cannot, you are using them as hope. Migraine deserves the first approach.
Key Research Papers
- Holland S, Silberstein SD, Freitag F, et al. Evidence-based guideline update: NSAIDs and other complementary treatments for episodic migraine prevention in adults. Report of the Quality Standards Subcommittee of the AAN and the AHS. Neurology. 2012;78(17):1346–1353.
- Peikert A, Wilimzig C, Köhne-Volland R. Prophylaxis of migraine with oral magnesium: results from a prospective, multi-center, placebo-controlled and double-blind randomized study. Cephalalgia. 1996;16(4):257–263.
- Schoenen J, Jacquy J, Lenaerts M. Effectiveness of high-dose riboflavin in migraine prophylaxis: a randomized controlled trial. Neurology. 1998;50(2):466–470.
- Diener HC, Pfaffenrath V, Schnitker J, et al. Efficacy and safety of 6.25 mg t.i.d. feverfew CO2-extract (MIG-99) in migraine prevention — a randomized, double-blind, multicentre, placebo-controlled study. Cephalalgia. 2005;25(11):1031–1041.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on nutraceutical migraine prevention:
- Magnesium and migraine prevention
- Riboflavin and migraine prophylaxis
- Coenzyme Q10 and migraine
- Feverfew MIG-99 and migraine
- Butterbur, Petasites, migraine, and hepatotoxicity
- Melatonin and migraine prevention
- Vitamin D and migraine
- Omega-3 fatty acids (EPA/DHA) and migraine
- MTHFR, methylfolate, and migraine with aura
- Ferritin, iron deficiency, and migraine
Connections
- Magnesium
- Migraine Overview
- Vitamin B2 (Riboflavin)
- Chronic Migraine and Medication Overuse
- Menstrual Migraine and Hormonal Triggers
- Diet Triggers and Elimination Protocol
- CGRP Inhibitors and Preventives
- Triptans and Gepants — Acute Treatment
- Vestibular Migraine
- Aura and Visual Disturbances
- Riboflavin and Migraine Prevention
- Magnesium and Sleep
- Headache
- Insomnia
- Magnesium Glycinate
- Omega-3 Fatty Acids
- Magnesium Replenishment
- Migraine in Pregnancy and Breastfeeding
- Butterbur — the full profile, including the pyrrolizidine-alkaloid liver toxicity that drove it out of routine use.