Migraine in Pregnancy & Breastfeeding
If you live with migraine and you are pregnant, trying to conceive, or breastfeeding, you probably have two questions circling in your head: Will my migraines get better or worse? and What can I safely take if one hits? This article walks through both — the hormonal shifts that change migraine patterns across pregnancy and postpartum, the red flags that should never be dismissed as "just another migraine," and a practical tier of acute and preventive options with the best available safety data.
A note on tone: medication decisions in pregnancy and lactation are individual. Nothing here replaces a conversation with your obstetrician, headache specialist, or a maternal-fetal medicine pharmacist. What this page can do is help you walk into that conversation already knowing the landscape.
Table of Contents
- What Usually Changes — and Why
- When Migraine Does Not Improve (or Gets Worse)
- New-Onset Headache in Pregnancy: The Red-Flag Workup
- Acute Treatment Tier in Pregnancy
- Preventives Generally Considered Acceptable
- Preventives to Avoid in Pregnancy
- Status Migrainosus and the Emergency Department Plan
- Postpartum Migraine Surge and Stroke Risk
- Breastfeeding Compatibility
- Key Research Papers
- Connections
- Featured Videos
What Usually Changes — and Why
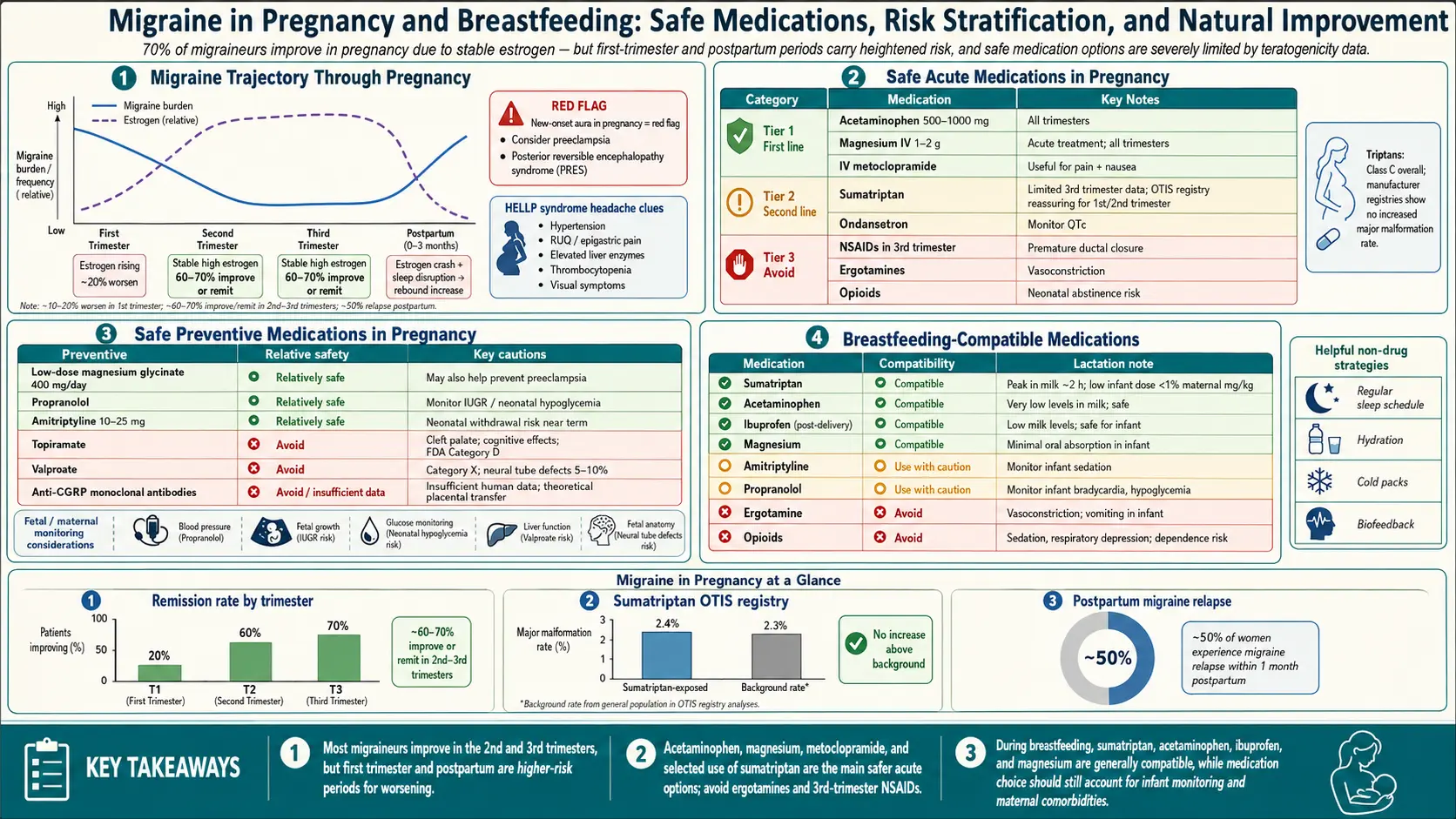
The headline statistic most neurologists quote is this: roughly 50–75% of women with migraine improve during pregnancy, with the biggest gains in the second and third trimesters. Some women stop having attacks entirely. The reason is hormonal. Estrogen levels rise steadily through pregnancy and — crucially — stay stable at high levels, rather than cycling up and down every month. Migraine brains seem to react less to a high-but-steady estrogen environment than to the sharp monthly drop that normally triggers menstrual attacks.
The first trimester is the bumpy part. Estrogen is climbing but nausea, dehydration, interrupted sleep, and the sudden stop of any preventive medication can together make the first 12 weeks feel worse, not better. If you can get through the first trimester, the second and third usually bring meaningful relief.
For more on how estrogen drives attacks, see Menstrual Migraine and Hormonal Triggers.
When Migraine Does Not Improve (or Gets Worse)
The 50–75% improvement figure hides an important subgroup: migraine with aura. Women who have aura are less likely to improve in pregnancy, and a meaningful minority get worse. A few patterns to know:
- Migraine without aura — highest improvement rate; many women become attack-free by the second trimester.
- Migraine with aura — lower improvement rate. Aura may appear for the first time in pregnancy, or become more frequent.
- New-onset aura — a woman who has always had migraine without aura may develop aura for the first time during pregnancy. This is not automatically dangerous but it does warrant medical review (see the red-flag section below).
- Chronic migraine — if you were on daily preventives pre-pregnancy, stopping them (as often happens in the first trimester) can mean a rebound worsening.
New-Onset Headache in Pregnancy: The Red-Flag Workup
Not every bad headache in pregnancy is a migraine. Pregnancy itself raises the risk of several serious conditions that can masquerade as migraine, and the stakes of missing them are very high. Any new or significantly different headache in pregnancy — especially in the second half — deserves a same-day medical evaluation.
The main differential diagnoses to rule out:
- Preeclampsia. The headache is often bilateral, throbbing, and resistant to usual analgesics. Look for blood pressure ≥ 140/90, proteinuria, visual changes (blurring, scotomata), right-upper-quadrant pain, or sudden swelling of hands and face. Preeclampsia is the single most important call to make after 20 weeks of gestation.
- Cerebral venous sinus thrombosis (CVST). Pregnancy and the postpartum period are hypercoagulable. A progressive, unrelenting headache that builds over days — sometimes with focal neurological signs or seizures — can be CVST. It is a neurological emergency.
- Ischemic or hemorrhagic stroke. Sudden-onset "thunderclap" headache, one-sided weakness, speech changes, or a headache that is categorically the worst you have ever had.
- Reversible cerebral vasoconstriction syndrome (RCVS) / posterior reversible encephalopathy syndrome (PRES). Both cluster around pregnancy and postpartum, often with extreme blood pressures.
- Pituitary apoplexy and idiopathic intracranial hypertension — less common but on the list.
Red-flag features that should trigger urgent (same-day) evaluation: thunderclap onset; fever; neck stiffness; new neurological deficit; seizure; visual loss; severe hypertension; the worst headache of your life; a headache that is qualitatively different from your usual pattern. Do not talk yourself out of calling. Obstetric triage exists precisely for this.
See also Preeclampsia and Aura and Visual Disturbances.
Acute Treatment Tier in Pregnancy
When an attack does break through, there is a rough tier of options ordered from most to least safety data in pregnancy. Always confirm with your own prescriber.
First line — acetaminophen (paracetamol). 500–1000 mg is the standard first-line acute treatment throughout pregnancy. Large observational datasets have raised questions about heavy, prolonged prenatal exposure and child neurodevelopment, but short, episodic use for migraine is considered the safest analgesic choice. Use the lowest effective dose, not chronically.
Non-pharmacologic rescue. Cold packs, a dark quiet room, hydration with electrolytes, a caffeine-containing beverage (within the 200 mg/day pregnancy limit), sleep. These sound trivial but genuinely abort many attacks before they escalate.
Antiemetics. Pregnancy-associated nausea plus migraine nausea is a miserable combination. Metoclopramide and ondansetron (after the first trimester, with some caveats) are commonly used. Metoclopramide also has mild anti-migraine activity.
Triptans. Sumatriptan has the most pregnancy safety data of any triptan — pregnancy registries run by drug manufacturers and Scandinavian national databases have followed thousands of exposed pregnancies without finding a clear increase in major malformations or adverse outcomes. Triptans are not FDA Category A (no drug is fully "proven safe" in pregnancy) but many headache specialists consider sumatriptan acceptable when acetaminophen fails, particularly if the alternative is a severe, dehydrating, intractable attack. Other triptans have less data but are probably broadly similar; sumatriptan remains the default. See Triptans and Gepants for the broader landscape.
NSAIDs (ibuprofen, naproxen, ketorolac). Can be used cautiously in the second trimester and are generally avoided in the first. Do not use NSAIDs after 30 weeks of gestation — they can cause premature closure of the fetal ductus arteriosus and oligohydramnios. In October 2020 the FDA extended this warning to include use from 20 weeks onward.
Ergots (ergotamine, dihydroergotamine). Avoid absolutely in pregnancy. They cause uterine contractions and vasoconstriction and carry known fetal risks.
Gepants (rimegepant, ubrogepant, atogepant) and ditans (lasmiditan). Insufficient human pregnancy data to recommend. Not first choice.
Opioids. Generally avoided. They do not treat migraine well, are associated with medication-overuse headache, and carry neonatal withdrawal risk with regular late-pregnancy use.
Preventives Generally Considered Acceptable
If your attack frequency is high enough to warrant prevention during pregnancy, several options have reasonable reassuring data. None is truly risk-free, and the decision always compares the drug risk against the harm of uncontrolled severe migraine (dehydration, missed nutrition, depression, medication overuse).
- Propranolol (and, less commonly, metoprolol). The beta-blocker with the most pregnancy data. Can cause fetal growth restriction and neonatal bradycardia/hypoglycemia if used near delivery, so dose and monitoring matter — but it is frequently used for migraine prevention in pregnancy.
- Cyproheptadine. An older antihistamine with anti-serotonergic activity. Used particularly in women who cannot tolerate beta-blockers.
- Magnesium. Oral magnesium 400 mg of elemental magnesium daily has migraine-preventive evidence and an excellent pregnancy safety profile. Glycinate or citrate forms are gentler on the gut than oxide. See Magnesium and Magnesium and Riboflavin. Note: intravenous magnesium has been linked to fetal bone issues with prolonged use, but oral dosing at preventive levels is standard.
- Riboflavin (vitamin B2) 400 mg daily. Water-soluble, essentially no fetal risk signal, and evidence for roughly halving attack frequency in responders.
- Coenzyme Q10 100–300 mg daily. Limited but reassuring pregnancy data; some evidence also for reducing preeclampsia risk in high-risk women.
- Non-drug preventives. Cognitive-behavioral therapy, biofeedback, sleep hygiene, trigger avoidance, regular meals, and hydration remain cornerstones and carry zero fetal risk.
Preventives to Avoid in Pregnancy
- Topiramate. Associated with cleft lip and cleft palate and with lower birth weight. Should be discontinued before conception when possible. Also reduces the effectiveness of some oral contraceptives, complicating preconception planning.
- Valproate (divalproex). Absolutely contraindicated. One of the strongest known human teratogens: causes neural tube defects, craniofacial abnormalities, and significant reductions in childhood IQ. Should not be used in any woman who could become pregnant without robust contraception and informed consent.
- ACE inhibitors and ARBs (lisinopril, candesartan, valsartan). Fetal kidney damage, oligohydramnios, and skull malformations — especially in the second and third trimesters. Candesartan is sometimes used off-label for migraine prevention; it must be stopped before conception.
- CGRP monoclonal antibodies (erenumab, fremanezumab, galcanezumab, eptinezumab). These drugs have very long half-lives (weeks to months) and inadequate human pregnancy data. Most guidelines advise stopping at least 5 months before conception. See CGRP Inhibitors and Preventives.
- Gepants as daily preventives (atogepant, rimegepant). Inadequate pregnancy data.
- OnabotulinumtoxinA (Botox) for chronic migraine. Limited data; most headache specialists pause Botox during pregnancy. Some continue it in carefully selected, severely affected patients — this is an individualized decision.
Status Migrainosus and the Emergency Department Plan
Status migrainosus — a debilitating migraine lasting more than 72 hours — happens in pregnancy too, and it is not a time to tough it out at home. Severe dehydration, ketosis, and inability to eat are themselves risks to the pregnancy. Triage to obstetric or emergency evaluation so that they can:
- Rule out preeclampsia and other red-flag diagnoses (blood pressure, urine, neurological exam, sometimes imaging).
- Give IV fluids — often transformative on their own.
- Administer IV magnesium sulfate (which doubles as preeclampsia prophylaxis and a migraine abortive in some protocols).
- Use IV metoclopramide, ondansetron, or prochlorperazine for nausea and as a migraine abortive.
- Consider a short course of oral or IV steroids (methylprednisolone) for particularly resistant cases; short prednisone courses are generally considered acceptable.
- Consider occipital or sphenopalatine nerve blocks — local anesthetic only, no systemic drug exposure.
Postpartum Migraine Surge and Stroke Risk
The protective estrogen bath ends abruptly at delivery. Within the first week postpartum, estrogen drops from pregnancy levels back toward baseline, and many women experience a sharp postpartum migraine surge. Roughly a third of women who improved in pregnancy have an attack within the first week after delivery, and more over the first month. Sleep deprivation, dehydration from breastfeeding, and the huge hormonal swing all contribute.
Two safety points matter here:
- Stroke risk is elevated throughout pregnancy and especially postpartum — and migraine, particularly migraine with aura, is an independent contributor. Smoking and combined hormonal contraception stack on top. Any woman with migraine with aura should avoid smoking and should usually avoid combined (estrogen-containing) oral contraceptives; progestin-only methods are generally preferred. This matters now, in the postpartum weeks when you will be choosing contraception.
- A new, severe, or unusual headache in the first six weeks postpartum is never "just postpartum migraine" until CVST, preeclampsia/eclampsia, RCVS, PRES, and pituitary apoplexy have been considered. Get it evaluated.
Breastfeeding Compatibility
The U.S. National Library of Medicine's LactMed database is the gold-standard free resource for breastfeeding medication questions. A quick summary for migraine drugs:
- Acetaminophen. Compatible. Minimal milk transfer.
- Ibuprofen. Compatible and generally preferred NSAID in lactation — very low milk levels.
- Sumatriptan. Compatible per LactMed. Milk levels are very low and oral bioavailability in the infant is poor. Some older sources suggested pumping and discarding for 8–12 hours; current LactMed guidance is that this is not necessary for most mothers. Eletriptan is also listed as compatible.
- Propranolol. Compatible; low milk levels.
- Metoclopramide. Compatible short-term; long courses are avoided because of maternal side effects.
- Magnesium, riboflavin, CoQ10. Compatible.
- Ergots. Avoid. They can suppress prolactin and reduce milk supply and carry infant risk.
- Topiramate. Transfers into milk at meaningful levels; monitor the infant for sedation, poor feeding, and diarrhea if the mother is on topiramate.
- CGRP monoclonal antibodies. Molecules are large and oral absorption in the infant is expected to be minimal, but human lactation data are sparse. Many clinicians consider them acceptable after shared decision-making; others prefer to wait.
- Gepants and ditans. Limited lactation data — not first choice.
As a rule of thumb, if a drug is broadly acceptable in pregnancy it is usually acceptable in breastfeeding too, often more so because the baby's exposure through milk is typically smaller than across the placenta.
Key Research Papers
- Negro A, Delaruelle Z, Ivanova TA, et al. Headache and pregnancy: a systematic review. J Headache Pain. 2017;18(1):106.
- MacGregor EA. Migraine in pregnancy and lactation. Neurol Sci. 2014;35 Suppl 1:61–4.
- Amundsen S, Nordeng H, Nezvalová Henriksen K, et al. Pharmacological treatment of migraine during pregnancy and breastfeeding. Nat Rev Neurol. 2015;11(4):209–19.
- Bushnell CD, Jamison M, James AH. Migraines during pregnancy linked to stroke and vascular diseases: US population-based case-control study. BMJ. 2009;338:b664.
- Ferro JM, Canhão P. Cerebral venous sinus thrombosis (includes pregnancy/postpartum discussion). N Engl J Med. 2015.
- Tsou AY, Bulova P, Capone G, et al. Medical care of adults with Down syndrome: a clinical guideline. JAMA. 2020;324(15):1543–1554.
Live PubMed Searches
The following PubMed topic searches return current peer-reviewed work on migraine management across pregnancy, lactation, and the postpartum period:
- Migraine course in pregnancy and estrogen
- Sumatriptan pregnancy registry outcomes
- Topiramate and cleft lip/palate in pregnancy
- Valproate and neural tube defects
- Migraine with aura and stroke in pregnancy
- Preeclampsia headache and differential diagnosis
- Cerebral venous sinus thrombosis and postpartum
- NSAIDs in pregnancy and ductus arteriosus closure
- CGRP monoclonal antibodies in pregnancy
- Migraine medications in breastfeeding and LactMed
Connections
- Magnesium
- Preeclampsia
- Menstrual Migraine and Hormonal Triggers
- CGRP Inhibitors and Preventives
- Aura and Visual Disturbances
- Magnesium, Riboflavin, and Supplements
- Triptans and Gepants — Acute Treatment
- Migraine Overview
- Chronic Migraine and Medication Overuse
- Diet Triggers and Elimination Protocol
- Vestibular Migraine
- Perimenopause
- Stroke
- Headache
- Hypertension
- Vitamin B2 (Riboflavin)
- Magnesium Replenishment
- Sleep Hygiene