Myalgic Encephalomyelitis / Chronic Fatigue Syndrome (ME/CFS): An Under-Recognized Multi-System Disease
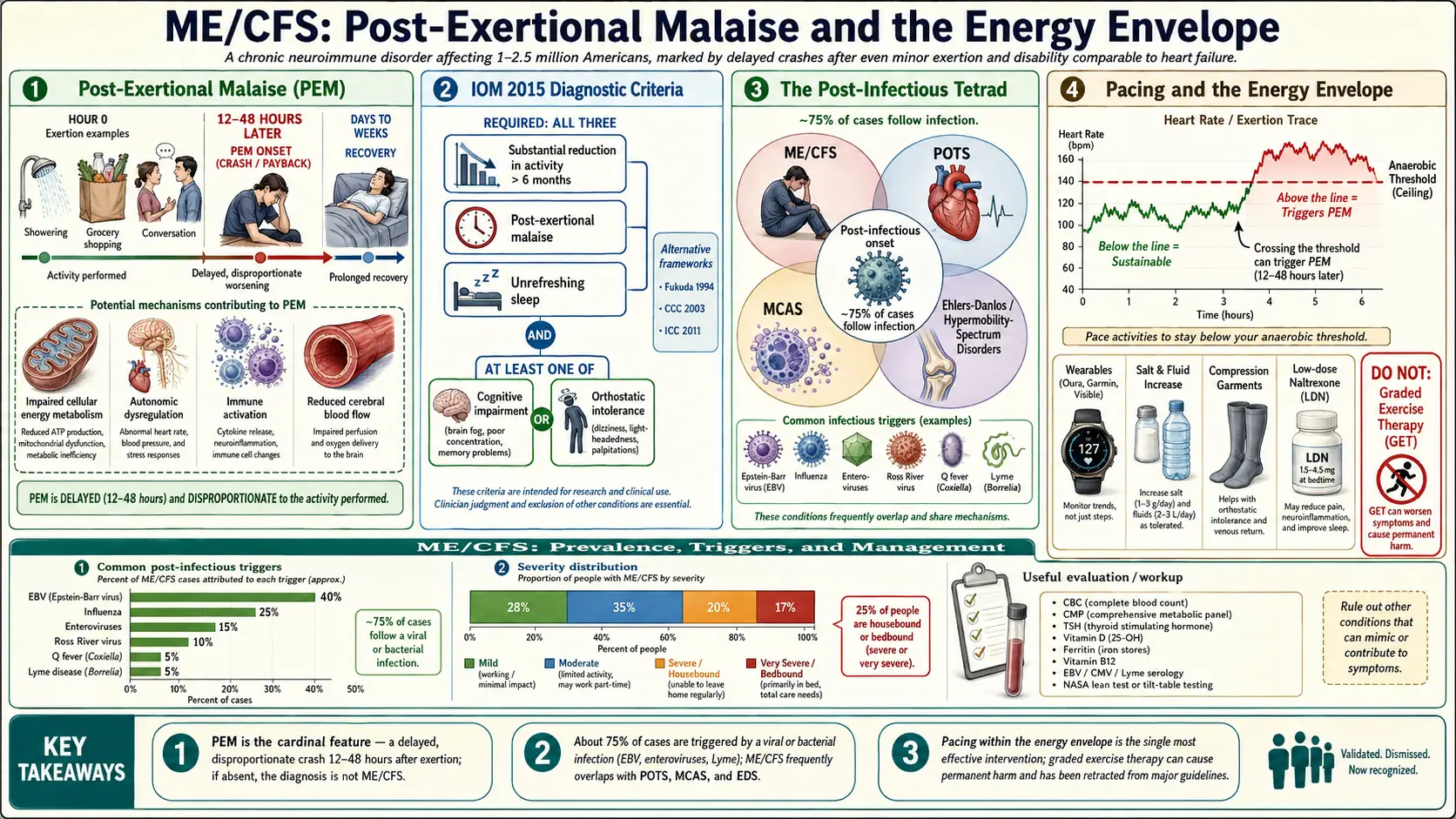
Myalgic encephalomyelitis / chronic fatigue syndrome (ME/CFS) is a serious, chronic, complex multi-system illness affecting an estimated 1 to 2.5 million Americans — likely many more given persistent diagnostic gaps. Its hallmark is post-exertional malaise (PEM), a dramatic worsening of symptoms after even minor physical, cognitive, or emotional exertion, lasting days to weeks and often completely disproportionate to the triggering activity. Unlike ordinary fatigue, ME/CFS is not relieved by rest, is often precipitated by a viral illness, and carries levels of functional disability comparable to heart failure or late-stage cancer.
This article covers diagnostic criteria, the critical distinction of PEM, common triggers, overlapping conditions, and the current management framework that prioritizes pacing above all.
What ME/CFS Is
ME/CFS is a neuroimmune disorder characterized by profound fatigue, post-exertional worsening, unrefreshing sleep, cognitive impairment (“brain fog”), and orthostatic intolerance, persisting for at least six months. It is distinguished from depression and from generic fatigue by the characteristic PEM response, which can be triggered by activities as modest as showering, grocery shopping, or holding a conversation.
Post-Exertional Malaise — The Cardinal Feature
PEM is a delayed, prolonged, disproportionate worsening of symptoms typically appearing 12–48 hours after exertion and lasting days to weeks. Patients describe it as “crashing” or “payback.” The pathophysiology appears to involve impaired cellular energy metabolism, autonomic dysregulation, immune activation, and altered cerebral blood flow — distinct mechanisms from deconditioning. Identifying PEM is the single most important diagnostic step; if it is absent, the diagnosis is something else.
Diagnostic Criteria
The 2015 IOM/NAM criteria require all three core symptoms:
- Substantial reduction or impairment in pre-illness activity levels, lasting >6 months, accompanied by fatigue that is often profound, not the result of ongoing exertion, and not substantially alleviated by rest.
- Post-exertional malaise.
- Unrefreshing sleep.
Plus at least one of:
- Cognitive impairment.
- Orthostatic intolerance.
Symptoms and Overlap
- Flu-like symptoms, tender lymph nodes, sore throat
- Headaches (often new or worse than previous pattern)
- Muscle and joint pain without swelling
- Temperature dysregulation
- Food and chemical sensitivities
- Gastrointestinal symptoms
- Dysautonomia (orthostatic tachycardia, palpitations, presyncope)
ME/CFS frequently overlaps with POTS, MCAS, Ehlers-Danlos/hypermobility spectrum disorders, and fibromyalgia — together sometimes called the “tetrad” of post-infectious/dysautonomic syndromes.
Triggers and Mechanisms
About 75 percent of cases follow an acute viral illness — mononucleosis (Epstein-Barr virus), influenza, enteroviruses, Ross River virus, Q fever, Lyme disease, and other infections. Long-term post-viral fatigue syndromes resemble ME/CFS closely. Proposed mechanisms include persistent immune activation, reduced natural-killer-cell function, autonomic dysregulation, mitochondrial dysfunction, reduced cerebral blood flow, and autoantibodies against autonomic receptors.
Workup
- CBC, CMP, CRP, ESR, TSH, free T4, cortisol, HbA1c, vitamin D, ferritin, B12.
- Celiac screen, iron studies.
- EBV, CMV, Lyme, babesia if indicated.
- Orthostatic vitals or a 10-minute stand test; tilt-table testing if POTS is suspected.
- Sleep study to exclude obstructive sleep apnea.
- Age-appropriate cancer screening.
Management — Pacing Above All
- Pacing. Staying strictly within one’s “energy envelope” to avoid triggering PEM. This is the single most effective intervention. Heart-rate monitoring during daily activities, typically staying under an anaerobic threshold calculated from baseline, helps patients pace objectively.
- Sleep hygiene and pharmacological sleep support where needed.
- Orthostatic intolerance. Increased salt and fluid, compression garments, midodrine, fludrocortisone, ivabradine where appropriate.
- Symptomatic pain management — low-dose naltrexone, duloxetine, amitriptyline, gabapentin where appropriate.
- Low-dose naltrexone (1.5–4.5 mg at bedtime) has multiple small trials showing symptom improvement.
- Cognitive load pacing — brain fog improves with reduced cognitive exertion, not pushing through.
- Nutrient repletion as indicated.
- Mental-health support for the adjustment and isolation of chronic illness (not as treatment of the underlying disease).
What to Avoid: Graded Exercise and CBT-as-Cure Framings
Historical recommendations of graded exercise therapy (GET) and CBT framed as curative have been retracted from U.K. NICE guidelines and by most expert bodies. GET can cause severe, sometimes permanent, harm in ME/CFS patients by repeatedly triggering PEM. CBT may help with coping but does not treat the underlying disease. These distinctions matter because many clinicians still recommend them.
Deep-Dive Articles
Post-Exertional Malaise (PEM) Explained
PEM is the cardinal feature that separates ME/CFS from ordinary fatigue. Delayed onset (24-72 h), disproportionate severity, prolonged recovery, and how to recognize it in yourself.
2-Day CPET & Objective Testing
The two-day cardiopulmonary exercise test is the gold standard for documenting PEM objectively. Where to get one (Workwell, Bateman Horne, Ithaca), cost, preparation, and disability use.
Pacing & Energy Envelope
Heart-rate pacing, anaerobic threshold, the envelope theory, wearables (Oura, Garmin, Visible), rest protocols, and why GET is harmful in ME/CFS.
IOM/SEID vs CCC vs ICC Criteria
Four competing diagnostic frameworks — Fukuda 1994, Canadian Consensus Criteria (CCC) 2003, International Consensus Criteria (ICC) 2011, IOM/SEID 2015. Which to use and why it matters.
Orthostatic Intolerance
POTS, neurally mediated hypotension, and orthostatic intolerance overlap with ME/CFS. Tilt testing, NASA lean test, salt/fluids/compression, and when medications help.
Post-Viral Triggers: EBV & Others
Epstein-Barr, HHV-6, enterovirus, giardia, and Lyme as common ME/CFS triggers. Testing (antibody panels, PCR), reactivation vs active infection, and antiviral considerations.
Severe & Very Severe ME
25% of ME/CFS patients are housebound or bedbound. Light/sound/touch sensitivity, tube feeding, home-care logistics, caregiver guidance, and the invisibility crisis.
LDN, Abilify & Experimental Therapies
Low-dose naltrexone, ultra-low-dose aripiprazole (Abilify), rituximab/cyclophosphamide trials, IVIG, and what early-phase research looks promising.
Mitochondrial Dysfunction & Energy Metabolism
The CPET data, ATP production failure, and evidence for CoQ10/carnitine/ribose.
Table of Contents
- Deep-Dive Articles
- What ME/CFS Is
- Post-Exertional Malaise — The Cardinal Feature
- Diagnostic Criteria
- Symptoms and Overlap
- Triggers and Mechanisms
- Workup
- Management — Pacing Above All
- What to Avoid: Graded Exercise and CBT-as-Cure Framings
- Research Papers
- Connections
- Featured Videos
Research Papers
Curated PubMed topic searches on ME/CFS (Chronic Fatigue Syndrome). Each link opens a live PubMed query so the result set stays current as new studies are indexed.
- PubMed topic search: Myalgic encephalomyelitis chronic fatigue syndrome
- PubMed topic search: ME/CFS IOM diagnostic criteria
- PubMed topic search: Post-exertional malaise
- PubMed topic search: CFS mitochondrial dysfunction
- PubMed topic search: ME/CFS cytokine inflammation
- PubMed topic search: CFS autonomic dysfunction
- PubMed topic search: Pacing ME/CFS
- PubMed topic search: Low-dose naltrexone ME/CFS
- PubMed topic search: Epstein-Barr virus chronic fatigue
- PubMed topic search: CFS two-day CPET
- PubMed topic search: ME/CFS prevalence epidemiology
- PubMed topic search: ME/CFS treatment review
Connections
- Mitochondria & ATP — interactive animation
- Post-Viral Triggers: EBV and Others
- Post-Exertional Malaise
- ME/CFS Diagnostic Criteria
- Severe and Very Severe ME
- 2-Day CPET and Objective Testing
- Orthostatic Intolerance in ME/CFS
- Pacing and the Energy Envelope
- LDN, Abilify and Experimental Therapies
- Mitochondrial Dysfunction and Energy Metabolism
- POTS
- MCAS
- Fibromyalgia
- Fatigue
- Brain Fog
- Low-Dose Naltrexone
- Lysine
- Magnesium
- Inflammatory Markers
- Mononucleosis