Headache
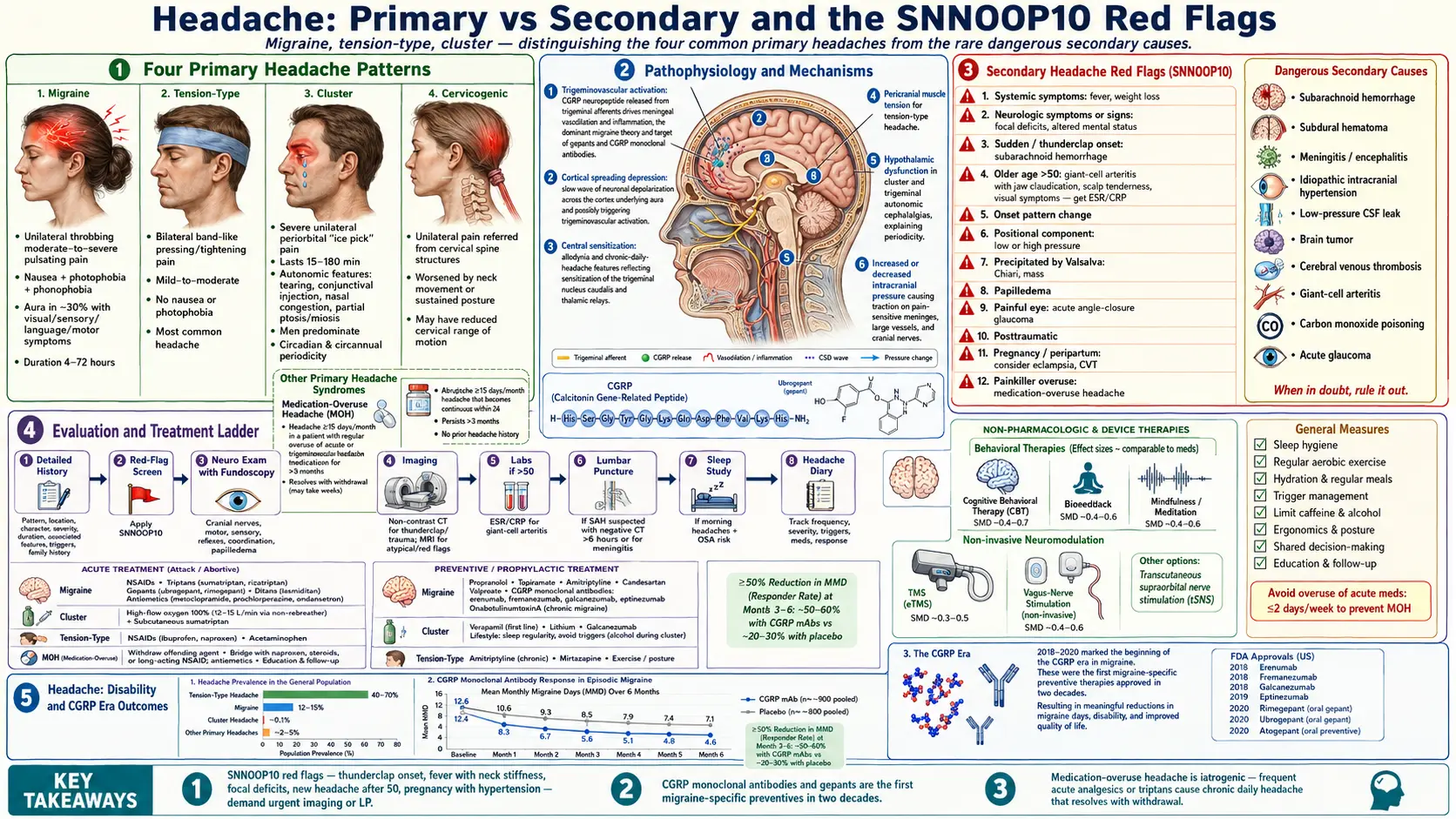

Table of Contents
- Overview
- Types of Headache
- Common Causes
- Mechanisms
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Headache is among the most common reasons people seek care worldwide. The first task in evaluation is to separate primary headache disorders — migraine, tension-type, cluster, and other trigeminal autonomic cephalalgias — from secondary headaches that signal an underlying disease such as hemorrhage, infection, raised intracranial pressure, or giant-cell arteritis. Most headaches are primary and treatable, but a careful history that screens for red-flag features keeps the rare dangerous causes from being missed.
Types of Headache
- Migraine — recurrent moderate-to-severe unilateral throbbing headaches, often with nausea, photophobia, phonophobia. About a third have aura (visual, sensory, language, or motor).
- Tension-type headache — bilateral, pressing or tightening, mild-to-moderate, without nausea or photophobia. The most common headache.
- Cluster headache — severe unilateral periorbital pain in attacks lasting 15 to 180 minutes, with autonomic features (tearing, conjunctival injection, nasal congestion). Predominates in men.
- Cervicogenic headache — pain referred from cervical spine structures, often unilateral, worsened by neck movement.
- Medication-overuse headache — chronic daily headache from frequent use of acute analgesics or triptans.
- Sinus headache — less common than commonly believed; most "sinus" headaches without infection are migraines with autonomic features.
- New daily persistent headache — sudden-onset daily headache that persists; often refractory.
- Post-traumatic headache — following concussion or head injury.
- Exertional, cough, and sex headaches — primary syndromes; require imaging at first presentation to exclude secondary causes.
Common Causes
- Primary headache predisposition — genetic; common across migraine, tension-type, and cluster.
- Triggers in migraine — sleep loss, missed meals, dehydration, alcohol, hormonal cycles, weather, stress, foods (chocolate, aged cheese, MSG, nitrates).
- Cervical spine disease — degenerative joint disease, whiplash, postural strain.
- Hypertension — severe or accelerated hypertension can cause headache; mild-to-moderate elevation usually does not.
- Medication-related — nitrates, dihydropyridine calcium-channel blockers, hormonal contraceptives, PDE5 inhibitors, and overuse of analgesics.
- Obstructive sleep apnea — morning headaches from CO2 retention.
- Caffeine withdrawal — in habitual users.
- Eye strain and refractive error — tension-type headache after prolonged screen use.
- Temporomandibular dysfunction — jaw and temple pain.
- Secondary causes — subarachnoid hemorrhage, subdural hematoma, meningitis or encephalitis, idiopathic intracranial hypertension, low-pressure (CSF leak) headache, brain tumor, cerebral venous thrombosis, giant-cell arteritis, carbon monoxide poisoning, acute glaucoma.
Mechanisms
- Trigeminovascular activation — the dominant theory in migraine; CGRP and other neuropeptides released from trigeminal afferents drive meningeal vasodilation and inflammation.
- Cortical spreading depression — a slow wave of neuronal depolarization underlies aura and may trigger trigeminovascular activation.
- Central sensitization — allodynia and chronic-daily-headache features reflect sensitization of trigeminal nucleus caudalis and thalamic relays.
- Pericranial muscle tension — contributes to tension-type headache, but not the sole driver; central pain modulation also matters.
- Hypothalamic dysfunction — central in cluster and other trigeminal autonomic cephalalgias; explains circadian and circannual periodicity.
- Increased or decreased intracranial pressure — raises or lowers traction on pain-sensitive structures (meninges, large vessels, cranial nerves).
Evaluation
- Detailed history — pattern (acute, recurrent, chronic), location, character, severity, duration, associated features, triggers, family history, medication and substance use.
- Red-flag screen (SNNOOP10) — systemic symptoms, neurologic symptoms, sudden onset, older age, pattern change, positional, precipitated by Valsalva, papilledema, painful eye, and posttraumatic.
- Neurologic exam — cranial nerves, motor and sensory function, coordination, gait, fundoscopy.
- Imaging — CT for thunderclap or trauma; MRI brain for atypical features, focal deficits, or red flags.
- ESR / CRP — in any new headache after age 50 to screen for giant-cell arteritis.
- Lumbar puncture — if subarachnoid hemorrhage is suspected and CT is negative within 6 hours, or for suspected meningitis.
- Sleep study — for morning headaches in patients with risk factors for OSA.
- Headache diary — the most useful longitudinal tool for identifying triggers, frequency, and response to therapy.
Management
- Migraine acute therapy — NSAIDs, triptans (sumatriptan, rizatriptan), gepants (ubrogepant, rimegepant), ditans (lasmiditan), antiemetics.
- Migraine preventives — propranolol, topiramate, amitriptyline, candesartan, valproate, CGRP monoclonal antibodies (erenumab, fremanezumab, galcanezumab, eptinezumab), botulinum toxin for chronic migraine.
- Tension-type headache — NSAIDs or acetaminophen for episodic; amitriptyline as preventive for chronic; physical therapy for cervicogenic component.
- Cluster headache — high-flow oxygen and subcutaneous sumatriptan for acute attacks; verapamil, lithium, galcanezumab for prevention.
- Medication-overuse headache — identify and withdraw the offending medication; cover the withdrawal phase with bridging therapy.
- Lifestyle and trigger management — consistent sleep, regular meals, hydration, exercise, stress reduction.
- Behavioral therapy — cognitive-behavioral therapy, biofeedback, mindfulness; effect sizes comparable to pharmacotherapy.
- Non-invasive neuromodulation — transcranial magnetic stimulation, vagus-nerve stimulation, supraorbital stimulation for selected migraine patients.
- Treat secondary causes — high-dose corticosteroids urgently for suspected giant-cell arteritis; neurosurgical referral for hemorrhage or mass; antibiotics for meningitis.
When to Seek Medical Care
- "Thunderclap" headache — maximum severity within seconds; rule out subarachnoid hemorrhage.
- Headache with fever and neck stiffness; rule out meningitis.
- Sudden severe headache with focal neurologic signs (weakness, numbness, vision change, slurred speech).
- New-onset headache in a person over 50, particularly with jaw claudication, scalp tenderness, or visual symptoms (rule out giant-cell arteritis).
- Progressive headache with morning vomiting, papilledema, or positional component.
- Headache in pregnancy with hypertension, vision change, or seizure.
- Headache with recent head injury or anticoagulation use.
- Immunocompromised patient with new headache.
- Cancer history with new headache pattern.
Connections
- Hypertension
- Obstructive Sleep Apnea
- Migraine
- Depression
- Magnesium
- Anxiety
- Brain Fog
- Chronic Pain
- Fatigue
- Meningitis
- Concussion
- MSG
- Insomnia
- Dizziness
- Stroke
- Nausea Vomiting
- Tick Borne Co Infections
- Malaria
References & Research
Historical Background
The systematic classification of headache disorders was established by the International Headache Society's first International Classification of Headache Disorders in 1988, now in its third edition (ICHD-3). The CGRP era, which began with the approval of the gepants and CGRP monoclonal antibodies between 2018 and 2020, transformed migraine treatment for the first time in two decades by offering preventives that work specifically on the migraine pathway rather than borrowing from cardiovascular and psychiatric pharmacopoeias.
Key Research Papers
- Headache Classification Committee of the International Headache Society. The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1-211.
- Ashina M, Katsarava Z, Do TP, et al. Migraine: epidemiology and systems of care. The Lancet. 2021;397(10283):1485-1495.
- Goadsby PJ, Reuter U, Hallstrom Y, et al. A controlled trial of erenumab for episodic migraine. New England Journal of Medicine. 2017;377(22):2123-2132.
- Lipton RB, Dodick DW, Ailani J, et al. Effect of ubrogepant vs placebo on pain and the most bothersome associated symptom in the acute treatment of migraine: the ACHIEVE II randomized clinical trial. JAMA. 2019;322(19):1887-1898.
- Loder E, Burch R, Rizzoli P. The 2012 AHS/AAN guidelines for prevention of episodic migraine: a summary and comparison with other recent clinical practice guidelines. Headache. 2012;52(6):930-945.
- May A, Schwedt TJ, Magis D, et al. Cluster headache. Nature Reviews Disease Primers. 2018;4:18006.
- Diener HC, Holle D, Solbach K, Gaul C. Medication-overuse headache: risk factors, pathophysiology and management. Nature Reviews Neurology. 2016;12(10):575-583.
- Tepper SJ, Diener HC, Ashina M, et al. Erenumab in chronic migraine with medication overuse: subgroup analysis of a randomized trial. Neurology. 2019;92(20):e2309-e2320.
- Charles A. The pathophysiology of migraine: implications for clinical management. Lancet Neurology. 2018;17(2):174-182.
- Do TP, Remmers A, Schytz HW, et al. Red and orange flags for secondary headaches in clinical practice: SNNOOP10 list. Neurology. 2019;92(3):134-144.
PubMed Topic Searches
- Migraine pathophysiology and CGRP
- Tension-type headache treatment
- Cluster headache treatment
- Medication-overuse headache
- SNNOOP10 secondary-headache red flags
- Giant-cell arteritis and headache