Triptans and Gepants for Acute Migraine Treatment
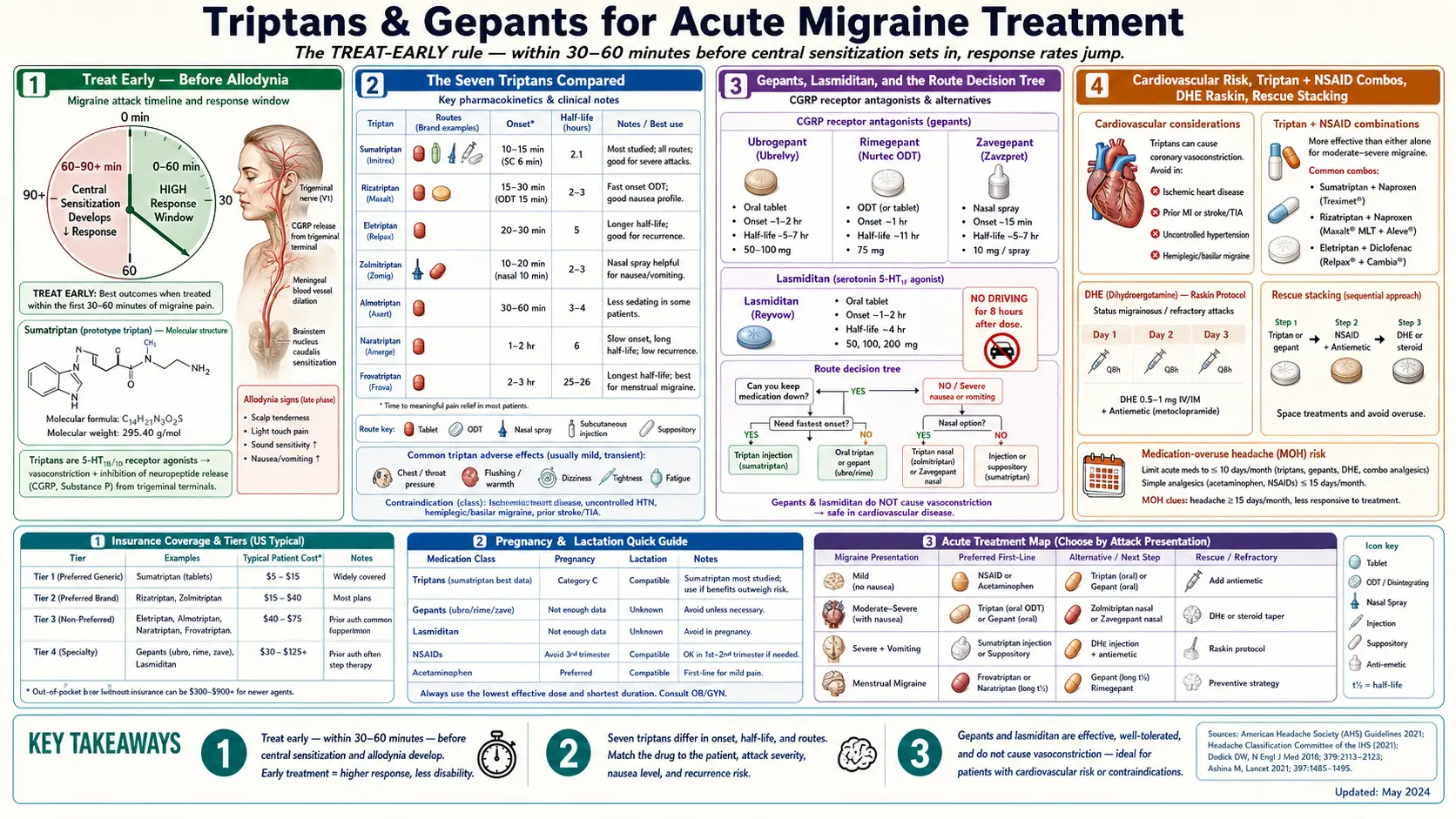
Table of Contents
- Abortive vs Prevention — What the Words Mean
- The Treat-Early Rule (Before Allodynia)
- The Seven Triptans Compared
- Oral vs Nasal vs Subcutaneous — A Decision Tree
- Triptan Non-Responders: Switch Before You Quit
- Gepants — The Newer Small Molecules
- Lasmiditan (Reyvow) — The Ditan
- If You Have Cardiovascular Risk
- Combos: Triptan + NSAID, and Anti-Emetics
- Ergotamines and DHE — Old Drugs, Still Useful
- Rescue Stacking When the First Dose Fails
- Pregnancy and Breastfeeding
- Insurance Tiering — The Reality
- Key Research Papers
- Connections
- Featured Videos
Abortive vs Prevention — What the Words Mean
Migraine care splits neatly into two buckets. Abortive (or "acute") medications are the ones you reach for when a migraine is starting or already hurting. Their job is to stop this attack. Preventive medications are taken every day whether you have a headache or not, and their job is to make future attacks less frequent, less severe, or less responsive to triggers. This article is about abortive treatment. The CGRP inhibitors and preventives page covers the other half.
The distinction matters because the drugs are different, the dosing rules are different, and the mistakes people make are different. Taking too much preventive does not cause medication-overuse headache; taking too much abortive does. Skipping a preventive for a day is almost harmless; skipping abortive treatment on an attack you could have stopped often means a wrecked 24 hours.
The Treat-Early Rule (Before Allodynia)
The single most important thing to know about abortive medication is this: it works dramatically better if you take it early. Within the first 30 to 60 minutes of pain, when the ache is still mild and you can still function, response rates for triptans and gepants run 60–70%. Wait two hours until the pain is moderate-to-severe, and response rates fall by roughly half.
The biological reason is a phenomenon called central sensitization. Early in an attack, the pain signal is driven by activated trigeminal nerves outside the brain — territory your medication can easily reach. After about 60 to 90 minutes, the signal moves inward and recruits the brain's own pain-processing neurons. You can usually tell when this has happened because a new symptom appears: cutaneous allodynia, where normal touch on the scalp, face, or even the skin where your glasses or ponytail sit becomes painful. Brushing your hair hurts. The pillow hurts. Once allodynia is present, triptans still work but less often, and even when they work, relief is slower and partial.
Practical translation: the moment you recognize this is a migraine — not a headache, not a sinus flare, not "maybe it'll pass" — take the medication. Carry it with you. Keep a dose in your car, your desk, your nightstand. The fear of "wasting" a dose on a headache that might have gone away on its own is misplaced; the cost of an untreated day is far higher than the cost of one extra tablet.
The Seven Triptans Compared
Triptans are 5-HT1B/1D receptor agonists. They constrict dilated cranial blood vessels, calm down the trigeminal nerve endings that release pain chemicals, and block pain signals at the brainstem. Seven are approved in the United States, and they are not interchangeable. Different triptans have different speeds of onset, different durations, different side-effect profiles, and different best-use cases.
- Sumatriptan (Imitrex) — the original, available in tablets (25/50/100 mg), nasal spray (5/20 mg), a new nasal powder (Onzetra Xsail), and subcutaneous injection (4/6 mg via autoinjector). Oral onset is 30–60 minutes. Injection onset is 10–15 minutes — the fastest abortive medication on the market. Half-life is 2 hours, which is short and means recurrence within the same day is common. Best for: people who need speed, people who vomit early and cannot keep tablets down, and people with predictable, self-limited attacks.
- Rizatriptan (Maxalt, Maxalt-MLT) — the MLT formulation is an orally disintegrating tablet (ODT) that melts on the tongue without water. Dose 5 or 10 mg. Onset 30 minutes. Half-life 2–3 hours. Has the highest 2-hour pain-free rates of any oral triptan in head-to-head meta-analyses. Best for: people who want the fastest-acting oral option, people with early nausea. Important: propranolol (common migraine preventive) raises rizatriptan levels, so the dose drops to 5 mg if you also take propranolol.
- Eletriptan (Relpax) — 20 or 40 mg tablet, onset 30–60 minutes, half-life 4–5 hours. One of the strongest oral triptans; good for severe attacks and lower recurrence because of the longer half-life. Best for: severe attacks, weekend migraines, anyone who failed rizatriptan.
- Zolmitriptan (Zomig, Zomig-ZMT nasal) — tablets 2.5/5 mg, ODT, and nasal spray 2.5/5 mg. The nasal spray reaches effective blood levels within 10–15 minutes, second only to injected sumatriptan for speed. Half-life 3 hours. Best for: fast escalation attacks, morning migraines where you wake up already hurting.
- Almotriptan (Axert) — 6.25/12.5 mg tablet. Similar efficacy to sumatriptan with notably fewer side effects (less chest pressure, less tingling). Half-life 3–4 hours. Best for: people who are bothered by triptan side effects but still need triptan efficacy.
- Naratriptan (Amerge) — 1 or 2.5 mg tablet. Slow onset (1–2 hours), long half-life (6 hours). Gentler, smoother, less recurrence. Best for: slower-building attacks, menstrual migraines where the attack lasts 2–3 days and you need sustained coverage. See the menstrual migraine page for mini-prophylaxis protocols using naratriptan or frovatriptan.
- Frovatriptan (Frova) — 2.5 mg tablet, the longest half-life of any triptan at 26 hours. Slow onset makes it a poor choice for a rapidly escalating attack, but the long tail makes it the standard agent for menstrual-migraine mini-prevention — dosed twice daily for 5 to 6 days around the expected attack window.
If one triptan does not work, a different triptan often will. Roughly 30–40% of people who fail their first triptan respond to a second. The American Headache Society recommends trying at least two or three different triptans, at adequate doses and taken early, before concluding that triptans as a class do not work for you.
Oral vs Nasal vs Subcutaneous — A Decision Tree
Route of delivery matters as much as which molecule. Use this rough decision tree:
- Mild to moderate pain, no nausea, attack builds slowly. Start with an oral tablet or ODT (rizatriptan MLT, eletriptan, almotriptan). Cheapest, easiest, works fine when taken early.
- Pain already moderate-severe, or attack escalates fast. Use a nasal spray (zolmitriptan nasal, sumatriptan nasal, or the newer zavegepant gepant). Onset is 10–30 minutes; you bypass a gut that may be slowed by migraine-related gastroparesis.
- Vomiting, or can't keep tablets down. Injection (sumatriptan SC autoinjector) or nasal. Oral is pointless if you throw it up.
- Wake up with severe migraine already in progress. Injection or nasal. Do not start with a tablet; you are already past the window where oral works well.
- Infrequent but devastating attacks (e.g. 1–2 per month, each lasting all day). Keep sumatriptan SC autoinjectors in reserve. Expensive per dose, but a single injection can save an entire workday.
One gut-truth worth saying out loud: migraine slows gastric emptying (this is why nausea is so common). That means oral tablets sit in the stomach longer than usual and absorb later and less completely. The sicker you already are, the more a non-oral route makes sense.
Triptan Non-Responders: Switch Before You Quit
Perhaps 30–40% of migraine patients are labelled "triptan non-responders" at some point. The label is almost always premature. Before accepting it, make sure all of the following are true:
- You took the medication within 30–60 minutes of pain onset, not hours later.
- You used an adequate dose (sumatriptan 100 mg, not 25; rizatriptan 10 mg, not 5 unless you are on propranolol).
- You tried at least two different triptans, ideally three, on separate attacks.
- You tried a non-oral route at least once (nasal or subcutaneous).
- You combined a triptan with an NSAID at least once (see combos below).
If all five boxes are checked and you still get less than 50% pain relief within two hours on most attacks, then triptans probably are not your drug. This is exactly where gepants and lasmiditan become useful.
Gepants — The Newer Small Molecules
Gepants are small-molecule CGRP receptor antagonists. Instead of squeezing blood vessels like triptans, they block the calcitonin gene-related peptide receptor that drives migraine pain at the trigeminal nerve. They do not cause vasoconstriction, which makes them safe for people with cardiovascular disease. Three are FDA-approved for acute treatment:
- Ubrogepant (Ubrelvy) — 50 or 100 mg tablet. Onset around 1–2 hours. Can repeat the dose once after 2 hours. 2-hour pain-freedom rate around 20% in pivotal trials (placebo 12%) — smaller than triptans, but no vasoconstriction and no risk of medication-overuse headache in the typical sense. The Lipton 2019 ACHIEVE II trial established this drug.
- Rimegepant (Nurtec ODT) — 75 mg orally disintegrating tablet. Unique among abortives because it is also approved for prevention (taken every other day). Onset 1–2 hours for acute use. 2-hour pain-free rate around 21% vs 11% placebo in Croop's 2019 trial. The every-other-day dual use is attractive for people with frequent migraines who want a single drug to cover both roles.
- Zavegepant (Zavzpret) — 10 mg nasal spray, approved 2023. Onset as early as 15 minutes, similar to nasal triptans. The first non-triptan, non-ergot abortive with a true fast-acting route. Best for: fast-escalating attacks in cardiovascular-risk patients, or triptan failures who need speed.
Gepants are slower and somewhat weaker than a well-matched triptan in head-to-head contexts, but they have two killer features. First, they are not vasoconstrictors, so they are usable in people who cannot take triptans (coronary disease, stroke history, uncontrolled hypertension). Second, they do not appear to cause medication-overuse headache the way triptans, opioids, and barbiturates do — see the medication-overuse article.
Lasmiditan (Reyvow) — The Ditan
Lasmiditan is a 5-HT1F receptor agonist. Triptans hit 5-HT1B (vessels), 5-HT1D (nerves), and 5-HT1F (central). Lasmiditan hits only 1F, so it has no vasoconstrictor activity. Doses are 50, 100, or 200 mg oral tablets. 2-hour pain-free rates around 28–32% at 200 mg (Kuca SPARTAN trial 2018). It works.
The catch: lasmiditan crosses the blood-brain barrier and can cause dizziness, sedation, and impaired attention. The FDA requires an 8-hour no-driving window after any dose. For many working-age patients this is a deal-breaker. But for a weekend migraine, an evening attack, or a patient where triptans are contraindicated and gepants are too slow, lasmiditan fills a genuine gap.
If You Have Cardiovascular Risk
Triptans and ergots constrict blood vessels, including coronary arteries. They are contraindicated in anyone with:
- Coronary artery disease or a history of myocardial infarction
- Stroke or transient ischemic attack
- Peripheral artery disease
- Uncontrolled hypertension
- Hemiplegic or basilar migraine (older labels; some guidelines now allow cautious use)
- Pregnancy in most cases (see below)
For these patients, the acute-treatment shortlist is: gepants (rimegepant, ubrogepant, zavegepant), lasmiditan, NSAIDs if kidneys tolerate them, and anti-emetic adjuncts. This is one of the most consequential developments in migraine care in a generation — before 2019, a 60-year-old with coronary disease and severe migraine often had nothing. Now they have three gepants and a ditan.
Combos: Triptan + NSAID, and Anti-Emetics
Adding an NSAID to a triptan increases response rates by roughly 10–15 percentage points, reduces recurrence, and extends coverage. The FDA-approved combination is Treximet (sumatriptan 85 mg + naproxen 500 mg) in a single tablet, but you can build the same effect by taking your triptan plus naproxen 500 mg or ibuprofen 600–800 mg separately.
Anti-emetics earn their keep too. Migraine-related gastroparesis slows every oral absorbtion; an anti-emetic speeds gastric emptying and blunts nausea simultaneously. Two workhorses:
- Metoclopramide (Reglan) 10 mg oral or IV — pro-kinetic and anti-nauseant, works within 30 minutes. Watch for akathisia (inner restlessness) and, over the long term, tardive dyskinesia with chronic use.
- Prochlorperazine (Compazine) 10 mg oral, IM, or IV — actually reduces migraine pain on its own, beyond the anti-nausea effect. Heavy-hitter for ER use.
- Ondansetron (Zofran) — excellent anti-nausea but does not speed gastric emptying and does not reduce pain.
Ergotamines and DHE — Old Drugs, Still Useful
Dihydroergotamine (DHE) predates triptans and still has specialized roles. It is a non-selective serotonin receptor agonist, longer-acting and less likely to give rebound than triptans. Available as nasal spray (Migranal, Trudhesa) and as IV infusion. The IV protocol — the Raskin protocol, typically 0.5–1 mg IV every 8 hours combined with metoclopramide for three days — is a standard rescue for status migrainosus (a migraine that has lasted more than 72 hours) and for breaking a medication-overuse cycle. Many headache clinics operate "infusion clinics" that deliver this on an outpatient basis.
Contraindications overlap with triptans and are somewhat stricter: no coronary disease, no stroke, no uncontrolled hypertension, no pregnancy, and do not combine with a triptan within 24 hours (both vasoconstrict).
Rescue Stacking When the First Dose Fails
A working rescue ladder for a bad attack looks something like this, modified to your personal contraindications:
- At first recognition: oral triptan (or gepant) + naproxen 500 mg + an anti-emetic such as metoclopramide 10 mg. Drink water.
- At 2 hours if still hurting: second dose of the triptan (check max daily dose) or switch to the nasal/SC route.
- At 4 hours if still hurting: add a gepant (rimegepant or ubrogepant) — different mechanism, stackable with a triptan that is already wearing off. Add a dose of prochlorperazine if you have it.
- At 6–8 hours if status migrainosus: DHE nasal spray if prescribed; otherwise consider an urgent care or ER visit for IV fluids, IV ketorolac, IV metoclopramide or prochlorperazine, and possibly IV DHE or IV magnesium.
- Red flags to go straight to the ER: "worst headache of my life," thunderclap onset, new neurological deficit, fever and stiff neck, head trauma, or a migraine that feels different from your usual pattern.
Stacking drugs is safer than it sounds as long as you respect the rules: do not combine a triptan with DHE within 24 hours, do not exceed the daily max of any one class, and do not use any abortive on more than 10–15 days per month averaged over a few months — that is the territory of medication-overuse headache.
Pregnancy and Breastfeeding
Migraines often improve during pregnancy, especially the second and third trimesters, but not always. The acute-treatment options shrink:
- First-line: acetaminophen, sometimes with metoclopramide. Non-drug measures — ice packs, dark room, hydration, sleep — matter more than usual.
- Second-line: sumatriptan has the largest pregnancy exposure registry of any triptan and has not been linked to major malformations, though data are not definitive. Many headache specialists will permit sumatriptan in pregnancy after discussion when attacks are disabling. Ergots and DHE are contraindicated. Gepants have little human pregnancy data and are generally avoided.
- NSAIDs: avoid in the third trimester (premature closure of the fetal ductus arteriosus); generally avoided throughout pregnancy if possible.
- Breastfeeding: sumatriptan and eletriptan have the lowest milk transfer and are generally considered compatible. Ibuprofen and acetaminophen are compatible.
Pregnancy-specific decisions should always involve your obstetrician and ideally a headache specialist. The risk calculus changes trimester by trimester.
Insurance Tiering — The Reality
In the U.S., generic triptans (sumatriptan tablets, rizatriptan, zolmitriptan, naratriptan, almotriptan) are cheap — often under $20 per month with a discount card. Brand-name formulations (Zomig nasal, Onzetra, Treximet, Imitrex SC autoinjectors) are not. Gepants, lasmiditan, and the newer nasal gepant cost $800–$1000 per month at retail and sit on insurance tiers 3 or 4. Practical tactics:
- Prior authorization is almost always required for gepants and lasmiditan. Insurers typically require documented failure of two triptans first. Document those failures in your chart.
- Manufacturer copay cards can bring Nurtec, Ubrelvy, Qulipta, and Reyvow down to $0–$10 per prescription for commercially insured patients. They do not apply to Medicare or Medicaid.
- Quantity limits are aggressive: 8 gepant tablets per month is common, 9 triptan tablets per month is common. If you have more than 8 migraines a month, you also need preventive therapy.
- Sumatriptan autoinjectors (generic) are often covered but limited to 2 per month; ask for a "needle-free" or prefilled-syringe alternative if the autoinjector is denied.
The hard truth: if you use more than 8–10 doses per month of any acute agent, you are in preventive-therapy territory. Preventives — CGRP monoclonal antibodies, gepants dosed every other day, beta blockers, topiramate, Botox for chronic migraine — reduce attack frequency so acute doses become affordable again. See the preventives page for the other half of the strategy.
Key Research Papers
- Ferrari MD, Roon KI, Lipton RB, Goadsby PJ. Oral triptans (serotonin 5-HT1B/1D agonists) in acute migraine treatment: a meta-analysis of 53 trials. Lancet. 2001.
- Lipton RB, Dodick DW, Ailani J, et al. Effect of ubrogepant vs placebo on pain and the most bothersome associated symptom in the acute treatment of migraine: the ACHIEVE II randomized clinical trial. N Engl J Med. 2019.
- Croop R, Goadsby PJ, Stock DA, et al. Efficacy, safety, and tolerability of rimegepant orally disintegrating tablet for the acute treatment of migraine. Lancet. 2019.
- Kuca B, Silberstein SD, Wietecha L, et al. Lasmiditan is an effective acute treatment for migraine: a phase 3 randomized study (SPARTAN). Neurology. 2018.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on acute migraine pharmacology and clinical practice:
- Triptans in acute migraine — meta-analyses
- Gepants, ubrogepant, and rimegepant for migraine
- Zavegepant nasal spray for acute migraine
- Lasmiditan and the 5-HT1F pathway
- Cutaneous allodynia and triptan response
- Sumatriptan-naproxen combination therapy
- Dihydroergotamine for status migrainosus
- Triptan cardiovascular safety
- Sumatriptan pregnancy exposure registry
Connections
- CGRP Inhibitors and Preventives
- Chronic Migraine and Medication Overuse
- Menstrual Migraine and Hormonal Triggers
- Migraine Overview
- Magnesium, Riboflavin, and Supplements
- Diet Triggers and Elimination Protocol
- Vestibular Migraine
- Aura and Visual Disturbances
- Mast Cell Activation Syndrome
- POTS
- Chronic Pain
- Headache
- Stroke
- Hypertension
- Magnesium
- Migraine in Pregnancy and Breastfeeding
- Chronic Fatigue Syndrome
- Vertigo and Meniere's Disease