Chronic Migraine and Medication Overuse Headache
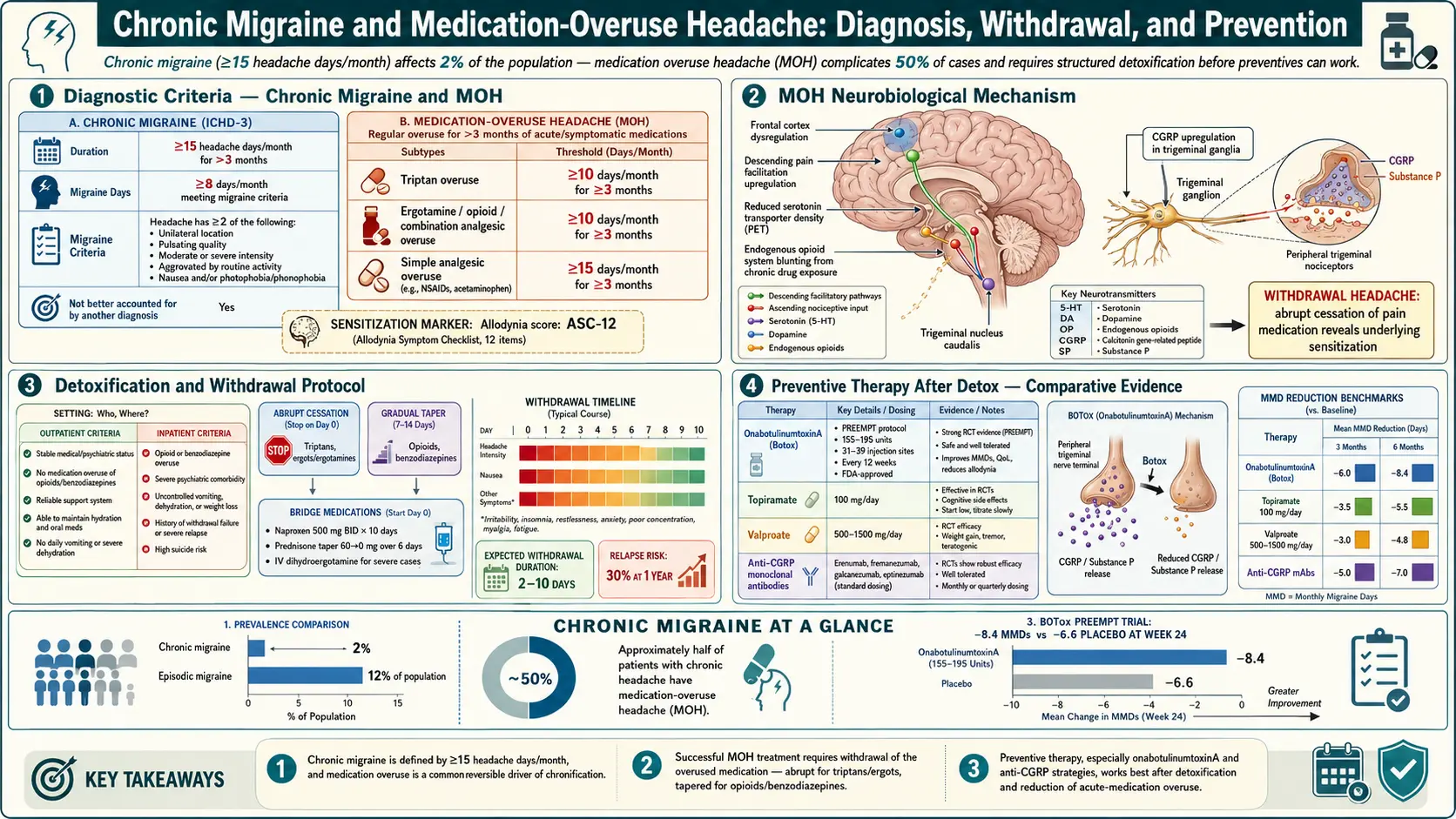
Table of Contents
- Episodic vs Chronic — The ICHD-3 Definitions
- How Episodic Becomes Chronic
- Medication Overuse Headache — The Thresholds
- Why Opioids and Butalbital Are the Worst Offenders
- What MOH Does to the Brain
- Withdrawal — Cold Turkey vs Taper
- Bridge Therapy During Detox
- Inpatient vs Outpatient Detox
- Botox (OnabotulinumtoxinA) — The PREEMPT Protocol
- CGRP Antibodies for Chronic Migraine
- Neuromodulation Devices
- Nerve Blocks
- Lifestyle Stabilization as Foundation
- How to Track: Diaries and Apps
- What Recovery Looks Like
- When to Pursue Disability
- Key Research Papers
- Connections
- Featured Videos
Episodic vs Chronic — The ICHD-3 Definitions
The International Classification of Headache Disorders, third edition (ICHD-3) — the rulebook neurologists use — draws a sharp line between episodic and chronic migraine. The line is drawn at 15 headache days per month.
- Episodic migraine: fewer than 15 headache days per month.
- Chronic migraine: headache on 15 or more days per month for at least 3 months, of which at least 8 days per month meet full migraine criteria (or respond to a triptan or ergot).
Those "8 migraine days" matter. Many people with chronic migraine have a mix — some days the headache is a full migraine attack with nausea, light sensitivity, and throbbing unilateral pain; other days it is a lower-grade "tension-type" ache that still keeps them from functioning. ICHD-3 counts all of those days toward the 15, as long as at least 8 have migraine features.
The diagnostic label matters because it unlocks treatments. Botox, for example, is FDA-approved only for chronic migraine — not for episodic. Many insurers demand documented chronic migraine (15+ days/month) before paying for CGRP injections, Botox, or neuromodulation devices. The diary you keep at home is the evidence that gets you access to the treatment you need.
How Episodic Becomes Chronic
Roughly 2.5% of episodic migraine patients progress to chronic migraine every year — a finding from the American Migraine Prevalence and Prevention (AMPP) study led by Marcelo Bigal and Richard Lipton. That is not a huge absolute number, but across a long disease course it adds up: someone with migraine since their twenties has a meaningful probability of crossing into chronic territory by midlife if risk factors stack.
The strongest modifiable risk factors for chronification:
- High baseline attack frequency (already 10–14 days/month — one step below the threshold).
- Medication overuse — especially opioids, butalbital-containing combinations, and triptans used on more than 10 days/month.
- Obesity (BMI over 30 roughly doubles the risk).
- Untreated sleep apnea and poor sleep generally.
- Depression and anxiety — bidirectional; each makes the other worse.
- Persistent stressors (work, caregiving, financial strain).
- Cutaneous allodynia — when your scalp or face becomes tender during attacks, it is a sign that central sensitization has already begun.
The good news, buried in the same epidemiology: patients can "re-convert" from chronic back to episodic. Removing the overused medication is the single highest-yield intervention. Anywhere from 45% to 70% of chronic migraine sufferers who also overuse analgesics will drop below 15 headache days per month within two to six months of detox — often without adding any new drug.
Medication Overuse Headache — The Thresholds
Medication overuse headache (MOH) is a specific ICHD-3 diagnosis in its own right. It is defined as headache on 15 or more days per month in a person with a pre-existing headache disorder, caused by regular overuse of acute or symptomatic headache medication for more than 3 months. The thresholds, memorize these:
- Triptans (sumatriptan, rizatriptan, etc.) — 10 or more days per month.
- Ergots (ergotamine, dihydroergotamine oral/nasal) — 10 or more days per month.
- Opioids (codeine, tramadol, hydrocodone, oxycodone) — 10 or more days per month.
- Butalbital combinations (Fioricet, Fiorinal) — 10 or more days per month, and many specialists argue even 5 days is too many.
- Combination analgesics (Excedrin Migraine, anything with caffeine + acetaminophen + aspirin) — 10 or more days per month.
- Simple analgesics used alone (plain acetaminophen, plain ibuprofen, plain naproxen, plain aspirin) — 15 or more days per month.
Two traps catch most patients. First, these thresholds are per month, every month, for three months. A bad week does not cause MOH — a bad pattern does. Second, people routinely underestimate their use because they grab "just one" on dozens of workdays. A headache diary tends to reveal usage double what the patient quoted from memory.
The gepants — ubrogepant (Ubrelvy), rimegepant (Nurtec) — appear to not cause MOH in the same way, and rimegepant is actually approved for both acute and preventive use. This is one of the most clinically important differences between the triptan era and the gepant era, and it is why neurologists increasingly steer patients with frequent attacks toward gepants.
Why Opioids and Butalbital Are the Worst Offenders
All acute migraine medications can cause MOH if overused, but they are not equally bad. The risk hierarchy, from worst to least bad:
- Opioids. Cause MOH faster than any other class and are associated with the highest rate of progression from episodic to chronic migraine. Opioids also sensitize pain pathways systemically, worsen sleep, and offer minimal benefit for most migraine attacks. No current migraine guideline recommends opioids for routine migraine care.
- Butalbital combinations (Fioricet, Fiorinal). Butalbital is a barbiturate with addiction potential, strong rebound, and nasty withdrawal (anxiety, insomnia, seizures at high doses). These should essentially not be prescribed for migraine anymore; they remain on the market largely because patients on them for years cannot easily stop.
- Combination analgesics with caffeine (Excedrin Migraine). Caffeine is itself a headache driver in overuse. Many MOH cases are driven by daily Excedrin plus daily coffee.
- Triptans. Effective drugs that cause MOH at a well-defined threshold (10 days/month). Most patients do fine staying under the limit.
- Plain NSAIDs and acetaminophen. Cause MOH too, but the threshold is higher (15 days/month), and they are the safest of the commonly used classes from an MOH standpoint.
If you are currently on daily opioids or butalbital for migraine, the single most important conversation you can have with your neurologist is how to get off them. This is not about blame or addiction stigma — it is about physiology. These drugs make the underlying brain disorder worse the longer they are used.
What MOH Does to the Brain
In plain language: the brain adapts to whatever you feed it daily. Feed it triptans every day and the serotonin receptors those drugs target downregulate — there are fewer of them, and they respond less vigorously. Feed it opioids every day and the mu-opioid system rewires, amplifying pain input instead of dampening it (opioid-induced hyperalgesia). Feed it caffeine-containing combination pills every day and caffeine withdrawal headaches start between doses.
Underneath all of this sits the trigeminovascular system — the nerve network that carries migraine pain from meningeal blood vessels through the trigeminal nerve into the brainstem and up into the thalamus. In MOH, this system becomes hyper-responsive. Animal studies show that repeated triptan or opioid exposure produces central sensitization: the threshold for triggering a headache drops, and normal stimuli (a skipped meal, a noisy room, a weather front) that would once have passed without incident now reliably set off attacks.
The upshot is that you cannot reason or willpower your way out of MOH. The brain has been rewired by the medication, and the only reliable way to un-wire it is to stop the medication and let the system normalize. That takes weeks, not days, and feels awful in the middle.
Withdrawal — Cold Turkey vs Taper
"Detox" in headache medicine means stopping the overused acute medication. There are two approaches, and your class of drug dictates which is safe.
Cold turkey is standard for triptans, ergots, NSAIDs, acetaminophen, and combination analgesics like Excedrin. You pick a start date and stop on that date. The first 2 weeks are typically the worst — headache intensifies, nausea worsens, sleep suffers. By week 3 or 4, most patients begin to see daylight. By week 8, headache days have usually dropped substantially.
Structured taper is mandatory for opioids (physiologic dependence, autonomic withdrawal) and butalbital (risk of seizures if stopped abruptly after long-term high-dose use). A typical butalbital taper cuts the dose by 10–25% every one to two weeks under physician supervision. Opioid tapers follow the same slow principle and sometimes benefit from adjunct clonidine or buprenorphine bridging.
The rebound period — the stretch where headaches worsen before they improve — generally runs 2 to 8 weeks. Most patients who will benefit from detox see their headache days drop by week 8. Some take up to 12 weeks. Knowing that the worst part is time-limited is the single most important piece of information going in.
Bridge Therapy During Detox
"Bridge therapy" means short-term treatments used only during the detox window to blunt the rebound. These are not daily forever-medications — they are training wheels that come off after 1–4 weeks. Common options:
- Scheduled naproxen 500 mg twice daily for 2–4 weeks. Safe, cheap, and surprisingly effective. NSAIDs do not cause MOH as readily as triptans or opioids, and scheduled dosing (rather than as-needed panic use) is part of what breaks the overuse cycle.
- Prednisone taper — 60 mg daily for 3 days, then 40 mg for 3 days, then 20 mg for 3 days. Short oral steroid bursts can interrupt the status-migrainosus pattern that often erupts at the start of detox.
- IV dihydroergotamine (DHE) — the Raskin protocol, originally developed at Cornell, uses IV DHE every 8 hours for 3–5 days, often in an outpatient infusion suite or brief hospital stay. This remains one of the most effective bridges for severe MOH.
- Occipital and sphenopalatine ganglion nerve blocks (see below) performed at the start of detox.
- IV magnesium sulfate 1–2 grams infused over 30–60 minutes — cheap, safe, and sometimes dramatically helpful, particularly in patients who are also magnesium-deficient on serum testing.
- IV valproate (Depacon) 500–1000 mg infused over an hour, repeated once or twice. Useful for intractable rebound days but avoided in pregnancy.
Starting a preventive at the same time as detox is standard practice — topiramate, a beta-blocker, amitriptyline, a CGRP antibody, or Botox all work better once the brain is no longer being overwhelmed by the overused medication.
Inpatient vs Outpatient Detox
Most MOH detox happens outpatient. A typical outpatient plan: stop the overused drug on day zero, start a preventive, run a bridge (often scheduled naproxen plus a prednisone taper), and schedule follow-up at 2, 4, and 8 weeks. This works for the majority.
Inpatient detox — usually a 3 to 5 day admission to a headache specialty unit — is reserved for:
- Long-term opioid or butalbital dependence with meaningful withdrawal risk.
- Failed outpatient detox attempts (often multiple).
- Severe comorbid depression or suicidality.
- Intractable status migrainosus unresponsive to outpatient bridge.
- Need for aggressive IV therapy (IV DHE Raskin protocol with cardiac monitoring).
A handful of U.S. centers run dedicated inpatient headache programs — the Jefferson Headache Center (Philadelphia), Michigan Head Pain and Neurological Institute, Mayo Clinic, and Diamond Headache Clinic are the best known. Insurance coverage varies and often requires prior authorization with documentation of failed outpatient attempts.
Botox (OnabotulinumtoxinA) — The PREEMPT Protocol
Botox was FDA-approved for chronic migraine in 2010 on the strength of the two PREEMPT trials. The protocol is precise and worth understanding — your injections should match it.
- Total dose: 155 units of onabotulinumtoxinA.
- Number of injection sites: 31, spread across seven muscle groups.
- Dose per site: 5 units.
- Muscle groups:
- Corrugator (2 sites, forehead above eyebrows)
- Procerus (1 site, bridge of nose)
- Frontalis (4 sites, forehead)
- Temporalis (8 sites, temples)
- Occipitalis (6 sites, back of head)
- Cervical paraspinal (4 sites, upper neck)
- Trapezius (6 sites, shoulders)
- Interval: every 12 weeks.
The two PREEMPT trials (Aurora 2010, Diener 2010) each enrolled around 700 chronic migraine patients. Both showed about 8–9 fewer headache days per month after 24 weeks of treatment compared to baseline, with Botox superior to placebo on several endpoints. Full response usually takes two or three cycles; do not judge Botox on a single round.
Practical points. Botox for migraine must be delivered by someone trained in the PREEMPT protocol — most often a headache-specialist neurologist, not a cosmetic injector. Insurance typically requires documented chronic migraine (15+ days/month) plus failure of two or three oral preventives. The injections take about 15 minutes and feel like a series of bee stings. Mild neck soreness is common for a day or two. Eyelid or eyebrow droop is rare when the protocol is followed correctly.
CGRP Antibodies for Chronic Migraine
All four monoclonal antibodies targeting the calcitonin-gene-related peptide (CGRP) pathway are approved for chronic migraine. They are the first preventive class developed specifically for migraine rather than borrowed from other specialties.
- Erenumab (Aimovig) — 70 mg or 140 mg subcutaneous injection monthly. Blocks the CGRP receptor.
- Fremanezumab (Ajovy) — 225 mg monthly or 675 mg quarterly. Binds the CGRP ligand.
- Galcanezumab (Emgality) — 240 mg loading dose, then 120 mg monthly.
- Eptinezumab (Vyepti) — 100 or 300 mg IV infusion every 3 months.
Expected benefit in chronic migraine trials: about 4 to 7 fewer migraine days per month, with 30–40% of patients achieving 50% or better reduction. Side-effect profile is remarkably clean — injection-site reactions, constipation (particularly with erenumab), and occasional blood pressure elevation are the main concerns. Unlike topiramate, they do not cause cognitive fog or weight loss. Unlike amitriptyline, they do not cause sedation. Unlike Botox, they work on their own schedule without 31 needles every 12 weeks. See the CGRP inhibitors deep-dive for the full comparison.
Importantly, CGRP antibodies work even in the presence of ongoing medication overuse — trial data and real-world cohorts show benefit before full detox is achieved. This has changed practice: many clinicians now start a CGRP monoclonal on day zero of detox, making the rebound period more bearable and improving the odds of success.
Neuromodulation Devices
Four wearable devices are FDA-cleared for migraine, and all can be useful in chronic migraine and MOH where drug options are limited or maxed out:
- Cefaly — a supraorbital TENS-style device worn as a forehead band. Daily 20-minute preventive sessions plus 60-minute acute sessions. Non-prescription.
- Nerivio — a remote electrical neuromodulation (REN) armband controlled via smartphone app. Delivers 45-minute conditioned-pain-modulation sessions during attacks. Also approved for chronic migraine prevention with every-other-day use.
- gammaCore — a non-invasive vagus nerve stimulator applied to the side of the neck. Both acute and preventive use.
- SAVI Dual (sTMS mini) — single-pulse transcranial magnetic stimulation held to the back of the head. Acute and preventive use, including in adolescents.
Effect sizes are modest compared with Botox or CGRP antibodies, but the devices have almost no systemic side effects, which makes them particularly attractive for patients who cannot tolerate medications, who are pregnant, or who are in the middle of MOH detox and want a non-drug option to reach for instead of another pill.
Nerve Blocks
Two office-based nerve-block procedures are standard in chronic migraine:
- Greater and lesser occipital nerve blocks — a small injection of lidocaine (sometimes with a steroid) at the back of the head, where the occipital nerves emerge. Takes 5 minutes, numbs the scalp, and can abort status migrainosus or reduce headache days for weeks afterward. Often used at the start of detox.
- Sphenopalatine ganglion (SPG) block — lidocaine delivered via a thin intranasal catheter (Tx360 or SphenoCath device) to a nerve cluster behind the nasal cavity. Useful as a bridge therapy and for cluster headache. Non-invasive and repeatable.
Both are typically covered by insurance when performed by a headache specialist or pain physician, and both are drug-free alternatives for patients who cannot take more systemic medication.
Lifestyle Stabilization as Foundation
Every patient hates the "sleep, eat, hydrate, exercise" lecture, and every headache specialist gives it anyway because it works. In chronic migraine, the brain is already hypersensitive. Variation in sleep, meals, caffeine, or stress lands harder than it would on an episodic brain. The non-negotiable foundation:
- Sleep: same bedtime and wake time every day, including weekends. Screen for sleep apnea if you snore, are overweight, or wake unrefreshed.
- Meals: do not skip. Blood sugar drops are potent triggers.
- Hydration: 2–3 liters a day. Dehydration headaches stack on top of migraine physiology.
- Caffeine: consistent daily amount or — better — a gradual taper off. Erratic caffeine is worse than steady caffeine.
- Exercise: 30 minutes of aerobic activity, 4–5 days a week. Walking counts. Benefits are similar in magnitude to some preventive medications.
- Stress management: CBT for migraine (available via apps like Migraine Mentor) has trial evidence as strong as some drugs.
See the diet triggers article and the supplement protocol for the detailed nutrition and supplement piece.
How to Track: Diaries and Apps
You cannot manage what you do not measure, and insurance companies will not pay for advanced treatments without documented headache days. A good diary captures, for each day: headache yes/no, severity 0–10, duration, any medication taken (dose and time), menstrual day, sleep hours, and suspected triggers. Useful tools:
- Migraine Buddy — the most popular free app; generates reports your neurologist can actually read.
- N1-Headache (formerly Curelator) — a research-grade tracker that identifies individual trigger correlations over 90 days.
- Paper calendar — still beats no tracking at all.
Bring a printed or exported report to every appointment. "About two weeks a month, I think" is a losing argument with insurance. "18 headache days in March, 16 in April, 17 in May" is a winning one.
What Recovery Looks Like
Recovery from chronic migraine with MOH is measured in weeks to months, not days. A realistic timeline for someone doing outpatient detox plus a new preventive:
- Weeks 1–2: worst stretch. Rebound headache, irritability, sleep disruption. Bridge therapy helps. Do not abandon the plan here.
- Weeks 3–6: slow improvement. Headache days begin to drop. Intensity softens before frequency does, often.
- Weeks 6–12: preventive fully kicks in. Many patients cross back under 15 headache days per month.
- Month 4–6: stable new baseline. This is when to judge whether the preventive is working and whether to switch, add, or keep going.
Re-converting from chronic to episodic is a real, studied outcome. It does not happen for everyone — roughly half to two-thirds of motivated patients who complete detox and maintain a preventive end up back in the episodic range. The other third may remain chronic but with fewer overall headache days and better function. Either is a meaningful win.
A final practical rule: once off the overused medication, stay off. The brain has a long memory. Reintroducing daily triptans, daily Excedrin, or daily opioids almost always drags patients back into chronic territory within months. Acute medication is for acute attacks — keep a mental line at 8 days of acute use per month, not 10, as a safety margin.
When to Pursue Disability
Not every person with chronic migraine can keep working full time, and nobody should feel ashamed about naming that honestly. Indicators that disability is worth pursuing:
- Headache on 20+ days per month despite a fair trial of at least two preventives (one usually being Botox or a CGRP antibody).
- Cognitive impairment from attacks or medications that impedes job tasks.
- Documented missed workdays that outpace available leave.
- Comorbid depression, PTSD, or anxiety that amplifies the functional impact.
The U.S. Social Security Administration does not have a dedicated migraine listing, but chronic migraine can qualify under listings for neurological impairment (11.00 series) or, more often, via a medical-vocational allowance that adds up headache days, cognitive limitations, and documented treatment failures. Private long-term disability (LTD) policies through employers are often more accessible than SSDI; if you have one, read the policy's definition of "own occupation" vs "any occupation." Detailed headache diaries, neurologist letters, Botox and CGRP records, and work absence documentation are the paper trail that wins these claims. A specialized disability attorney is worth the 25% contingency fee for contested cases.
Key Research Papers
- Aurora SK, et al. OnabotulinumtoxinA for treatment of chronic migraine: results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 1 trial. Cephalalgia. 2010.
- Diener HC, et al. OnabotulinumtoxinA for treatment of chronic migraine: results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 2 trial. Cephalalgia. 2010.
- Katsarava Z, et al. Medication-overuse headache: where are we now? Curr Pain Headache Rep. 2012.
- Bigal ME, Lipton RB. Concepts and mechanisms of migraine chronification. Headache. 2008.
Live PubMed Searches
For further reading, these PubMed topic searches return current peer-reviewed work on chronic migraine and medication overuse headache:
- Chronic migraine ICHD-3 criteria
- Medication overuse headache detox strategies
- OnabotulinumtoxinA PREEMPT protocol
- CGRP monoclonal antibodies in chronic migraine
- Opioid and butalbital overuse headache
- Episodic to chronic migraine chronification
- Occipital nerve blocks for migraine
- Neuromodulation devices for migraine
Connections
- CGRP Inhibitors and Preventives
- Diet Triggers and Elimination Protocol
- Magnesium, Riboflavin, and Supplements
- Migraine Overview
- Insomnia
- Menstrual Migraine and Hormonal Triggers
- Aura and Visual Disturbances
- Triptans and Gepants — Acute Treatment
- Vestibular Migraine
- Chronic Pain
- Chronic Fatigue Syndrome
- Fibromyalgia
- Low-Dose Naltrexone
- Headache
- Depression
- Magnesium
- Anxiety
- Migraine in Pregnancy and Breastfeeding