CGRP Inhibitors and Migraine Preventives
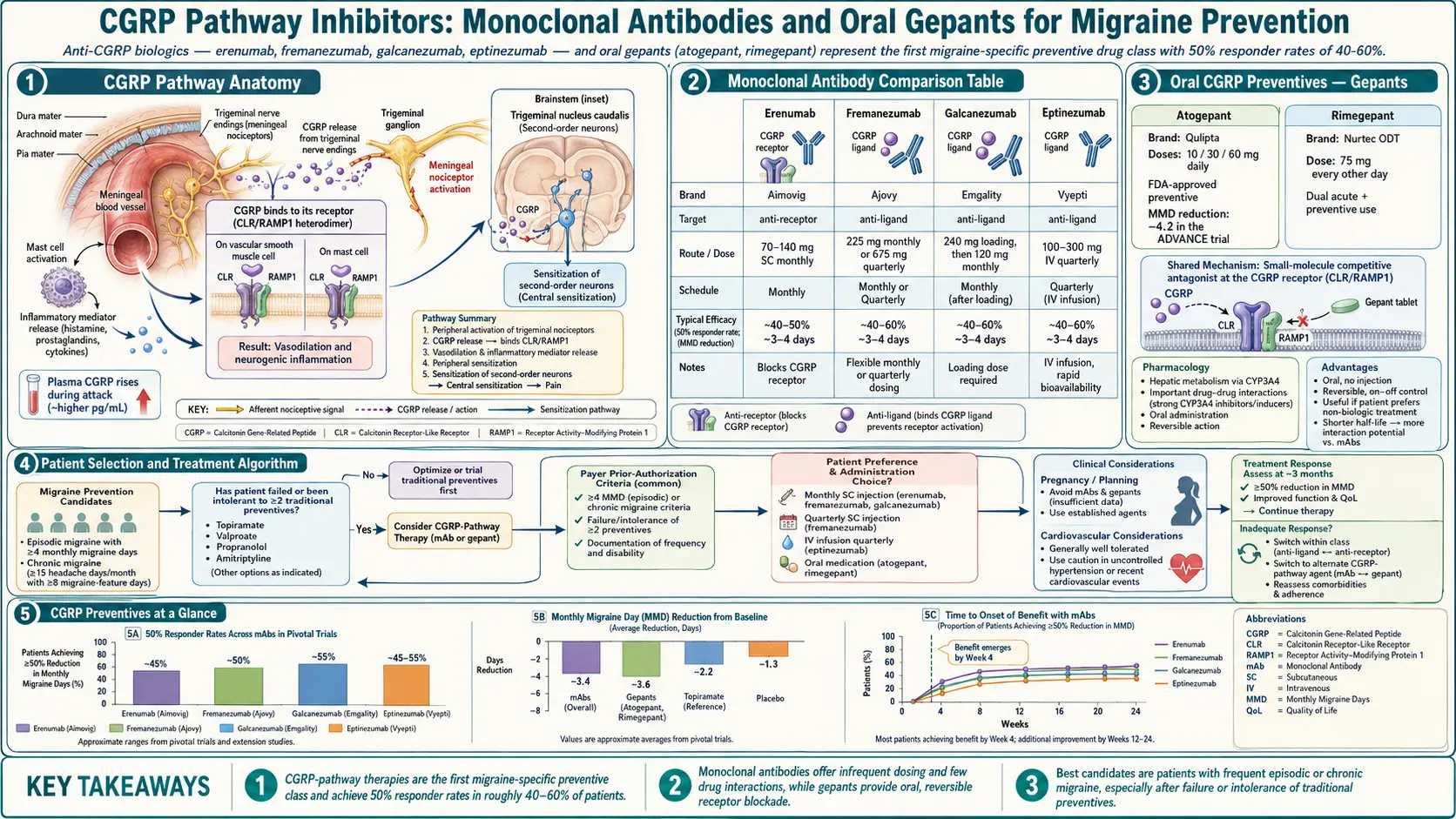
Table of Contents
- When to Start a Preventive
- The Classical Preventives
- Topiramate (Topamax)
- Propranolol and Beta-Blockers
- Amitriptyline and Nortriptyline
- Valproate (Depakote)
- Verapamil
- CGRP Monoclonal Antibodies
- Oral CGRP Blockers (Gepants)
- Botox for Chronic Migraine
- Sequencing Preventive Trials
- Combining Preventives
- Insurance Hurdles and Copay Help
- CGRP Safety Signals
- Pregnancy and Breastfeeding
- Tapering Off After Remission
- Key Research Papers
- Connections
- Featured Videos
When to Start a Preventive
The rough rule: four or more migraine days per month, or fewer attacks that are severe, long, or disabling enough to wreck your life. If you are using acute medication more than two days a week, you are also at risk for medication-overuse headache and need a preventive to break the cycle. See the chronic migraine article for that pattern.
A preventive is not supposed to stop every attack. A treatment is considered successful if it cuts your migraine days by at least 50% — the benchmark used in every trial. Some patients get 70–80% reduction; some get nothing. You cannot predict in advance which drug will be your drug, which is why preventive therapy is an honest trial-and-error process that usually takes a year or longer to sort out.
The Classical Preventives
Before CGRP blockers existed, migraine prevention relied on drugs developed for other diseases that happened to reduce headache frequency. They are still the first-line options for most insurance plans and, for a large minority of patients, they work. All five below are generic, cheap (usually under $20/month), and require a prior authorization for nothing. That is a real advantage when a CGRP biologic might cost $700/month without coverage.
Topiramate (Topamax)
An anticonvulsant repurposed for migraine prevention. Dosing usually starts at 25 mg at bedtime and titrates up by 25 mg every week to a target of 100 mg/day (split or at bedtime). Trials show a 50% responder rate around 35–50%.
Weight effect: causes weight loss — one reason it is popular. Cognitive side effects are the major problem and the nickname "Dopamax" is not a joke. Patients describe word-finding trouble, slowed thinking, and short-term memory lapses. Other reliable side effects: tingling in hands and feet (paresthesias), carbonated drinks tasting flat, kidney stones (1–2% risk), and a narrow-angle glaucoma risk in the first month.
Do not take topiramate if you need your cognitive edge for work (writers, coders, students during exams), have a history of kidney stones, or are trying to conceive — it is a known teratogen (cleft palate, lower IQ in exposed infants) and requires reliable contraception.
Propranolol and Beta-Blockers
A non-selective beta-blocker originally developed for high blood pressure. Dosing begins at 20–40 mg twice daily and titrates to 80–240 mg/day, often as a long-acting formulation. Responder rates are similar to topiramate, around 40–50%. Metoprolol and nadolol are reasonable alternatives.
Propranolol is the first preventive worth considering if you also have anxiety, essential tremor, high blood pressure, or POTS — one drug, multiple targets.
Side effects: fatigue, exercise intolerance (lower maximum heart rate), cold hands and feet, vivid dreams, erectile dysfunction in some men. Weight gain is modest (3–5 lb on average) but real.
Do not take propranolol if you have asthma (can trigger bronchospasm), significant bradycardia or AV block, poorly controlled diabetes (masks hypoglycemia), severe depression (can worsen it), or serious Raynaud's. Taper off — never stop abruptly — because of rebound hypertension and tachycardia.
Amitriptyline and Nortriptyline
A tricyclic antidepressant. Dosing is much lower than the antidepressant dose: 10–25 mg at bedtime, titrated to 50–100 mg if tolerated. Responder rates are similar to the others, around 40–50%. Nortriptyline (a tricyclic metabolite) is slightly less sedating and less anticholinergic — reasonable if amitriptyline knocks you flat.
Amitriptyline is the logical first pick if you also have insomnia, fibromyalgia, tension-type headache, irritable bowel, or chronic pain overlap. See chronic pain.
Side effects: dry mouth, constipation, urinary retention, weight gain (often 5–15 lb), morning grogginess, and in older adults confusion or falls. An ECG is prudent at higher doses because of QT prolongation risk.
Do not take amitriptyline if you are over 65 (on the Beers list of drugs to avoid in the elderly), have significant cardiac conduction disease, benign prostatic hypertrophy with retention, or narrow-angle glaucoma.
Valproate (Depakote)
Another anticonvulsant, FDA-approved for migraine prevention. Dosing is typically 500–1000 mg/day divided. Efficacy is real — roughly 45% responder rate — but the side-effect profile knocks it out of first-line use for most patients.
Side effects: weight gain (often 10–20 lb), hair loss, tremor, sedation, elevated liver enzymes, thrombocytopenia, pancreatitis (rare), and the notorious "Depakote belly." In women of reproductive age, valproate is a major teratogen — neural tube defects, cleft palate, and a 7–10 point drop in childhood IQ with in-utero exposure. Never start it in anyone who could become pregnant without an iron-clad contraception plan.
Valproate is reasonable for men or post-menopausal women who have failed two or three other classes, especially if they also have epilepsy or bipolar disorder.
Verapamil
A calcium channel blocker. Inside migraine care, verapamil's real home is hemiplegic migraine and cluster headache — it is first-line for the latter. For ordinary migraine it is a third- or fourth-line choice with mediocre evidence. Dosing starts at 80 mg three times daily and can climb to 240–480 mg/day for cluster.
Side effects: constipation (reliably), leg swelling, low blood pressure, bradycardia, AV block. High doses require periodic ECG monitoring. Do not combine with beta-blockers without cardiology input — the combination can cause dangerous bradycardia or heart block.
CGRP Monoclonal Antibodies
Calcitonin gene-related peptide (CGRP) is a signaling molecule released during migraine attacks that dilates blood vessels and amplifies pain in the trigeminal nerve. Block CGRP — or its receptor — and you short-circuit that cascade. The CGRP monoclonal antibody class, approved starting in 2018, was the first drug class ever developed specifically for migraine prevention. Four are currently on the U.S. market:
- Erenumab (Aimovig) — targets the CGRP receptor. 70 mg or 140 mg subcutaneous monthly, self-injected. Approved ages 18+.
- Fremanezumab (Ajovy) — targets the CGRP ligand. 225 mg monthly or 675 mg quarterly subcutaneous. Approved ages 18+.
- Galcanezumab (Emgality) — targets the CGRP ligand. Loading dose 240 mg, then 120 mg monthly subcutaneous. Approved ages 18+. Also approved for episodic cluster headache.
- Eptinezumab (Vyepti) — targets the CGRP ligand. 100 mg or 300 mg IV infusion every three months, given in an infusion center over about 30 minutes. Approved ages 18+.
Efficacy. Across the pivotal trials, the 50% responder rate is roughly 40–60%, and about 20% of patients get a 75% or better reduction — a response that classical preventives almost never deliver. Some patients become near-symptom-free. A small number (often called "super-responders") stop having migraines within weeks.
Onset. Many patients feel a reduction in the first week. Others need two or three monthly doses before judging. The adequate trial is three months (one quarterly cycle for eptinezumab).
Injection technique. The subcutaneous drugs ship as a prefilled pen or autoinjector. You inject into the thigh or abdomen (erenumab allows the upper arm with help). Store in the fridge, then let it warm to room temperature on the counter for 30 minutes before injecting — that single step eliminates most of the injection-site stinging patients complain about.
Who responds? There is no reliable biomarker. Episodic and chronic migraine both respond. Patients who failed two or more classical preventives still respond at similar rates to treatment-naive patients — which is why CGRP antibodies are worth trying even if topiramate and propranolol did nothing for you.
Oral CGRP Blockers (Gepants)
Small-molecule CGRP receptor antagonists — the "gepants" — are pills, not injections. Two are approved for prevention:
- Atogepant (Qulipta) — 10, 30, or 60 mg once daily. Approved for episodic and chronic migraine.
- Rimegepant (Nurtec ODT) — 75 mg orally disintegrating tablet every other day for prevention. Uniquely, the same tablet is also approved as an acute treatment for a migraine attack in progress, so one prescription covers both jobs.
Trial responder rates sit around 55–60%, similar to the injectables. The appeal is simple: no needles, faster onset of benefit (often by week one), and easier to stop if it is not working or you are planning pregnancy. The downsides: daily dosing, higher out-of-pocket cost than generics, and a ceiling on acute-use gepants if you use rimegepant for prevention. See triptans and gepants for the acute-dosing overlap.
Botox for Chronic Migraine
OnabotulinumtoxinA is approved only for chronic migraine — 15 or more headache days per month for at least three months, with at least 8 of those being migraine. It is not indicated for episodic migraine; trials failed that population.
The PREEMPT protocol: 155 units total across 31 injection sites, every 12 weeks. Sites span the forehead, temples, back of the head, neck, and upper shoulders. Most patients tolerate the injections with nothing worse than brief stinging. Some develop transient neck weakness or a dropped eyebrow for a few weeks. Responders usually see benefit after the second or third cycle, not the first.
Botox and CGRP antibodies can be combined. Many headache specialists use Botox as the anchor and add a CGRP drug on top for breakthrough days.
Sequencing Preventive Trials
Rules of a good preventive trial:
- One drug at a time. If you start two preventives simultaneously and get better, you do not know which one did it — and you are stuck on two sets of side effects.
- Titrate slowly. Most side effects come from ramping too fast. A slow climb to target dose over four to eight weeks is standard.
- Give it 2–3 months at target dose before declaring failure. CGRP antibodies need three months; classical preventives usually two.
- Keep a headache diary. Memory is unreliable once attacks become frequent. An app (Migraine Buddy, N1-Headache) or a paper calendar is enough — track days, severity, acute medication use, and menstrual timing.
Most insurance plans will require you to fail two classical preventives (typically a beta-blocker, topiramate, or tricyclic) before they will cover a CGRP antibody. That is "step therapy." Build the paper trail deliberately: take each drug, record the failure, and let your neurologist document it.
Combining Preventives
Combining is legitimate and common in refractory patients. Sensible pairings:
- CGRP antibody + Botox — the most studied combination; additive benefit in real-world data.
- CGRP antibody + oral preventive (propranolol or amitriptyline) — often helps patients who plateau on monotherapy.
- Propranolol + amitriptyline — a classical combination targeting different mechanisms; watch blood pressure and fatigue.
Avoid combining verapamil with a beta-blocker (bradycardia risk) and two drugs with the same side-effect profile (e.g., amitriptyline plus another strongly anticholinergic medicine).
Insurance Hurdles and Copay Help
CGRP drugs have a list price around $700 per month. Almost no one pays that. Typical path:
- Prior authorization — your neurologist's office submits chart notes documenting four or more migraine days per month and failure of two preventives. This is paperwork, not medicine, and sometimes takes two or three appeals.
- Step therapy — the insurer may demand failure of specific drugs (often topiramate and a beta-blocker) before approving a CGRP.
- Copay assistance. Every CGRP manufacturer runs a bridge program: Aimovig Ally, Ajovy Savings, Emgality Savings Program, Vyepti Access. With commercial insurance, patients often pay $0 to $5 per month. Federal insurance (Medicare, Medicaid, VA, Tricare) is excluded by law from manufacturer copay cards — for those patients, the manufacturer's patient assistance foundation or a third-party charity (HeadWise Network, Patient Access Network) is the alternative.
- Appeals. If denied, appeal. First-level appeals win roughly 40% of the time when the chart clearly documents diary days and prior failures.
CGRP Safety Signals
CGRP antibodies have a clean short-term safety record, but the drug class is only six years old in 2024–2026 use. Known and watched signals:
- Constipation — clearly real, dose-related, worst with erenumab. A small minority develop severe constipation needing drug discontinuation.
- Injection-site reactions — redness, itching, bruising; usually mild and improve with warming the pen before injection.
- Raynaud's phenomenon — new-onset or worsening cold fingers and color changes. CGRP is a vasodilator; blocking it tips some patients into vasospasm.
- Hypertension — erenumab carries a label warning; check blood pressure in the first few months.
- Cardiovascular events in older adults — still debated. CGRP is a protective vasodilator during ischemia in animal models. Trials excluded patients with recent MI or stroke, so we do not have solid data on safety in people with established cardiovascular disease. Headache specialists generally avoid CGRP drugs in patients with recent stroke, MI, or unstable angina until more data accumulate.
- Hair thinning — anecdotal post-marketing reports, mechanism unclear.
Pregnancy and Breastfeeding
Pregnancy data for CGRP antibodies are limited. Manufacturers recommend stopping at least 5 months before attempting conception (reflecting the long half-life; fremanezumab and galcanezumab sit around 30–45 days). Animal studies have not shown teratogenicity, but human registry data are still accumulating, and most headache specialists will not start a CGRP drug in someone trying to conceive.
Classical preventives during pregnancy: propranolol and amitriptyline have the longest human safety record and are preferred. Topiramate and valproate are contraindicated in pregnancy. For breastfeeding, propranolol, amitriptyline, and (based on the IgG size) probably CGRP antibodies are considered low-risk — the large antibodies do not cross into milk in meaningful amounts — but official labeling is cautious. Many migraines remit during the second and third trimesters because of high estrogen, which can let you drop preventives entirely for nine months. See menstrual migraine.
Tapering Off After Remission
Once your migraine days drop substantially for 6–12 months, a trial off the preventive is reasonable. Many patients maintain the benefit; some relapse within a few months and restart. Taper rather than stop abruptly for propranolol (rebound hypertension), topiramate (seizure risk with high doses), and amitriptyline (cholinergic rebound, flu-like symptoms). CGRP antibodies can simply be stopped — the drug clears slowly on its own and the taper is automatic.
If migraines return within three months of stopping, restart the drug that worked. There is no meaningful tachyphylaxis with CGRP antibodies — responders generally respond again.
Key Research Papers
- Goadsby PJ, et al. A controlled trial of erenumab for episodic migraine. N Engl J Med. 2017.
- Dodick DW, et al. Effect of fremanezumab compared with placebo for prevention of episodic migraine: a randomized clinical trial. JAMA. 2018.
- Stauffer VL, et al. Evaluation of galcanezumab for the prevention of episodic migraine: the EVOLVE-1 randomized clinical trial. JAMA Neurol. 2018.
- Ashina M, et al. Atogepant for the preventive treatment of migraine. N Engl J Med. 2020.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on migraine preventive pharmacology:
- CGRP monoclonal antibodies for migraine prevention
- Erenumab long-term safety and constipation
- Atogepant and rimegepant in migraine prevention
- Topiramate and cognitive side effects
- Propranolol for migraine prevention
- OnabotulinumtoxinA PREEMPT trials in chronic migraine
- CGRP antibodies in pregnancy and breastfeeding
- Adherence and discontinuation in migraine preventive therapy
Connections
- Chronic Pain
- POTS
- Chronic Migraine and Medication Overuse
- Menstrual Migraine and Hormonal Triggers
- Triptans and Gepants — Acute Treatment
- Migraine Overview
- Fibromyalgia
- Magnesium, Riboflavin, and Supplements
- Diet Triggers and Elimination Protocol
- Vestibular Migraine
- Aura and Visual Disturbances
- Headache
- Depression
- Insomnia
- Hypertension
- Epilepsy
- Post-Viral Triggers and ME/CFS
- Stroke