Vertigo & Ménière's Disease
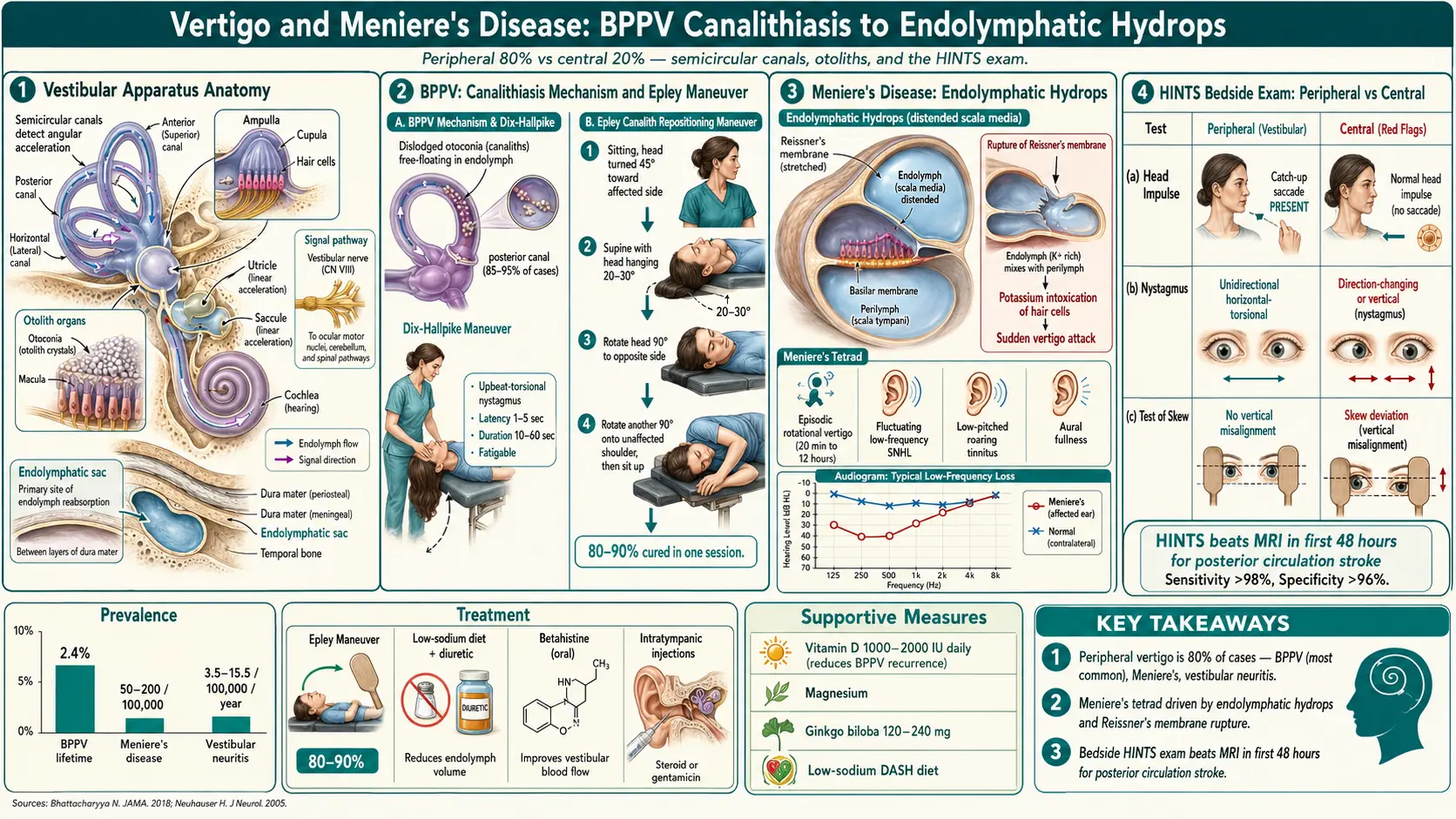
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Recent Research and Advances
- References & Research
- Featured Videos
1. Overview
Vertigo is the subjective sensation of rotational movement — either the feeling that oneself or the surrounding environment is spinning, tilting, or swaying — when no actual movement is occurring. Vertigo is a symptom, not a disease, and results from asymmetric input between the two vestibular systems or from disruption of central vestibular processing. It is one of the most common presenting complaints in both primary care and emergency medicine, accounting for approximately 5.6 million clinical visits per year in the United States. True vestibular vertigo must be distinguished from other forms of dizziness, including presyncope (lightheadedness from reduced cerebral perfusion), disequilibrium (imbalance without rotational sensation), and non-specific dizziness (psychiatric or multifactorial).
The causes of vertigo are broadly classified as peripheral (originating from the inner ear or vestibular nerve, accounting for approximately 80% of cases) or central (originating from the brainstem or cerebellum, accounting for approximately 20% of cases). The major peripheral causes include:
- Benign paroxysmal positional vertigo (BPPV) — the most common cause, accounting for approximately 20-30% of all vertigo cases
- Ménière's disease — characterized by episodic vertigo, sensorineural hearing loss, tinnitus, and aural fullness
- Vestibular neuritis — acute, prolonged vertigo from viral inflammation of the vestibular nerve
- Labyrinthitis — vestibular neuritis with concurrent hearing loss
- Superior semicircular canal dehiscence syndrome (SCDS) — vertigo and autophony from a bony defect in the superior canal
Central causes include vestibular migraine (increasingly recognized as a major cause of episodic vertigo), brainstem or cerebellar stroke, multiple sclerosis, acoustic neuroma (vestibular schwannoma), and cerebellar degeneration.
Ménière's disease is a chronic inner ear disorder characterized by the classic tetrad of episodic vertigo, fluctuating sensorineural hearing loss, tinnitus, and aural fullness. The pathological hallmark is endolymphatic hydrops — distension of the endolymphatic compartment of the inner ear. First described by the French physician Prosper Ménière in 1861, the disease affects quality of life significantly due to its unpredictable, recurrent nature and progressive hearing loss. Management ranges from dietary modifications and medical therapy to interventional procedures including intratympanic steroid or gentamicin injections, endolymphatic sac surgery, and vestibular nerve section.
2. Epidemiology
Vertigo is extremely common, with a lifetime prevalence of approximately 7-10% in the general population. The annual incidence of vertigo is estimated at 11-13 per 1,000 persons. Vertigo accounts for approximately 2-3% of emergency department visits and 5% of primary care visits in the United States. BPPV is the most prevalent vestibular disorder, with a lifetime prevalence of 2.4% and an annual incidence of 64 per 100,000. BPPV is more common in women (2-3:1 female-to-male ratio) and increases in prevalence with age, peaking in the 6th and 7th decades.
Ménière's disease has a prevalence of 50-200 per 100,000 population in the United States, with an annual incidence of approximately 15 per 100,000. The disease shows a slight female predominance (1.3:1), with peak onset between 40 and 60 years of age, though it can occur at any age. Bilateral involvement develops in approximately 25-40% of patients over time, typically within 5 years of diagnosis. Ménière's disease is more prevalent in Caucasians and appears to have higher reported rates in Northern Europe and North America. A positive family history is present in approximately 7-10% of cases, suggesting genetic predisposition.
Vestibular neuritis has an annual incidence of approximately 3.5-15.5 per 100,000, with peak incidence between ages 40 and 60. Vestibular migraine is increasingly recognized as a major cause of episodic vertigo, with a prevalence of approximately 1-2.7% in the general population and affecting up to 10-30% of patients evaluated in dizziness clinics. It is the most common cause of spontaneous episodic vertigo in children and young adults, with a strong female predominance (3-5:1).
3. Pathophysiology
Normal Vestibular Physiology
The vestibular system detects head motion and position relative to gravity through two types of sensory organs in each inner ear: the three semicircular canals (horizontal/lateral, anterior/superior, and posterior), which detect angular (rotational) acceleration, and the two otolith organs (utricle and saccule), which detect linear acceleration and head position relative to gravity. Each semicircular canal contains a cupula with embedded hair cells that are deflected by endolymph flow during head rotation. The otolith organs contain a macula with hair cells topped by an otolithic membrane embedded with calcium carbonate crystals (otoconia). Vestibular signals are transmitted via the vestibular nerve (cranial nerve VIII) to the vestibular nuclei in the brainstem, which integrate information with visual and proprioceptive inputs to maintain balance, spatial orientation, and gaze stability through the vestibulo-ocular reflex (VOR).
Benign Paroxysmal Positional Vertigo (BPPV)
BPPV results from dislodged otoconia (calcium carbonate crystals) that migrate from the utricle into one of the semicircular canals, most commonly the posterior canal (85-95% of cases), followed by the horizontal (lateral) canal (5-15%) and rarely the anterior (superior) canal (<2%). Two mechanisms are recognized: canalithiasis (free-floating otoconia within the canal lumen, the more common mechanism) and cupulolithiasis (otoconia adherent to the cupula). In canalithiasis, head movements cause the free-floating otoconia to shift within the canal, generating endolymph flow that deflects the cupula and creates an inappropriate vestibular signal. This produces a brief, intense sensation of vertigo with characteristic nystagmus whose direction corresponds to the affected canal (upbeat-torsional for posterior canal BPPV, direction-changing horizontal for lateral canal BPPV).
Ménière's Disease: Endolymphatic Hydrops
The pathological hallmark of Ménière's disease is endolymphatic hydrops — distension of the endolymph-filled membranous labyrinth due to impaired reabsorption or overproduction of endolymph. The endolymphatic system normally maintains a precise ionic composition (high potassium, low sodium) through the activity of the stria vascularis and the endolymphatic sac, which is the primary site of endolymph reabsorption. In Ménière's disease, dysfunction of the endolymphatic sac or its drainage pathways leads to progressive accumulation of endolymph, causing distension of the cochlear duct (scala media), saccule, and utricle.
The mechanism by which endolymphatic hydrops produces the episodic symptoms of Ménière's disease is debated, but the leading theory involves rupture of Reissner's membrane (the thin membrane separating the potassium-rich endolymph from the sodium-rich perilymph). When the distended membrane ruptures, potassium-rich endolymph floods into the perilymphatic space, causing potassium intoxication of the vestibular and cochlear hair cells and nerve fibers. This produces sudden depolarization followed by blockade of neural transmission, resulting in the acute vertigo attack, hearing loss, tinnitus, and aural fullness. The membrane subsequently heals, endolymph-perilymph homeostasis is restored, and symptoms resolve until the next rupture episode. Over time, repeated episodes of hair cell potassium poisoning lead to cumulative damage and progressive, permanent sensorineural hearing loss.
Vestibular Neuritis
Vestibular neuritis is caused by inflammation and demyelination of the vestibular nerve, most commonly attributed to reactivation of herpes simplex virus type 1 (HSV-1) in the vestibular ganglion. Pathological studies have demonstrated HSV-1 DNA in vestibular ganglia and inflammatory infiltrates in the vestibular nerve. The inflammation typically affects the superior division of the vestibular nerve (which innervates the horizontal and anterior semicircular canals and the utricle) more than the inferior division (which innervates the posterior semicircular canal and the saccule), producing a characteristic pattern of canal dysfunction. The sudden unilateral vestibular loss creates an asymmetry in tonic vestibular input to the brainstem, producing the acute vertiginous symptoms, spontaneous nystagmus (beating away from the affected side), and postural imbalance.
Vestibular Migraine
Vestibular migraine pathophysiology involves trigemino-vascular activation and cortical spreading depression affecting brainstem vestibular nuclei and their connections to the vestibular cortex, thalamus, and cerebellum. Release of calcitonin gene-related peptide (CGRP) and substance P from trigeminal afferents may directly modulate vestibular hair cell and nerve function. Central sensitization of vestibular pathways leads to heightened vestibular sensitivity during and between migraine attacks. Genetic studies suggest shared susceptibility loci between migraine and vestibular dysfunction.
4. Etiology and Risk Factors
Benign Paroxysmal Positional Vertigo (BPPV)
- Idiopathic — the most common cause (50-70% of cases), likely related to age-related degeneration and detachment of otoconia
- Head trauma — responsible for 7-17% of BPPV cases; may cause bilateral BPPV
- Vestibular neuritis — BPPV develops in 10-15% of patients following vestibular neuritis
- Prolonged bed rest or supine positioning — post-surgical, hospitalization
- Osteoporosis and vitamin D deficiency — associated with increased BPPV risk and recurrence; vitamin D supplementation may reduce recurrence
- Female sex and advancing age — risk increases with age, especially in women
Ménière's Disease
- Impaired endolymphatic sac function — reduced endolymph reabsorption due to anatomical, inflammatory, or vascular factors
- Genetic predisposition — familial clustering in 7-10% of cases; associations with DTNA, FAM136A, and aquaporin genes
- Autoimmune mechanisms — elevated circulating immune complexes, anti-heat shock protein 70 antibodies, and association with other autoimmune diseases; some patients respond to immunosuppressive therapy
- Viral infection — herpes simplex virus, cytomegalovirus, and varicella-zoster virus DNA detected in endolymphatic sac tissue
- Allergic factors — higher prevalence of allergy in Ménière's patients (up to 40%); allergic inflammation may affect endolymphatic sac function
- Vascular factors — migraine and cardiovascular risk factors are associated with Ménière's disease
- Anatomical variations — small or abnormally positioned endolymphatic sac and duct; narrow vestibular aqueduct
Vestibular Neuritis
- Viral reactivation — HSV-1 reactivation in the vestibular ganglion (primary proposed mechanism)
- Preceding upper respiratory infection — reported in 40-50% of cases
- Vascular ischemia — anterior vestibular artery territory ischemia (alternative hypothesis)
Central Causes of Vertigo
- Vestibular migraine — history of migraine, female sex, family history of migraine
- Posterior circulation stroke — hypertension, diabetes, atrial fibrillation, hyperlipidemia, smoking, advanced age
- Multiple sclerosis — demyelinating plaques involving vestibular pathways
- Vestibular schwannoma (acoustic neuroma) — benign tumor of Schwann cells on the vestibular nerve; neurofibromatosis type 2
- Cerebellar degeneration — alcohol abuse, paraneoplastic syndromes, genetic ataxias
5. Clinical Presentation
Benign Paroxysmal Positional Vertigo (BPPV)
BPPV presents with brief episodes of intense rotational vertigo triggered by specific head position changes — rolling over in bed, looking up, bending forward, or tilting the head back. Each episode typically lasts 10-60 seconds (canalithiasis) or may be more sustained (cupulolithiasis). There is characteristically a latency period of 1-5 seconds between the provocative head movement and onset of vertigo. Episodes may be accompanied by nausea and transient nystagmus. Between attacks, patients may feel normal or have mild unsteadiness. There is no hearing loss, tinnitus, or neurological symptoms with BPPV. The condition may remit spontaneously and recur.
Ménière's Disease
The classic Ménière's attack consists of four cardinal symptoms occurring together:
- Episodic rotational vertigo — spontaneous attacks lasting 20 minutes to 12 hours (typically 2-4 hours); associated with severe nausea, vomiting, and inability to stand or walk; not triggered by head position changes; occurs without warning or may be preceded by aural symptoms
- Fluctuating sensorineural hearing loss — initially low-frequency hearing loss that fluctuates (worsens during attacks and partially recovers); over years, progresses to involve all frequencies and becomes permanent; ultimately affects moderate-to-severe range (40-60 dB) in most patients
- Tinnitus — typically low-pitched roaring or buzzing in the affected ear; intensifies before and during attacks
- Aural fullness — sensation of pressure or blockage in the affected ear; often precedes attacks by minutes to hours
Attacks are typically episodic and unpredictable, occurring in clusters over weeks to months followed by periods of remission. Attack frequency varies widely, from several per week to a few per year. Over time, vestibular function deteriorates progressively, and some patients enter a "burnt-out" phase where vertigo attacks diminish or cease but hearing loss and tinnitus persist.
Vestibular Neuritis
Vestibular neuritis presents with the sudden onset of severe, continuous rotational vertigo lasting days to weeks, accompanied by nausea, vomiting, and postural imbalance. The vertigo is present at rest, worsened by head movement, and is not triggered by specific positions. Physical examination reveals spontaneous horizontal-torsional nystagmus beating toward the unaffected ear, positive head impulse test (corrective saccade when the head is rapidly turned toward the affected side), and deviation of gait and posture toward the affected side. Crucially, hearing is preserved in vestibular neuritis (if hearing is affected, the diagnosis is labyrinthitis). The acute phase typically resolves over 1-3 weeks through central vestibular compensation.
Red Flags for Central Vertigo
Clinical features suggesting a central cause (brainstem or cerebellar) requiring urgent evaluation include:
- Vertical or pure torsional nystagmus (suggests central pathology)
- Direction-changing nystagmus not consistent with BPPV
- Normal head impulse test with nystagmus (HINTS protocol: suggests stroke rather than vestibular neuritis)
- Severe imbalance or inability to stand disproportionate to the degree of nystagmus
- Acute-onset hearing loss with vertigo (consider labyrinthine infarction or acoustic neuroma)
- Associated neurological symptoms — diplopia, dysarthria, dysphagia, facial numbness, limb weakness or ataxia (posterior circulation stroke)
- New-onset headache with vertigo, particularly sudden severe headache (cerebellar hemorrhage)
6. Diagnosis
Bedside Clinical Tests
- Dix-Hallpike maneuver — the definitive bedside test for posterior canal BPPV; the patient is rapidly brought from sitting to a supine position with the head hanging 20-30 degrees below the table edge and rotated 45 degrees to one side; a positive test produces upbeat-torsional nystagmus with a latency of 1-5 seconds, duration of 10-60 seconds, and fatigability with repeated testing; the direction of the torsional component identifies the affected ear
- Supine roll test — for horizontal canal BPPV; the supine patient's head is rapidly rotated 90 degrees to each side; direction-changing horizontal nystagmus (geotropic or apogeotropic) identifies the affected canal
- HINTS examination (Head Impulse, Nystagmus, Test of Skew) — a bedside protocol with sensitivity >98% and specificity >96% for distinguishing peripheral from central causes of acute vestibular syndrome (superior to MRI in the first 48 hours for posterior fossa stroke); a "dangerous" HINTS pattern (normal head impulse test, direction-changing nystagmus, or skew deviation) suggests central pathology
- Head impulse test — rapid passive head rotation toward each side while the patient fixates on the examiner's nose; a corrective catch-up saccade indicates ipsilateral vestibular hypofunction
- Romberg test and tandem gait — assess postural stability
Audiological Testing
- Pure-tone audiometry — essential for Ménière's disease diagnosis; demonstrates low-frequency sensorineural hearing loss (initially affecting 250 Hz and 500 Hz) in the early stages, progressing to flat moderate-severe loss; serial audiometry documents fluctuation and progression
- Speech discrimination testing — reduced speech recognition score disproportionate to pure-tone thresholds may indicate retrocochlear pathology (vestibular schwannoma)
- Electrocochleography (ECoG) — measures summating potential to action potential (SP/AP) ratio; an elevated ratio (>0.4-0.5) suggests endolymphatic hydrops and supports Ménière's diagnosis
Vestibular Function Testing
- Videonystagmography (VNG) — records eye movements during positional testing, smooth pursuit, saccades, and caloric stimulation; caloric testing identifies unilateral vestibular weakness (>25% reduced caloric response on one side)
- Video head impulse test (vHIT) — quantitative measurement of VOR gain for each semicircular canal; reduced gain and overt/covert saccades indicate vestibular hypofunction
- Vestibular evoked myogenic potentials (VEMPs) — cervical VEMPs (cVEMPs) assess saccular function; ocular VEMPs (oVEMPs) assess utricular function; abnormal in Ménière's disease, superior canal dehiscence, and vestibular schwannoma
- Rotary chair testing — evaluates bilateral vestibular function and central vestibular processing
Imaging
- MRI of the brain with gadolinium — indicated to rule out vestibular schwannoma, cerebellopontine angle tumors, brainstem or cerebellar stroke, multiple sclerosis plaques, and other central pathology
- MRI of the inner ear with intratympanic or intravenous gadolinium — can directly visualize endolymphatic hydrops (hydrops MRI) and is increasingly used to confirm Ménière's disease
- CT temporal bone — indicated for suspected superior semicircular canal dehiscence, cholesteatoma, or temporal bone fracture
Ménière's Disease Diagnostic Criteria (AAO-HNS 2015)
Definite Ménière's disease requires:
- Two or more spontaneous episodes of vertigo, each lasting 20 minutes to 12 hours
- Audiometrically documented low-to-medium frequency sensorineural hearing loss in the affected ear on at least one occasion before, during, or after one of the episodes of vertigo
- Fluctuating aural symptoms (hearing loss, tinnitus, or aural fullness) in the affected ear
- Not better accounted for by another vestibular diagnosis
7. Treatment
BPPV: Canalith Repositioning Maneuvers
Canalith repositioning procedures (CRPs) are the first-line treatment for BPPV with success rates of 80-95% in a single session:
- Epley maneuver — the gold-standard treatment for posterior canal BPPV; a sequence of five head position changes that guide free-floating otoconia from the posterior semicircular canal back into the utricle through the common crus; each position is held for 30-60 seconds until nystagmus resolves; success rate of 80-90% per session and 95-98% after 2-3 sessions
- Semont (liberatory) maneuver — alternative for posterior canal BPPV; involves rapid 180-degree rotation from one lateral position to the opposite side; success rate approximately 75-90%
- Lempert (BBQ roll) maneuver — for horizontal canal BPPV (geotropic variant); sequential 90-degree head rotations in the supine position toward the unaffected ear through 360 degrees
- Gufoni maneuver — for horizontal canal BPPV (both geotropic and apogeotropic variants)
Vestibular suppressant medications (meclizine, dimenhydrinate) should not be used as primary treatment for BPPV, as they do not address the underlying cause and may impair vestibular compensation. Medications may be used briefly for severe nausea. Recurrence of BPPV occurs in approximately 15-20% per year; vitamin D supplementation (in deficient patients) may reduce recurrence risk.
Ménière's Disease: Conservative Management
- Dietary sodium restriction — limit to 1,500-2,000 mg sodium per day; cornerstone of long-term management; reduces endolymph volume; many patients report significant reduction in attack frequency
- Caffeine and alcohol avoidance — may trigger attacks in some patients
- Adequate hydration — maintaining consistent fluid intake
- Stress management — stress is a recognized trigger for Ménière's attacks
- Betahistine (Serc) — histamine H1 agonist and H3 antagonist; widely used in Europe and internationally (not FDA-approved in the US); doses of 24-48 mg three times daily; improves cochlear and vestibular blood flow; reduces attack frequency in many patients; well-tolerated; evidence from the BEMED trial showed no significant benefit over placebo for attack frequency but is still widely prescribed
- Diuretics — hydrochlorothiazide (25-50 mg daily) or triamterene-hydrochlorothiazide (37.5/25 mg daily); aim to reduce endolymph volume; commonly used despite limited controlled trial evidence
Ménière's Disease: Acute Attack Treatment
- Vestibular suppressants — meclizine (25-50 mg), dimenhydrinate (50-100 mg), or diazepam (5-10 mg) for acute vertigo episodes
- Antiemetics — promethazine (25 mg), ondansetron (4-8 mg) for nausea and vomiting
- Rest in a dark, quiet room during acute attacks
Ménière's Disease: Interventional Therapies
- Intratympanic dexamethasone injection — corticosteroid injected through the tympanic membrane into the middle ear; anti-inflammatory effect on the inner ear; preserves hearing; response rates of 70-90% for vertigo control; may require repeated injections; increasingly used as first-line interventional therapy
- Intratympanic gentamicin injection — aminoglycoside antibiotic that is selectively vestibulotoxic; delivered through the tympanic membrane to ablate vestibular function in the affected ear; vertigo control rates of 80-95%; risk of sensorineural hearing loss (10-30%) limits its use; low-dose protocols reduce hearing loss risk; reserved for patients failing conservative management
Ménière's Disease: Surgical Options
- Endolymphatic sac decompression/shunt — surgical decompression of the endolymphatic sac with or without shunt placement; hearing-preserving procedure; vertigo control in 60-80% of patients; debated efficacy due to lack of strong sham-controlled data
- Vestibular nerve section — selective surgical division of the vestibular portion of cranial nerve VIII (retrosigmoid or middle fossa approach); preserves hearing; vertigo control rates of 90-95%; significant surgical risks (CSF leak, hearing loss, facial nerve injury)
- Labyrinthectomy — complete surgical destruction of the vestibular and cochlear apparatus; reserved for patients with non-serviceable hearing; vertigo control approaches 95-100%; results in total hearing loss in the operated ear
Vestibular Neuritis Treatment
- Acute phase — short-term vestibular suppressants (diazepam, meclizine) and antiemetics for the first 24-72 hours only; corticosteroids (methylprednisolone taper starting at 100 mg for 3 days, then tapering over 3 weeks) within the first 72 hours improves vestibular recovery; antivirals (valacyclovir) have not shown consistent benefit
- Vestibular rehabilitation — the cornerstone of recovery; structured physical therapy program of gaze stabilization, habituation, and balance exercises promotes central vestibular compensation; early initiation and consistent performance significantly improve outcomes; vestibular suppressant medications should be discontinued within 48-72 hours to avoid impairing compensation
Vestibular Migraine Treatment
- Acute treatment — triptans (rizatriptan, sumatriptan), vestibular suppressants, and NSAIDs
- Preventive medications — beta-blockers (propranolol 40-160 mg/day), tricyclic antidepressants (amitriptyline 10-75 mg/day), topiramate (50-100 mg/day), venlafaxine (37.5-150 mg/day), CGRP monoclonal antibodies (erenumab, galcanezumab, fremanezumab)
- Lifestyle modifications — trigger avoidance (dietary, sleep, stress), regular sleep schedule, regular exercise
8. Complications
- Falls and fall-related injuries — vertigo and vestibular dysfunction significantly increase fall risk, particularly in elderly patients; fractures, head injuries, and associated morbidity
- Progressive hearing loss — Ménière's disease causes progressive sensorineural hearing loss over years; bilateral involvement in 25-40% of patients can cause severe bilateral hearing impairment
- Chronic imbalance — incomplete vestibular compensation following vestibular neuritis or chemical/surgical vestibular ablation; persistent unsteadiness exacerbated by visual complexity and head movements
- Drop attacks (Tumarkin's otolithic crisis) — sudden falls without loss of consciousness due to acute otolithic dysfunction in Ménière's disease; dangerous and unpredictable; occur in approximately 5-10% of Ménière's patients
- Psychological comorbidity — anxiety (especially anticipatory anxiety about attacks), depression, agoraphobia, and panic disorder are highly prevalent in patients with chronic vestibular disorders; up to 50% of Ménière's disease patients report significant psychological distress
- Driving and occupational impairment — unpredictable vertigo attacks may preclude driving, operating machinery, or working at heights
- Missed diagnosis of central pathology — posterior fossa stroke, vestibular schwannoma, or multiple sclerosis misdiagnosed as peripheral vestibular disorder
- Persistent postural-perceptual dizziness (PPPD) — chronic, non-vertiginous dizziness and unsteadiness that may develop following resolution of an acute vestibular event; a functional vestibular disorder requiring specific treatment (SSRI/SNRI, vestibular rehabilitation, cognitive behavioral therapy)
9. Prognosis
BPPV has an excellent prognosis. Canalith repositioning maneuvers resolve symptoms in 80-95% of patients within 1-3 treatment sessions. However, BPPV has a significant recurrence rate of approximately 15-20% per year and 50% over 5 years. Most recurrences respond to repeated repositioning maneuvers. BPPV does not cause permanent hearing loss or neurological damage.
Ménière's disease follows a variable course. Vertigo attacks typically occur in clusters over months to years, with periods of remission. Many patients experience a natural "burn-out" of vertigo attacks over 5-10 years as vestibular function progressively declines, though hearing loss and tinnitus persist. Approximately 60-70% of patients are adequately managed with conservative measures (dietary modification, medical therapy). An additional 15-25% require intratympanic therapy, and 5-10% ultimately require surgical intervention. Bilateral involvement develops in 25-40% of patients, significantly worsening prognosis for both hearing and balance. Overall, most patients maintain functional independence, but the unpredictable nature of attacks causes significant lifestyle limitation and psychological distress.
Vestibular neuritis has a generally favorable prognosis. The acute vertigo resolves within 1-3 weeks through central vestibular compensation. However, approximately 30-50% of patients have residual vestibular hypofunction on testing, and 10-15% develop chronic dizziness or PPPD. Vestibular rehabilitation significantly improves outcomes and accelerates compensation. Approximately 10-15% of patients develop BPPV in the months following vestibular neuritis. Recurrence of vestibular neuritis in the same ear is rare (<2%), but it can occur in the contralateral ear.
10. Prevention
- BPPV prevention — vitamin D supplementation (when serum levels are <20 ng/mL) has been shown to reduce BPPV recurrence by approximately 25-45%; avoiding triggers (rapid head movements, sleeping on the affected side); prompt treatment of episodes to reduce duration and fall risk
- Ménière's disease flare prevention — strict dietary sodium restriction (1,500-2,000 mg/day); consistent hydration; caffeine and alcohol moderation; stress management; regular sleep; adherence to prescribed medications (betahistine, diuretics); treatment of underlying allergies if present
- Fall prevention — home safety modifications (handrails, non-slip mats, adequate lighting); avoidance of sedating medications when possible; vestibular rehabilitation for balance training; assistive devices when needed
- Vestibular migraine prevention — migraine trigger identification and avoidance (dietary triggers, sleep irregularity, stress, hormonal fluctuations); prophylactic medications; regular exercise; adequate hydration
- Prevention of posterior circulation stroke — management of vascular risk factors (hypertension, diabetes, hyperlipidemia, atrial fibrillation, smoking cessation) to reduce risk of central vertigo from cerebrovascular disease
- Hearing preservation — early and aggressive treatment of Ménière's disease; hearing-preserving interventional approaches (intratympanic steroids, endolymphatic sac surgery) preferred over destructive procedures when possible
- Vestibular rehabilitation — proactive vestibular physical therapy following any vestibular insult to optimize central compensation and prevent chronic dizziness
11. Recent Research and Advances
Research in vestibular medicine has advanced considerably in recent years, with improved diagnostic tools, better understanding of disease mechanisms, and emerging therapies.
Endolymphatic hydrops imaging: Gadolinium-enhanced MRI of the inner ear now allows direct visualization of endolymphatic hydrops in vivo. Both intratympanic and intravenous gadolinium protocols have been developed, with 3T MRI demonstrating high sensitivity for detecting endolymphatic space distension. This imaging modality is becoming an increasingly important diagnostic tool for Ménière's disease and may help differentiate it from other conditions. Studies have shown that the degree of hydrops correlates with disease severity and hearing loss, though notably, hydrops can be present in asymptomatic individuals.
Vestibular migraine has emerged as one of the most common causes of episodic vertigo, with the publication of consensus diagnostic criteria by the Bárány Society and the International Headache Society in 2012. Research into the pathophysiology of vestibular migraine has identified shared mechanisms between migraine and vestibular dysfunction, including CGRP-mediated modulation of vestibular function. CGRP monoclonal antibodies (erenumab, fremanezumab, galcanezumab) approved for migraine prevention are being investigated for vestibular migraine, with early results showing promising reduction in vertigo attack frequency.
The HINTS examination (Head Impulse, Nystagmus, Test of Skew) has been validated as a bedside diagnostic approach that outperforms early MRI for detecting posterior fossa stroke in patients presenting with acute vestibular syndrome. Studies demonstrate >98% sensitivity for stroke detection when performed by trained clinicians, compared to approximately 80% sensitivity for diffusion-weighted MRI in the first 24-48 hours.
Intratympanic drug delivery has been refined with sustained-release formulations and novel agents. Sustained-release dexamethasone formulations (hydrogels, nanoparticles) are being developed to extend inner ear drug exposure and reduce the need for repeated injections. OTO-104 (poloxamer-based sustained-release dexamethasone) and OTO-313 (gacyclidine for tinnitus) represent innovative approaches to inner ear drug delivery. Research into gene therapy for inner ear disorders, including restoration of hair cell function through Atoh1 gene delivery, holds long-term promise for hearing restoration in Ménière's disease and other forms of sensorineural hearing loss.
Advances in vestibular implant technology offer potential for patients with bilateral vestibular loss. Multichannel vestibular implants that electrically stimulate the vestibular nerve to restore vestibular function have demonstrated feasibility in clinical trials, with improvements in balance, gaze stability, and quality of life in implanted patients.
12. References & Research
Historical Background
Prosper Ménière (1799-1862), a French physician at the Imperial Institute for Deaf-Mutes in Paris, first proposed in 1861 that episodes of vertigo, hearing loss, and tinnitus could originate from the inner ear rather than the brain, as was previously believed. His landmark presentation to the French Academy of Medicine described patients with the classic symptom triad and correlated their symptoms with inner ear pathology, fundamentally changing the understanding of vestibular disorders. Hallpike and Cairns confirmed the presence of endolymphatic hydrops in temporal bones of Ménière's disease patients in 1938. The Dix-Hallpike maneuver for diagnosing BPPV was described by Margaret Dix and Charles Hallpike in 1952. Robert Bárány won the Nobel Prize in Medicine in 1914 for his work on vestibular physiology, including caloric testing. The revolutionary Epley canalith repositioning maneuver was developed by John Epley in 1980 (published 1992), transforming the treatment of BPPV from a condition managed with vestibular suppressants to one cured in minutes with a simple head maneuver. The HINTS examination was developed by David Newman-Toker and colleagues, published in 2009, establishing a superior bedside approach to differentiating central from peripheral causes of acute vestibular syndrome.
Key Research Papers
- Bhattacharyya N, Gubbels SP, Schwartz SR, et al. Clinical practice guideline: benign paroxysmal positional vertigo (update). Otolaryngol Head Neck Surg. 2017;156(3_suppl):S1-S47.
- Lopez-Escamez JA, Carey J, Chung WH, et al. Diagnostic criteria for Ménière's disease (AAO-HNS 2015). J Vestib Res. 2015;25(1):1-7.
- Epley JM. The canalith repositioning procedure: for treatment of benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg. 1992;107(3):399-404.
- Newman-Toker DE, Kattah JC, Alvernia JE, Wang DZ. Normal head impulse test differentiates acute cerebellar strokes from vestibular neuritis. Neurology. 2008;70(24 Pt 2):2378-2385.
- Kattah JC, Talkad AV, Wang DZ, Hsieh YH, Newman-Toker DE. HINTS to diagnose stroke in the acute vestibular syndrome. Stroke. 2009;40(11):3504-3510.
- Lempert T, Olesen J, Furman J, et al. Vestibular migraine: diagnostic criteria (consensus document of the Bárány Society and International Headache Society). J Vestib Res. 2012;22(4):167-172.
- Strupp M, Magnusson M. Acute unilateral vestibulopathy. Neurol Clin. 2015;33(3):669-685.
- Naganuma H, Kawahara K, Tokumasu K, Okamoto M. Water may cure patients with Ménière disease. Laryngoscope. 2006;116(8):1455-1460.
- Patel M, Agarwal K, Arshad Q, et al. Intratympanic methylprednisolone versus gentamicin in patients with unilateral Ménière's disease: a randomised, double-blind, comparative effectiveness trial. Lancet. 2016;388(10061):2753-2762.
- Hallpike CS, Cairns H. Observations on the pathology of Ménière's syndrome. J Laryngol Otol. 1938;53(10):625-655.
- von Brevern M, Radtke A, Lezius F, et al. Epidemiology of benign paroxysmal positional vertigo: a population based study. J Neurol Neurosurg Psychiatry. 2007;78(7):710-715.
- Nakashima T, Pyyko I, Arroll MA, et al. Ménière's disease. Nat Rev Dis Primers. 2016;2:16028.
- Jeong SH, Kim HJ, Kim JS. Vestibular neuritis. Semin Neurol. 2013;33(3):185-194.
- Gurgél RK, Ward PD, Schwartz S, Norton MC, Foster NL, Tschanz JT. Relationship of hearing loss and dementia: a prospective, population-based study. Otol Neurotol. 2014;35(5):775-781.
- Jeong SH, Oh SY, Kim HJ, Koo JW, Kim JS. Vestibular dysfunction in migraine: effects of associated vertigo and motion sickness. J Neurol. 2010;257(6):905-912.
Research Papers
The following PubMed topic searches retrieve current peer-reviewed literature on Vertigo and Meniere's Disease. Each link opens a live PubMed query so you always see the most recent publications.
- Meniere's disease review
- BPPV Epley maneuver
- Vestibular neuritis acute vertigo
- Endolymphatic hydrops Meniere
- Betahistine Meniere's disease
- Intratympanic gentamicin Meniere
- Vestibular rehabilitation therapy
- Meniere low sodium diet
- Central versus peripheral vertigo diagnosis
- HINTS exam vertigo
- Ginkgo biloba vertigo
Connections
- Hearing & the Cochlea — interactive animation
- Tinnitus
- Dizziness
- Ginkgo Biloba
- Stress Management
- Magnesium
- Vitamin D3
- Vitamin B6
- Ginger
- Vestibular Migraine
- Migraine
- Headache
- Stroke
- Tinnitus Remedies
- Potassium
- Anxiety
- Sinusitis
- Nausea and Vomiting
- Hypertension
- Hearing Loss