Gluten-Free Diet: A Practical Guide
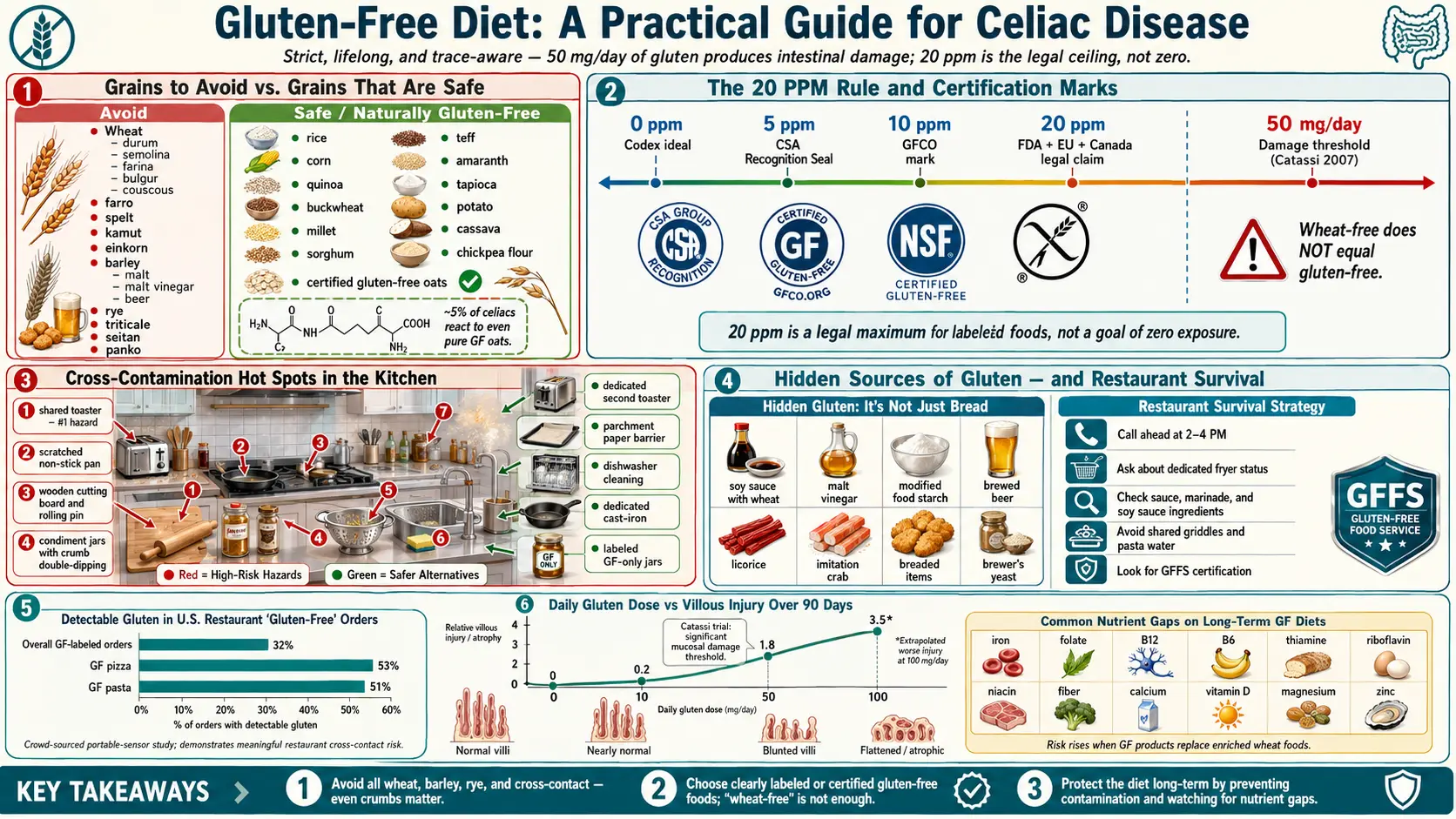
Table of Contents
- Why "Strict" Really Means Strict
- The FDA 20-ppm Rule — And What It Does Not Mean
- Grains to Avoid and Grains That Are Safe
- The Oats Question
- Hidden Sources of Gluten
- Cross-Contamination in a Shared Kitchen
- Eating Out — A Survival Strategy
- Travel and Dining Cards Abroad
- Labeling Laws and Certification Marks
- Non-Food Gluten Sources
- Medications and Supplements
- The Shared-Household Question
- Nutrient Gaps and the Processed GF Trap
- A Sample Week
- Cost and the U.S. Tax Deduction
- The Emotional Labor Nobody Warned You About
- Key Research Papers
- Connections
- Featured Videos
Why "Strict" Really Means Strict
If you have celiac disease, the gluten-free diet is not a preference, a trend, or a dial you can turn up and down depending on the week. It is a prescription — the only prescription that actually treats the disease. Every time gluten reaches the small intestine of a celiac patient, the immune system attacks the intestinal lining. The damage begins within hours, continues for days, and can be triggered by amounts small enough that you cannot taste, see, or smell them.
The quantity that matters is astonishingly small. Research by Catassi and colleagues in 2007 established that as little as 50 milligrams of gluten per day — about one-eightieth of a slice of ordinary bread — produces measurable intestinal damage in adults with celiac disease over three months. Lower, more intermittent doses also provoke symptoms and serology changes in sensitive individuals. There is no "cheat day." There is no "just a bite." The goal is zero, and the practical target is as close to zero as daily life allows.
That sounds grim. It is not, once the kitchen is sorted out and the shopping habits are rebuilt. But the first six months after diagnosis require re-learning almost every routine that involves food, because gluten is hiding in places most newly diagnosed patients never imagined.
The FDA 20-ppm Rule — And What It Does Not Mean
In the United States, any packaged food labeled "gluten-free" must contain fewer than 20 parts per million (ppm) of gluten. The same 20-ppm threshold is codified in the international Codex Alimentarius standard, the European Union Regulation 828/2014, the Canadian Food and Drug Regulations, and Australia & New Zealand labeling rules (Australia/NZ actually requires "no detectable gluten" for a gluten-free claim, a stricter standard than 20 ppm).
Twenty parts per million was chosen because studies showed that most celiac patients who kept total daily gluten intake under roughly 10 milligrams avoided mucosal damage. If you eat up to 500 grams of packaged "gluten-free" food per day at the 20-ppm ceiling, your theoretical maximum intake is 10 mg — at the safety edge but still below the 50-mg damage threshold from Catassi's work.
Two things this rule does not mean:
- 20 ppm is not zero. A minority of very sensitive celiac patients report symptoms at levels well below 20 ppm, and long-term microdosing exposure remains an active research debate. If your antibodies stay elevated and your biopsies do not heal despite a "perfect" diet, trace exposure from certified-GF products is a legitimate suspect.
- "Wheat-free" does not equal "gluten-free." A product labeled wheat-free may still contain barley malt, rye flour, or spelt. Read both claims independently.
Grains to Avoid and Grains That Are Safe
The grains that contain gluten — all members of the wheat, barley, and rye families — are:
- Wheat and every wheat variant: durum, semolina, farina, graham, bulgur, couscous, farro, spelt, kamut (khorasan), emmer, einkorn.
- Barley — including malt, malt extract, malt vinegar, malt syrup, most beer, and malt beverages.
- Rye and pumpernickel.
- Triticale, a wheat-rye hybrid.
- Seitan, which is pure wheat gluten sold as a meat substitute — one of the most dangerous foods on a vegan menu for a celiac.
- Panko, which is simply Japanese wheat breadcrumb.
Naturally gluten-free grains and starches include rice (white, brown, wild), corn, quinoa, buckwheat (unrelated to wheat despite the name), millet, sorghum, teff, amaranth, tapioca, potato, sweet potato, cassava, arrowroot, and chickpea flour. These are safe provided they have not been cross-contaminated during processing — a problem serious enough that certified-GF versions of naturally safe grains exist and are worth buying when available.
The Oats Question
Oats contain a protein called avenin, which is chemically similar to gluten but does not trigger the same immune response in the large majority of celiac patients. Pure oats are therefore biologically safe for most people with celiac disease.
The practical problem is that oats are rarely pure. Conventional oats are grown in rotation with wheat and barley, harvested with shared equipment, trucked in shared trailers, and milled in shared facilities. Cross-contact at any stage can push gluten content well above the 20-ppm threshold — sometimes into the thousands of ppm. Buying the generic canister of oats at the supermarket is not safe.
What is safe is certified gluten-free oats, grown on dedicated fields and processed with segregated equipment. The leading brands in the U.S. are GF Harvest (purity-protocol farm in Wyoming), Bob's Red Mill Gluten Free Oats, and Gluten-Free Oats (Montana). Read the label: "gluten-free oats" is the claim you need. Plain "oats" is not.
Even certified GF oats bother a small subset of celiac patients — roughly 5 percent react to the avenin itself. If you introduce oats and your symptoms return, stop. Retest serology after three months off oats to confirm.
Hidden Sources of Gluten
After the obvious breads, pastas, and pastries, the second tier of risk is ingredients that do not sound like gluten at all:
- Soy sauce. Most brewed soy sauce is fermented with wheat. Use tamari labeled gluten-free or coconut aminos.
- Malt vinegar. Made from barley. Distilled white, apple cider, rice, red wine, and balsamic vinegars are safe (the distillation process removes gluten proteins, and the FDA accepts distilled vinegars as gluten-free).
- Wheat-based thickeners in soups, gravies, and sauces. Restaurant "au jus" and "roux" are classic traps.
- Modified food starch. In the U.S., if the source is wheat, the label must say "wheat" under FALCPA (the Food Allergen Labeling and Consumer Protection Act), so modified food starch without a "wheat" disclosure is generally derived from corn or potato and is safe. In the European Union and many other jurisdictions, the allergen declaration applies differently — verify the source.
- Beer, ale, lager, stout. Barley-based. A growing category of gluten-removed beers (reduced below 20 ppm from a barley base) is technically permitted but remains controversial among celiac advocacy groups because the test methods may not catch all gluten fragments. Safer alternatives: beers brewed from sorghum, rice, or millet and labeled gluten-free from the start.
- Licorice candy (most contains wheat flour).
- Imitation crab and many processed meats (wheat binders).
- Breaded or dusted items in a salad bar — crispy chicken, croutons, some cheese blends.
- Brewer's yeast grown on spent barley mash.
Cross-Contamination in a Shared Kitchen
This is the section newly diagnosed patients most underestimate. If anyone else in your home still eats gluten, the kitchen becomes a minefield of shared surfaces. Wheat flour is particularly persistent — airborne flour dust from baking bread can stay suspended for hours and settle across every exposed surface in the room.
The practical rules that matter most:
- Separate toaster. Non-negotiable. A conventional toaster is impossible to clean of crumbs, and every gluten-free slice you toast in it picks up a dose. Buy a second toaster, label it, and keep it physically separated. A toaster oven that never sees gluten bread is an acceptable substitute.
- Separate condiment jars. The double-dipping rule: peanut butter, butter, mayonnaise, jam, cream cheese, and hummus jars used by someone who just spread gluten bread now contain crumbs. Keep your own labeled jars, use squeeze bottles where possible, or practice strict one-scoop-out-of-the-jar hygiene.
- Dedicated colander. Pasta water drains gluten proteins into the colander's mesh; no amount of washing reliably removes it. Buy a second colander, label it, and store it separately.
- Dedicated cutting board and wooden utensils. Wood is porous and absorbs gluten. Plastic or bamboo cutting boards develop scratches that trap proteins. Wooden spoons and rolling pins cannot be adequately decontaminated.
- Replace scratched non-stick pans. The scratch lines hold flour residue. Start fresh with a dedicated GF non-stick pan, and for cast iron, keep a separately seasoned skillet — the seasoning layer itself carries protein traces from past cooking.
- Dishwasher is generally fine. Hot water plus detergent plus rinse cycles decontaminate smooth surfaces (stainless steel, glass, ceramic, hard plastic) effectively. Hand-washing with a sponge that was just used on a gluten-covered pan is not fine — the sponge itself is the contaminated item.
- Parchment paper or foil between shared baking sheets and your food is a cheap, reliable barrier.
- Flour storage. If anyone bakes with wheat flour, do it when you are not home and clean every horizontal surface afterward. Better: keep wheat flour out of the house entirely and use GF flour for everyone's baking.
Eating Out — A Survival Strategy
Restaurants are the single biggest source of ongoing gluten exposure in otherwise strict celiac patients. A 2015 study by Leffler and colleagues (see Key Papers) found detectable gluten in roughly one-third of foods ordered as "gluten-free" at U.S. restaurants. The failure modes are predictable: shared fryers, flour-dusted grills, contaminated prep surfaces, staff who confuse gluten-free with low-carb, and the single pasta pot that was rinsed but never changed.
A workable approach:
- Call ahead at off-hours (2–4 PM) when the manager has time to answer questions. Ask: "Do you have a dedicated fryer for gluten-free items? Do you cook GF pasta in fresh water? Is the grill ever dusted with flour?"
- Dedicated-fryer fries are rarer than you think. In-N-Out's fries are cooked in a dedicated fryer and are generally safe. Chick-fil-A fries are not gluten-free — they share fryer oil with breaded chicken. Five Guys fries are dedicated. McDonald's fries contain a wheat derivative in the flavoring in the U.S. Always verify at the individual location.
- Chain audit is worth doing. Chipotle is widely considered celiac-friendly (corn tortillas and rice bowls prepared on a station separated from flour tortillas; ask them to change gloves). Pei Wei and P.F. Chang's maintain published gluten-free menus. Fast-casual chains vary locally — the published menu is the floor, the local kitchen is the ceiling.
- GIG-endorsed restaurants. The Gluten Intolerance Group runs a GFFS (Gluten-Free Food Service) certification program. Restaurants displaying the GFFS mark have passed a documented audit of their protocols. This is the strongest third-party signal available.
- Find Me Gluten Free. The crowd-sourced app is the best day-to-day tool for finding safer restaurants in unfamiliar cities. Read the recent reviews, not just the rating.
- Script your order. "I have celiac disease, which is a medical condition, not a preference. Even a crumb makes me sick. Can you check with the kitchen about the fryer and the prep surface?" Most servers respond well when the framing is medical rather than dietary.
Travel and Dining Cards Abroad
International travel is harder because the local staff may not speak English and the hidden-gluten ingredients differ by cuisine. Gluten-free dining cards are laminated wallet-sized cards that explain celiac disease and list what you cannot eat in the local language, written by native speakers. Well-regarded sources include SelectWisely, Legal Nomads, and the Celiac Travel project — cards exist for Spanish, French, Italian, German, Mandarin, Japanese, Vietnamese, Arabic, Hindi, and dozens of other languages.
Hand the card to the kitchen, not the waiter. Bring printed backups; phones lose charge. Learn the single most important phrase in the local language: "I cannot eat wheat, barley, or rye. It makes me very sick." In much of Italy, celiac disease is so well understood that gluten-free menus appear in ordinary neighborhood restaurants — Italy diagnoses pediatric celiac routinely and subsidizes gluten-free food. Ireland, Spain, Argentina, and Australia are also relatively celiac-aware. Most of Southeast Asia is not.
Labeling Laws and Certification Marks
The simple "gluten-free" claim under FDA rules means below 20 ppm and is legally enforceable. Beyond that, three third-party certification marks provide additional rigor:
- GFCO (Gluten-Free Certification Organization) — run by the Gluten Intolerance Group. Threshold: 10 ppm, half the FDA limit. The GFCO mark (a circle with "GF" inside) is the most widely seen certification on U.S. packaging and is the one most celiac dietitians recommend looking for first.
- CSA (Celiac Support Association) Recognition Seal — threshold 5 ppm. Stricter than GFCO but less commonly displayed.
- NSF Gluten-Free Certification — threshold 20 ppm, same as FDA, but with audited facility protocols.
- Crossed-grain symbol — used in Europe, Australia, and increasingly the U.S. by manufacturers licensed through national celiac societies. Threshold varies by licensing body but is typically 20 ppm or stricter.
A product with any of these marks is more reliable than one with only an unverified "gluten-free" claim on the front of the box.
Non-Food Gluten Sources
Most non-food exposures are theoretical risks that do not produce enough gluten to matter. A short list of what does and does not:
- Lipstick and toothpaste — almost never a problem in practice. Trace amounts of wheat derivatives are sometimes used, but the quantity transferred to the digestive tract is well below the damage threshold. Most celiac dietitians do not insist on gluten-free cosmetics unless symptoms persist mysteriously.
- Shampoo, conditioner, lotion — not absorbed through intact skin. Safe unless you eat them (relevant mainly for small children and lotion on hands that handle food).
- Communion wafers — a real and specific problem for Catholic and Protestant celiacs. Low-gluten hosts (made from wheat with most of the gluten removed, certified to contain trace amounts considered theologically valid as wheat bread by the Catholic Church) are available from suppliers such as the Benedictine Sisters of Perpetual Adoration. For most patients these are acceptable, but the most sensitive should consult their clergy about receiving only the cup.
- Play-Doh — contains wheat flour and will transfer gluten from hands to mouth. A real hazard for celiac children and for parents with celiac who handle it. Wheat-free play clay alternatives exist.
- Pepto-Bismol chewable tablets — historically contained gluten; reformulations vary. Check the current label.
- Envelope and stamp glue — an old worry that is no longer accurate; most adhesives use cornstarch or synthetic polymers.
Medications and Supplements
Most prescription and over-the-counter medications are gluten-free, but they are not labeled gluten-free. Inactive ingredients (binders, disintegrants, coatings) can include wheat starch, and generic versions of the same drug can have different inactives than the brand-name version. Pietzak's 2012 review remains the clearest patient-facing reference on this problem.
The workflow that works:
- Before filling a new prescription, ask the pharmacist (not the prescriber) to check the manufacturer's statement on gluten content. Pharmacists have access to the full inactive-ingredient lists and can call the manufacturer if needed.
- When a generic is substituted at refill, re-verify — the manufacturer may have changed even if the drug has not.
- For supplements, prefer brands that explicitly label gluten-free and ideally carry a third-party GF certification.
- Useful reference: the website glutenfreedrugs.com maintained by a Kansas City pharmacist catalogues gluten status of common prescriptions (verify against current labeling — formulations change).
The Shared-Household Question
A diagnosis does not require everyone in the home to go gluten-free. It does require that common-use items do. A practical division:
- Shared and gluten-free by default: condiment jars, butter dish, peanut butter, the toaster you use, the colander, cutting boards, wooden utensils, the family dinner.
- Separate and allowed to contain gluten: the other household members' sandwich bread, their cereal, their pasta, their snacks — stored on a designated shelf, ideally above the gluten-free foods so crumbs cannot fall down.
- Negotiated: baking. If a household member loves to bake with wheat flour, either they agree to do it elsewhere (a friend's kitchen, a community kitchen) or the celiac member leaves the house for the duration and cleans thoroughly afterward.
Families with young celiac children often go fully gluten-free at home because small children cannot reliably manage the separation. Adults usually find partial separation workable.
Nutrient Gaps and the Processed GF Trap
Wheat flour in the U.S. is fortified with iron, folate, thiamine, riboflavin, and niacin. Gluten-free flours — rice, tapioca, potato starch — are usually not fortified. Long-term gluten-free eaters are at elevated risk for deficiencies in iron, folate, B12, B6, thiamine, riboflavin, niacin, fiber, calcium, vitamin D, magnesium, and zinc. See the sibling article on Nutritional Deficiencies and Bone Health for screening schedules and supplementation.
The other trap is the "processed gluten-free junk food" problem. Boxed GF cookies, crackers, breads, and snack bars are often built from refined rice flour and potato starch with more fat and sugar than the wheat versions they replace, and with less fiber and fewer micronutrients. Switching a diet from bread-pasta-cookies to GF bread-pasta-cookies delivers no health benefit beyond gluten avoidance and may worsen fiber intake.
The goal after the first six months of diagnosis is to rebuild the diet around naturally gluten-free whole foods: vegetables, fruit, legumes, fish, eggs, meat, dairy (if tolerated), nuts, seeds, and whole gluten-free grains like quinoa, buckwheat, millet, and brown rice. Boxed GF products become occasional convenience items, not staples.
A Sample Week
A week that covers breakfast, lunch, and dinner without boxed GF products:
- Monday. Scrambled eggs with spinach and tomatoes. Lentil soup with rice and a green salad. Baked salmon, roasted sweet potato, steamed broccoli.
- Tuesday. Greek yogurt with berries and certified GF oats. Chicken-and-rice bowl with black beans, corn, and avocado. Beef stir-fry with tamari, ginger, and garlic over rice noodles.
- Wednesday. Omelette with mushrooms and cheese. Tuna salad on corn tortillas with cucumber and olives. Roasted chicken thighs with quinoa and asparagus.
- Thursday. Smoothie with banana, spinach, almond butter, and milk. Leftover roasted chicken over mixed greens with olive oil and lemon. Pork chops with mashed potatoes and green beans.
- Friday. GF corn-flake cereal with milk and fruit. Burrito bowl: rice, pinto beans, grilled chicken, salsa, guacamole. Homemade burger (no bun or GF bun), sweet potato fries, slaw.
- Saturday. Pancakes from a certified GF flour blend with maple syrup. Rice-paper spring rolls with shrimp and peanut dipping sauce. Grilled steak, baked potato, roasted Brussels sprouts.
- Sunday. Buckwheat porridge with cinnamon and walnuts. Mexican street-corn salad with grilled chicken. Roast chicken, root vegetables, simple green salad — cook once, eat twice into Monday.
Cost and the U.S. Tax Deduction
Gluten-free packaged products in the U.S. typically cost two to four times the wheat equivalent. A loaf of GF sandwich bread runs $6–$9 against $2–$3 for ordinary bread. GF pasta is roughly double. GF cereal and crackers carry similar premiums. For a single-person household this can add $100–$300 per month to grocery bills. Shopping whole-foods-first (rice, beans, potatoes, eggs, meat, produce) blunts the difference substantially.
The U.S. tax code offers a partial offset. Under IRS Revenue Ruling 55-261 and subsequent guidance, the cost differential between a gluten-free product and its conventional equivalent is deductible as a medical expense on Schedule A, provided:
- You have a documented medical diagnosis of celiac disease from a physician (a letter stating the diagnosis is sufficient; keep it with your tax records).
- You itemize deductions, and your total unreimbursed medical expenses exceed 7.5% of adjusted gross income (only the amount above the threshold is deductible).
- You keep receipts and a running log documenting the price paid for each GF product and the price of the conventional equivalent at the same store. The deduction is the difference, not the full price.
- Shipping costs for mail-order GF foods are fully deductible.
The bookkeeping burden is the main reason most celiac patients do not bother, and in households below the 7.5% AGI threshold the deduction is useless. For households with high medical expenses in the same year — surgery, hospitalization, orthodontia — adding the GF differential can matter. Consult a tax professional; this is general information, not tax advice.
The Emotional Labor Nobody Warned You About
Six months after diagnosis, most patients have the kitchen sorted and the shopping automatic. What remains is the social cost: every birthday party, office lunch, wedding, airport layover, and family holiday is now a logistics problem. Eating alone at a restaurant is simpler than eating with six friends who want to order family-style. Saying "I have celiac disease" to a stranger at a dinner party — again — is tiring even when people are kind.
Two habits help. First, stop apologizing for the disease; it is not a preference or an inconvenience you chose. A simple, factual statement ("I have celiac, so I will order separately") closes the topic faster than explanation. Second, eat before events where you suspect the food will be unsafe. Arriving not-hungry converts the evening from a food problem to a social event.
The compliance data is clear on one point: patients who connect with other celiac patients — through local support groups, the Celiac Disease Foundation, Beyond Celiac, or online communities — stay strict longer and feel less isolated. The disease is lifelong. The community is the antidote.
Key Research Papers
- Catassi C, et al. A prospective, double-blind, placebo-controlled trial to establish a safe gluten threshold for patients with celiac disease. Aliment Pharmacol Ther. 2007. (The 20-ppm threshold evidence.)
- Pietzak M. Celiac disease, wheat allergy, and gluten sensitivity: when gluten free is not a fad. J Parenter Enteral Nutr. 2012. (Medications and gluten labeling.)
- Leffler DA, et al. Etiologies and predictors of diagnosis in nonresponsive celiac disease. Aliment Pharmacol Ther. 2015. (Restaurant gluten exposure and persistent disease.)
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on the gluten-free diet and its practical challenges:
- Gluten-free diet adherence in celiac disease
- Gluten cross-contamination in restaurants
- Certified gluten-free oats and avenin tolerance
- Nutrient deficiencies on a gluten-free diet
- The 20-ppm gluten threshold and celiac sensitivity
- Gluten-free diet and quality of life
- Gluten-free diet cost and economic burden
- Medications and gluten content in celiac patients
Connections
- Celiac Disease Overview
- Nutritional Deficiencies and Bone Health
- Dermatitis Herpetiformis
- Endoscopy, Biopsy, and Marsh Classification
- Elimination Diet
- Low-FODMAP Diet for IBS
- Diet for IBD: SCD and Mediterranean
- Irritable Bowel Syndrome
- SIBO
- Vitamin D3
- Iron
- Calcium
- Ultra-Processed Foods
- Fermented Foods
- Leaky Gut
- Food Intolerance
- Oats
- Restaurant and Travel Survival