Vitamin E Deficiency: Symptoms, Causes, and Recovery
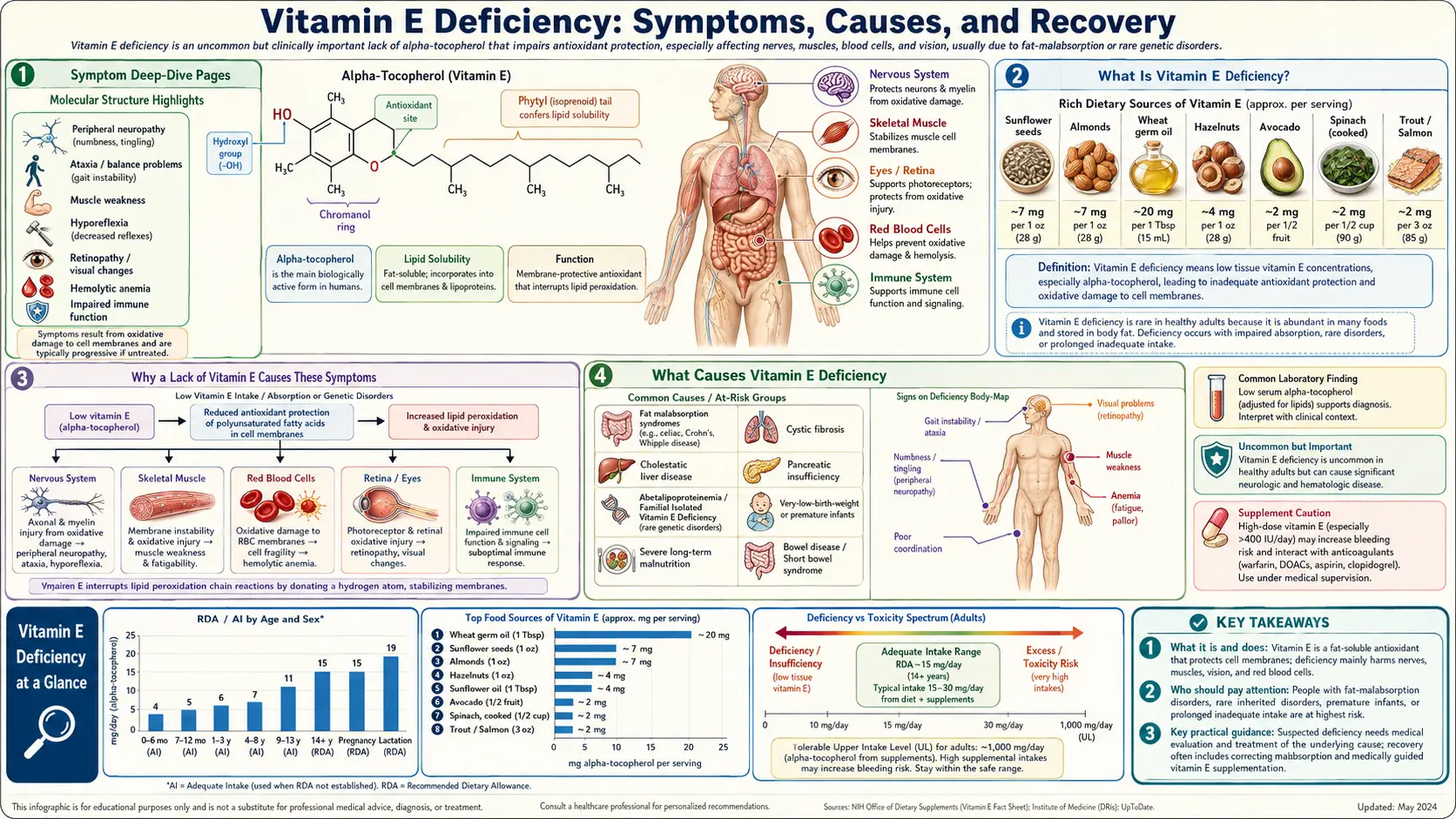
Vitamin E deficiency means your body has run low on alpha-tocopherol, the fat-soluble antioxidant that protects the delicate fatty membranes around your nerves, muscles, and red blood cells. Here is the reassuring part: in healthy adults who eat an ordinary mixed diet, a true deficiency is rare. The vitamin is stored in body fat and the liver, and it is plentiful in nuts, seeds, and plant oils. When deficiency does happen, it is almost always because the gut cannot absorb fat properly — in conditions such as cystic fibrosis, Crohn's or celiac disease, liver and bile-duct disease, or rare inherited problems with the protein that ships vitamin E around the body — or in premature babies, who are born with very little. Because vitamin E guards nerve and muscle membranes, a long-standing shortage shows up mainly as a slow, creeping neurological problem: numb or tingling feet, an unsteady, off-balance walk (ataxia), lost reflexes, muscle weakness, and sometimes trouble with vision. In newborns it can also pop red blood cells, causing a mild anemia. The good news is that, caught in time, much of this is preventable and treatable with vitamin E replacement. This hub explains what the deficiency is, why one missing vitamin causes these particular symptoms, who is actually at risk, how it is diagnosed, and exactly how it is corrected — with deep-dive pages for each of the major symptoms.
Symptom Deep-Dive Pages
Nerve Damage & Ataxia
The signature problem of long-standing vitamin E deficiency: numb, tingling feet, an unsteady wide-based walk, and lost reflexes. Why the longest nerves and the balance pathways fail first, and how much recovers with treatment.
Muscle Weakness
How a shortage of this membrane-protecting antioxidant can produce a true myopathy — weak, achy muscles — what it feels like, how it is told apart from other causes, and why strength tends to return once levels are restored.
Hemolytic Anemia
Why low vitamin E makes red blood cells fragile and prone to bursting, the classic picture in premature infants, and why this is one of the few quickly reversible parts of the deficiency.
Vision Problems
The retina is rich in the same fragile fats vitamin E protects. How severe, prolonged deficiency can damage the retina (a pigmentary retinopathy), what the early changes look like, and when to have eyes checked.
Table of Contents
- Symptom Deep-Dive Pages
- What Is Vitamin E Deficiency?
- Why a Lack of Vitamin E Causes These Symptoms
- What Causes Vitamin E Deficiency
- Who Is at Risk
- How Vitamin E Deficiency Is Diagnosed
- How Vitamin E Deficiency Is Corrected
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Is Vitamin E Deficiency?
"Vitamin E" is the name for a family of eight related fat-soluble compounds — four tocopherols and four tocotrienols — but for human health the one that matters most is alpha-tocopherol. It is the body's most important fat-soluble antioxidant: its single job is to protect the fatty parts of your cells from a kind of chemical rust called lipid peroxidation. Vitamin E deficiency simply means your tissues have run low on alpha-tocopherol, usually defined by a blood level below roughly 5 micrograms per milliliter (about 11.6 micromoles per liter) in adults — though, as explained under diagnosis, the number is interpreted alongside blood fats rather than read in isolation.
The first thing to understand is that true vitamin E deficiency is uncommon in healthy people. Three facts make it hard to become deficient by diet alone:
- The vitamin is stored. Being fat-soluble, alpha-tocopherol is held in body fat and the liver, building a reserve that buffers you through periods of lower intake. You do not run out in days or weeks the way you can with some water-soluble vitamins.
- It is widespread in ordinary food. Nuts, seeds, and vegetable oils are rich sources, and smaller amounts are in leafy greens, avocado, and many other foods. A normal mixed diet usually supplies enough to avoid overt deficiency, even if many people fall short of the optimal recommended intake.
- The body conserves it. A liver protein called the alpha-tocopherol transfer protein (α-TTP) selectively recycles alpha-tocopherol back into the bloodstream, preferentially keeping this one form in circulation.
So when a real deficiency appears, it is a signal that something specific is wrong — nearly always a problem absorbing dietary fat, a problem handling the vitamin once absorbed, or being born without a reserve. Because the damage builds slowly over months to years, the clinical picture is dominated not by a sudden illness but by a gradual neurological syndrome: a "dying back" of the longest nerves and the spinal pathways that carry position sense and coordinate movement. The result is a fairly recognizable pattern — numbness and tingling in the feet, lost ankle reflexes, an unsteady wide-based gait (ataxia), muscle weakness, and, in severe long-standing cases, eye changes. In premature infants the picture is different: there, the most visible effect is fragile red blood cells and a mild hemolytic anemia. Each of these is covered in depth on its own page above.
Why a Lack of Vitamin E Causes These Symptoms
The puzzle is why a shortage of one antioxidant causes these particular problems — unsteady walking, numb feet, weak muscles, fragile blood cells — and not something else entirely. The answer comes down to a single idea: vitamin E protects fat, and the tissues that suffer are the ones built from the most vulnerable fat.
Here is the mechanism in everyday language. Every cell is wrapped in a membrane made largely of fats called polyunsaturated fatty acids. These fats are flexible and essential, but their chemistry makes them easy targets for free radicals — unstable molecules, produced as a normal by-product of using oxygen for energy, that snatch electrons from whatever is nearby. When a free radical attacks a membrane fat, it starts a self-feeding chain reaction (lipid peroxidation): one damaged fat damages the next, like a row of dominoes, until the membrane is riddled with chemical "rust." Vitamin E is the firebreak. It sits inside the membrane, intercepts the free radical, and stops the chain before it spreads — sacrificing itself in the process (and then often being recharged by vitamin C). Remove the firebreak, and membranes slowly accumulate oxidative damage.
That single fact explains the whole pattern, because the tissues that fail are precisely the ones whose work depends on intact, fat-rich membranes — and which cannot easily replace themselves:
- Long nerves and the spinal cord (the dominant problem). Nerve cells are exquisitely membrane-dependent, and the very long fibers running to the feet and the large position-sense fibers in the spinal cord's dorsal columns are the most exposed of all — they are long, have a lot of membrane to protect, and renew themselves poorly. Over years of unchecked oxidation they degenerate from the far end inward (a "dying-back" neuropathy). This is why the classic deficiency shows up as numb, tingling feet, lost reflexes, and ataxia — the unsteady, wide-based walk that comes from losing the brain's sense of where the limbs are in space. (Deep dive: Nerve Damage & Ataxia; see also Peripheral Neuropathy.)
- Muscle. Muscle fibers have extensive membranes and burn a great deal of oxygen, so they too are vulnerable to oxidative injury. Deficiency can cause a true myopathy — weak, sometimes achy muscles — with telltale leakage of muscle enzymes into the blood. (Deep dive: Muscle Weakness.)
- Red blood cells. A red cell is essentially a soft bag of membrane, and it is hammered with oxygen on every trip through the lungs. Without enough vitamin E the membrane becomes fragile and the cells rupture (hemolysis) sooner than they should. Newborns — especially premature ones with almost no stores — are most susceptible, producing a mild hemolytic anemia. (Deep dive: Hemolytic Anemia.)
- The retina. The light-sensing layer at the back of the eye is among the most fat-rich, oxygen-exposed tissues in the body. Severe, prolonged deficiency can damage it, producing a pigmentary retinopathy and vision changes. (Deep dive: Vision Problems.)
So there is nothing mysterious about the syndrome. One antioxidant defends fatty membranes; the membranes that matter most for movement, strength, blood, and sight are the ones built from the most oxidation-prone fat; and so a long shortage is felt first and worst in the nerves and, in the very young, the blood. For more on why this antioxidant role is the heart of vitamin E's biology, see the Vitamin E overview and the broader topic of Oxidative Stress.
What Causes Vitamin E Deficiency
Because the body stores vitamin E and food supplies it readily, deficiency rarely comes from eating too little. Instead it almost always comes from a problem getting the vitamin out of food and into the body, or from being born without a reserve. Vitamin E is fat-soluble, so anything that interferes with digesting and absorbing dietary fat will, given time, interfere with vitamin E. Here are the causes worth knowing.
- Fat-malabsorption disorders (the largest group). To absorb vitamin E you need to digest fat, which requires pancreatic enzymes and bile. Conditions that disrupt this lead the field of causes: cystic fibrosis (where thick secretions block pancreatic enzymes), Crohn's disease and other inflammatory bowel disease, celiac disease, chronic pancreatitis, short-bowel syndrome (after large bowel resections), and bariatric (weight-loss) surgery that bypasses part of the gut.
- Liver and bile-duct disease (cholestasis). If bile cannot reach the intestine — as in chronic cholestatic liver disease, biliary atresia, or prolonged blockage of the bile ducts — fat and the fat-soluble vitamins are poorly absorbed. This is a particularly important and well-documented cause in children, where the resulting neurological syndrome was first carefully described (see the Sokol papers below).
- Prematurity. A baby builds its vitamin E stores mostly in the last weeks of pregnancy. Babies born early arrive with very little reserve and an immature gut, leaving them prone to deficiency — classically showing up as a hemolytic anemia in the first weeks of life.
- Rare inherited disorders of vitamin E handling. Two genetic conditions cause deficiency even when fat absorption is normal. Ataxia with Vitamin E Deficiency (AVED) is caused by mutations in the gene for the alpha-tocopherol transfer protein (α-TTP); without that protein, the liver cannot keep alpha-tocopherol in circulation, and a progressive ataxia results. Abetalipoproteinemia is a defect in packaging fat into lipoproteins, which blocks the transport of fat-soluble vitamins out of the gut and causes severe early deficiency. Both are rare but important, because high-dose vitamin E can prevent or slow the neurological damage.
- Other fat-blocking factors. Long-term use of medications or products that reduce fat absorption (for example, the weight-loss/fat-blocking agent orlistat, or chronic high intake of non-absorbable fat substitutes) can lower the absorption of fat-soluble vitamins and contribute to deficiency over time.
- Severe, prolonged malnutrition. Genuinely inadequate intake can deplete vitamin E, but in practice this matters mainly in the setting of overall starvation, very-low-fat diets sustained for long periods, or famine — not in someone simply eating a typical Western diet, which tends to fall short of optimal but rarely to the point of overt deficiency.
A practical note: these causes often share a theme. Whenever the gut cannot handle fat — whether from the pancreas, the bile, the bowel wall, or a genetic transport defect — vitamin E (along with vitamins A, D, and K) tends to fall together. That is why doctors who find one fat-soluble vitamin low will often check the others.
Who Is at Risk
It helps to turn the causes around and ask: who actually develops this? For the vast majority of people the honest answer is — they do not. Overt vitamin E deficiency is genuinely rare in the general population. The people who need to think about it fall into a few clear groups.
- People with fat-malabsorption conditions. This is the single most important group: anyone living with cystic fibrosis, inflammatory bowel disease, celiac disease, chronic pancreatitis, or cholestatic liver disease, and anyone who has had significant bowel surgery or a malabsorptive weight-loss operation. In these people, monitoring fat-soluble vitamins is routine.
- Premature and very-low-birth-weight infants. Born before they could stock up, and with immature digestion, these babies are the classic at-risk newborns. Neonatal units pay close attention to their vitamin E status.
- People with the rare inherited disorders AVED or abetalipoproteinemia — often suspected when a young person develops a progressive ataxia or neuropathy, especially with a family history or with very low vitamin E despite a normal diet.
- People on long-term fat-blocking medication (such as orlistat) without attention to fat-soluble vitamin intake.
- People with severe, prolonged undernutrition.
Two groups deserve a reassuring word. Healthy adults eating an ordinary diet are not meaningfully at risk of the deficiency syndrome described here, even though surveys suggest many of us get less than the ideal amount of vitamin E — that gap is about long-term optimal intake, not the dramatic neurological deficiency. And while older adults can have lower intakes, age by itself does not commonly produce overt deficiency in the absence of one of the conditions above. If you do not have a malabsorption problem and you eat foods like almonds, walnuts, seeds, and plant oils, your risk is low.
How Vitamin E Deficiency Is Diagnosed
Diagnosis rests on a simple blood test — a serum alpha-tocopherol level — interpreted in light of the clinical picture and, importantly, your blood fats. It is not part of a routine check-up; a doctor orders it when there is a reason to suspect deficiency, such as a known malabsorption condition or an unexplained neurological syndrome of numb feet, imbalance, and lost reflexes.
Here is what goes into making the diagnosis:
- Serum alpha-tocopherol. The core test. A level below roughly 5 µg/mL (about 11.6 µmol/L) in an adult indicates deficiency. Results are usually quick and the test is widely available; it is the same measurement used to confirm a suspected case and to track recovery during treatment.
- The vitamin E–to–lipid ratio (the key refinement). Because vitamin E travels through the blood riding on fat-carrying lipoproteins, the serum level rises and falls with your blood fats. Someone with very high or very low cholesterol and triglycerides can have a misleading raw number. To correct for this, the alpha-tocopherol level is divided by the total of cholesterol plus triglycerides (or by total lipids). A ratio below about 0.8 mg of alpha-tocopherol per gram of total lipid is the most reliable indicator of true deficiency, especially in people with abnormal blood fats — which is common in liver disease and in abetalipoproteinemia. This is why a Lipid Panel is often drawn alongside the vitamin E level.
- Looking for the cause. Once deficiency is confirmed, the work-up turns to why. Depending on the picture this may include tests of fat absorption, liver and bile-duct evaluation, screening for celiac disease, and — in a young person with progressive ataxia and very low vitamin E despite normal fat handling — genetic testing for AVED. A Comprehensive Metabolic Panel helps assess liver function, and the other fat-soluble vitamins (A, D, K) are frequently checked because they tend to fall together.
- Assessing the consequences. If symptoms are present, a doctor may add tests to gauge the damage: nerve conduction studies for the neuropathy, muscle enzyme levels (creatine kinase) and sometimes electromyography for suspected myopathy, an eye examination for retinal changes, and a Complete Blood Count with a look at red-cell fragility in infants suspected of hemolytic anemia.
The take-home point: a single vitamin E number can mislead if blood fats are abnormal, so the diagnosis is made by reading the level in context — ideally as a ratio to total lipids — and then hunting down the underlying reason.
How Vitamin E Deficiency Is Corrected
The encouraging news is that vitamin E deficiency is treatable, and the principles are straightforward: replace the vitamin in a form the person can actually absorb, in a dose matched to the cause, treat the underlying problem, and start early — because some nerve damage, once established, may not fully reverse.
- For people without malabsorption — food and ordinary supplements. When intake alone is the (uncommon) issue, a vitamin E–rich diet usually suffices, and it supports health in other ways too. The richest sources are nuts, seeds, and plant oils: a handful of almonds or sunflower seeds, walnuts, olive oil and other vegetable oils, plus smaller contributions from spinach and leafy greens, avocado, and wheat germ. For context, the adult Recommended Dietary Allowance is 15 mg (about 22 IU of natural alpha-tocopherol) per day. The fuller food list is on the Vitamin E overview.
- For fat-malabsorption — higher doses and water-miscible forms. This is the heart of treatment, because the problem is absorption, not intake. People with cystic fibrosis, cholestatic liver disease, and similar conditions are given larger oral doses and, crucially, special water-soluble (water-miscible) preparations — most notably TPGS (d-alpha-tocopheryl polyethylene glycol 1000 succinate), a form designed to be absorbed even when bile and fat digestion are impaired. TPGS was a genuine advance for treating these patients, allowing vitamin E to get in when ordinary oil-based capsules cannot. Doses are individualized and guided by repeat blood levels.
- For the rare inherited disorders — lifelong high-dose vitamin E. In AVED and abetalipoproteinemia, large daily doses of vitamin E are the cornerstone of care, often for life. Started early, this can prevent the neurological disease from developing or halt its progression — one of the clearest examples in medicine of a vitamin literally preventing irreversible nerve damage.
- For premature infants — careful supplementation. Vitamin E is given under neonatal supervision to correct and prevent the hemolytic anemia of prematurity, with attention to the right dose, since both too little and too much can be problematic in tiny infants.
- Always: treat the underlying cause. Replacing vitamin E without addressing why it ran low only delays the next shortfall. That might mean optimizing pancreatic enzyme replacement in cystic fibrosis, controlling inflammatory bowel disease, managing the liver or biliary problem, or adjusting a fat-blocking medication.
How much recovers depends largely on timing. The fragile red cells of hemolytic anemia bounce back quickly once vitamin E is restored. The neurological syndrome is different: caught early, symptoms can stabilize and substantially improve, but a long-untreated, advanced neuropathy and ataxia may only partly recover — which is the strongest argument for finding and correcting the deficiency before the damage is entrenched. A doctor follows treatment with periodic blood levels (read as a ratio to lipids) to confirm the vitamin is finally getting in.
When to Seek Care / Red Flags
Vitamin E deficiency develops slowly, so it rarely produces a sudden emergency the way some problems do. The more useful message is about not ignoring the early, treatable stage — because nerve damage is far easier to prevent than to reverse. Contact your doctor promptly to be evaluated if you notice any of the following, especially if you have a condition that affects fat absorption:
- New numbness, tingling, or "pins and needles" in the feet — particularly if it is creeping upward over weeks to months, the typical pattern of a nutritional neuropathy.
- Unsteadiness or loss of balance — feeling wobbly on your feet, a wide-based or clumsy walk, more stumbling or falls, or difficulty in the dark when you cannot use vision to compensate. Progressive ataxia always deserves medical evaluation.
- Muscle weakness — difficulty rising from a chair, climbing stairs, or lifting things, especially with muscle aching, which may point to a myopathy.
- Changes in vision — trouble seeing in dim light or a sense of narrowing side vision, which can signal retinal involvement in severe, long-standing deficiency.
- Known malabsorption and missed monitoring — if you have cystic fibrosis, cholestatic liver disease, celiac or Crohn's disease, or have had bowel or weight-loss surgery and have not had your fat-soluble vitamins checked, ask about it. Catching a low level before symptoms appear is the whole point.
For parents: a premature baby's care team monitors for the anemia of vitamin E deficiency, but report unusual pallor or poor feeding so it can be evaluated. The reason to act on these signs early is simple — the deficiency is treatable, and the nervous system rewards early treatment. For related symptoms, see Peripheral Neuropathy and the Anemia overview.
Key Research Papers
- Traber MG (2014). Vitamin E Inadequacy in Humans: Causes and Consequences. Advances in Nutrition;5(5):503-514. — DOI: 10.3945/an.114.006254
- Traber MG, Atkinson J (2007). Vitamin E, antioxidant and nothing more. Free Radical Biology and Medicine;43(1):4-15. — DOI: 10.1016/j.freeradbiomed.2007.03.024
- Muller DPR (2010). Vitamin E and neurological function. Molecular Nutrition & Food Research;54(5):710-718. — DOI: 10.1002/mnfr.200900460
- Kayden HJ, Traber MG (1999). Molecular Mechanisms of Vitamin E Transport. Annual Review of Nutrition;19:343-355. — DOI: 10.1146/annurev.nutr.19.1.343
- Kayden HJ, Traber MG (1993). Absorption, lipoprotein transport, and regulation of plasma concentrations of vitamin E in humans. Journal of Lipid Research;34(3):343-358. — DOI: 10.1016/s0022-2275(20)40727-8
- Sokol RJ, Heubi JE, Iannaccone ST, Bove KE, Balistreri WF (1983). Mechanism Causing Vitamin E Deficiency During Chronic Childhood Cholestasis. Gastroenterology;85(5):1172-1182. — DOI: 10.1016/s0016-5085(83)80087-0
- Sokol RJ, Guggenheim MA, Iannaccone ST, Barkhaus PE, Miller C, et al. (1985). Frequency and Clinical Progression of the Vitamin E Deficiency Neurologic Disorder in Children With Prolonged Neonatal Cholestasis. American Journal of Diseases of Children;139(12):1211-1215. — DOI: 10.1001/archpedi.1985.02140140045024
- Schuelke M, Mayatepek E, Inter M, Becker M, Pfeiffer E, et al. (1999). Treatment of ataxia in isolated vitamin E deficiency caused by alpha-tocopherol transfer protein deficiency. The Journal of Pediatrics;134(2):240-244. — DOI: 10.1016/s0022-3476(99)70424-5
- Oski FA, Barness LA (1967). Vitamin E deficiency: a previously unrecognized cause of hemolytic anemia in the premature infant. The Journal of Pediatrics;70(2):211-220. — DOI: 10.1016/s0022-3476(67)80416-5
- Ritchie JH, Fish MB, McMasters V, Grossman M (1968). Edema and Hemolytic Anemia in Premature Infants — A Vitamin E Deficiency Syndrome. New England Journal of Medicine;279(22):1185-1190. — DOI: 10.1056/nejm196811282792202
- Traber MG (2021). Vitamin E: How much is enough, too much and why! Free Radical Biology and Medicine;177:212-225. — DOI: 10.1016/j.freeradbiomed.2021.10.028
- National Institutes of Health, Office of Dietary Supplements (2021). Vitamin E — Health Professional Fact Sheet. — NIH ODS Fact Sheet
PubMed Topic Searches
- PubMed — Vitamin E deficiency: neuropathy and ataxia
- PubMed — Vitamin E deficiency and fat malabsorption
- PubMed — Ataxia with vitamin E deficiency (AVED)
- PubMed — Vitamin E deficiency and hemolytic anemia in premature infants
- PubMed — Vitamin E deficiency diagnosis and the tocopherol/lipid ratio
Connections
- Vitamin E Deficiency: Nerve Damage & Ataxia
- Vitamin E Deficiency: Muscle Weakness
- Vitamin E Deficiency: Hemolytic Anemia
- Vitamin E Deficiency: Vision Problems
- Vitamin E Overview
- Vitamin E Toxicity
- Vitamin E Benefits Hub
- Vitamin A
- Vitamin C
- Vitamin K2
- Selenium
- Oxidative Stress
- Antioxidants
- Lipid Panel
- Comprehensive Metabolic Panel
- Complete Blood Count
- Peripheral Neuropathy
- Anemia
- Cystic Fibrosis
- Celiac Disease
- Crohn's Disease
- Almonds
- Walnuts
- Olive Oil
- Spinach
- Avocado