Peripheral Neuropathy
1. Overview
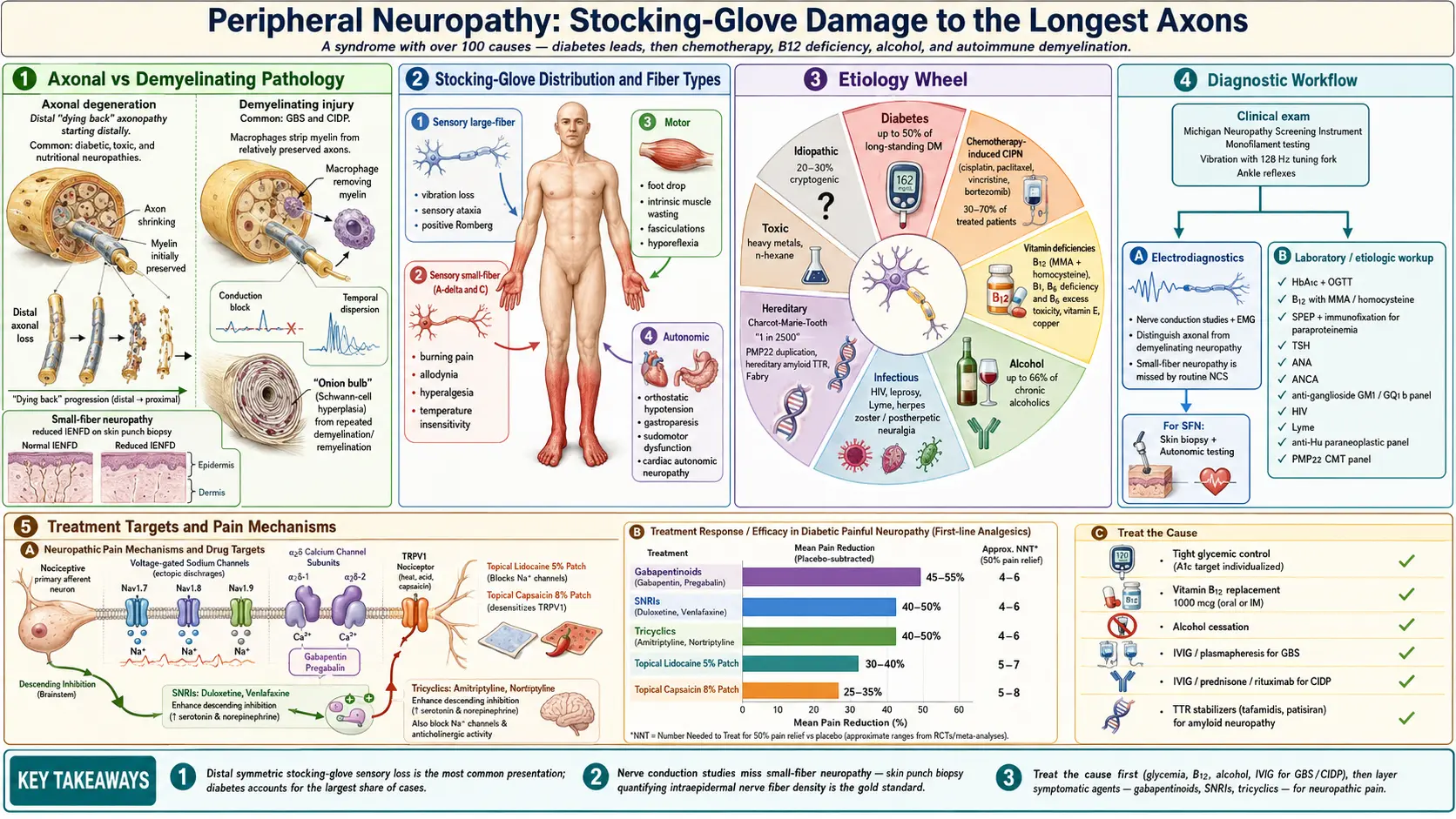
Peripheral neuropathy refers to damage or dysfunction of one or more peripheral nerves, resulting in weakness, numbness, pain, and autonomic dysfunction, typically affecting the hands and feet in a "stocking-glove" distribution. The peripheral nervous system connects the brain and spinal cord to the muscles, skin, internal organs, and glands, and its damage can disrupt motor, sensory, and autonomic functions. Peripheral neuropathy is not a single disease but rather a syndrome with over 100 identified causes.
The condition can affect a single nerve (mononeuropathy), two or more nerves in separate areas (mononeuropathy multiplex), or many nerves simultaneously (polyneuropathy). It can also be classified by the type of nerve fiber affected: motor neuropathy (affecting movement), sensory neuropathy (affecting sensation), autonomic neuropathy (affecting involuntary functions), or mixed neuropathy (affecting combinations of fiber types). The most common form is a distal symmetric sensorimotor polyneuropathy.
Peripheral neuropathy is further classified by the underlying pathological process:
- Axonal neuropathy — primary degeneration of the nerve axon; the most common type; includes metabolic, toxic, and many hereditary neuropathies
- Demyelinating neuropathy — primary damage to the myelin sheath surrounding nerve fibers; includes Guillain-Barre syndrome (GBS) and chronic inflammatory demyelinating polyneuropathy (CIDP)
- Mixed axonal-demyelinating neuropathy — features of both processes; seen in many chronic neuropathies
- Neuronopathy (ganglionopathy) — damage to the nerve cell body in the dorsal root ganglion; associated with paraneoplastic syndromes and Sjogren syndrome
2. Epidemiology
Peripheral neuropathy is one of the most common neurological conditions encountered in clinical practice, affecting approximately 2-8% of the general population. The prevalence increases significantly with age, rising to 8-15% in individuals over 55 years. In the United States alone, an estimated 20 million people are affected by some form of peripheral neuropathy.
Diabetic neuropathy is by far the most common cause in developed countries, affecting approximately 50% of patients with long-standing diabetes mellitus. Among patients with type 2 diabetes, approximately 10-15% have neuropathy at the time of diagnosis. Chemotherapy-induced peripheral neuropathy (CIPN) affects 30-70% of patients receiving neurotoxic chemotherapy agents, depending on the drug, dose, and duration. HIV-associated neuropathy affects approximately 30-67% of HIV-infected individuals, either from the virus itself or antiretroviral medications.
Hereditary neuropathies, collectively known as Charcot-Marie-Tooth (CMT) disease, have a prevalence of approximately 1 in 2,500 people, making them the most common inherited neurological disorders. Guillain-Barre syndrome (GBS) has an annual incidence of 1-2 per 100,000, while chronic inflammatory demyelinating polyneuropathy (CIDP) has a prevalence of approximately 1-9 per 100,000. Despite extensive workup, the cause of peripheral neuropathy remains unidentified in approximately 20-30% of cases, termed idiopathic or cryptogenic neuropathy.
3. Pathophysiology
The pathophysiology of peripheral neuropathy varies by etiology but involves several key mechanisms that damage peripheral nerve components including axons, myelin sheaths, Schwann cells, dorsal root ganglia, and vasa nervorum.
Axonal Degeneration
Axonal neuropathies involve primary degeneration of the nerve axon, typically beginning distally and progressing proximally in a pattern known as "dying back" neuropathy. This occurs because the most distal portions of long axons are most vulnerable to metabolic insults due to their distance from the neuronal cell body and high energy demands for axonal transport. In diabetic neuropathy, chronic hyperglycemia activates the polyol pathway (aldose reductase converts glucose to sorbitol, causing osmotic stress), the hexosamine pathway, protein kinase C activation, and advanced glycation end-products (AGEs) formation, collectively causing oxidative stress, mitochondrial dysfunction, and axonal degeneration.
Demyelination
Demyelinating neuropathies result from damage to the myelin sheath or Schwann cells, causing slowing of nerve conduction velocity, conduction block, and temporal dispersion. In immune-mediated demyelinating neuropathies such as GBS and CIDP, autoantibodies and autoreactive T cells target myelin components including myelin protein zero (MPZ), peripheral myelin protein 22 (PMP22), myelin-associated glycoprotein (MAG), and gangliosides (GM1, GD1a, GQ1b). Macrophage-mediated stripping of myelin from the axon is a hallmark histological finding. If the underlying axon is preserved, remyelination and recovery can occur, but repeated demyelination leads to secondary axonal degeneration ("onion bulb" formation).
Vascular Mechanisms
Damage to the vasa nervorum (the small blood vessels supplying peripheral nerves) causes ischemic nerve injury. This is the primary mechanism in vasculitic neuropathy, where inflammation of the vasa nervorum leads to nerve infarction, typically presenting as mononeuropathy multiplex. In diabetic neuropathy, microvascular disease contributes to ischemic damage of nerve fibers through endothelial dysfunction, basement membrane thickening, and reduced endoneurial blood flow.
Ion Channel and Receptor Dysfunction
Neuropathic pain results from aberrant expression and function of voltage-gated sodium channels (Nav1.7, Nav1.8, Nav1.9) in damaged sensory neurons, leading to ectopic firing and peripheral sensitization. Upregulation of alpha-2-delta calcium channel subunits at dorsal root ganglia and spinal cord contributes to central sensitization, forming the therapeutic target for gabapentinoids. Transient receptor potential (TRP) channels, particularly TRPV1 and TRPA1, become hyperactive in injured nociceptors, contributing to heat and chemical hypersensitivity.
Small Fiber Pathology
Small fiber neuropathy (SFN) selectively damages thinly myelinated A-delta and unmyelinated C fibers, which carry pain, temperature, and autonomic signals. The pathology involves degeneration of intraepidermal nerve fibers (IENFs), quantified by skin punch biopsy. Causes include diabetes and prediabetes, Sjogren syndrome, sarcoidosis, Fabry disease, and gain-of-function mutations in Nav1.7 (SCN9A), Nav1.8 (SCN10A), and Nav1.9 (SCN11A) sodium channels.
4. Etiology and Risk Factors
Metabolic and Endocrine Causes
- Diabetes mellitus — the most common cause; affects up to 50% of diabetic patients
- Prediabetes and metabolic syndrome — increasingly recognized as a cause of sensory and small fiber neuropathy
- Chronic kidney disease (uremia) — affects 60-90% of dialysis patients
- Hypothyroidism — can cause carpal tunnel syndrome and polyneuropathy
- Vitamin deficiencies — B12 (most common), B1 (thiamine/beriberi), B6 (pyridoxine), E, and copper
- Vitamin B6 excess — toxicity from megadose supplementation causes sensory neuronopathy
Toxic Causes
- Alcohol — direct neurotoxicity combined with nutritional deficiency; affects up to 66% of chronic alcoholics
- Chemotherapy agents — platinum compounds (cisplatin, oxaliplatin), taxanes (paclitaxel, docetaxel), vinca alkaloids (vincristine), bortezomib, thalidomide
- Other medications — amiodarone, metronidazole, nitrofurantoin, isoniazid, statins (controversial), fluoroquinolones
- Heavy metals — lead (motor predominant), arsenic, thallium, mercury
- Industrial solvents — n-hexane, acrylamide, carbon disulfide
Immune-Mediated and Inflammatory Causes
- Guillain-Barre syndrome (GBS) — acute inflammatory demyelinating polyneuropathy; often post-infectious
- Chronic inflammatory demyelinating polyneuropathy (CIDP) — chronic counterpart of GBS
- Multifocal motor neuropathy (MMN) — pure motor neuropathy with conduction block; anti-GM1 antibodies
- Vasculitic neuropathy — polyarteritis nodosa, granulomatosis with polyangiitis, eosinophilic granulomatosis with polyangiitis
- Paraproteinemic neuropathy — associated with monoclonal gammopathy (MGUS, myeloma, Waldenstrom macroglobulinemia, amyloidosis)
- Sarcoidosis — can cause cranial neuropathies, small fiber neuropathy, or polyneuropathy
- Sjogren syndrome — sensory neuronopathy, small fiber neuropathy, or trigeminal neuropathy
Infectious Causes
- HIV/AIDS — distal symmetric polyneuropathy, inflammatory demyelinating neuropathy
- Herpes zoster (shingles) — postherpetic neuralgia
- Leprosy (Hansen disease) — the most common infectious cause of neuropathy worldwide
- Lyme disease (Borrelia burgdorferi) — cranial neuropathy, radiculopathy, mononeuropathy multiplex
- Hepatitis B and C — associated with cryoglobulinemic vasculitic neuropathy
- Diphtheria — toxin-mediated demyelinating neuropathy
Hereditary Causes
- Charcot-Marie-Tooth disease (CMT) — the most common inherited neuropathy; multiple subtypes (CMT1A due to PMP22 duplication is most prevalent)
- Hereditary neuropathy with liability to pressure palsies (HNPP) — PMP22 deletion
- Familial amyloid polyneuropathy (FAP) — transthyretin (TTR) mutations
- Fabry disease — X-linked alpha-galactosidase A deficiency causing small fiber neuropathy
- Hereditary sensory and autonomic neuropathies (HSAN) — types I-V
Other Causes
- Compression and entrapment — carpal tunnel syndrome (median nerve), ulnar neuropathy at the elbow, peroneal neuropathy at the fibular head
- Paraneoplastic — anti-Hu (ANNA-1) antibodies causing sensory neuronopathy, typically associated with small cell lung cancer
- Critical illness polyneuropathy — axonal neuropathy developing during prolonged ICU stays
- Radiation-induced plexopathy — delayed complication of radiation therapy
5. Clinical Presentation
Sensory Symptoms
- Numbness and tingling (paresthesias) — typically beginning in the toes and feet, gradually ascending to involve the ankles, calves, and eventually the fingertips in a stocking-glove pattern
- Burning, stabbing, or shooting pain — neuropathic pain is present in approximately 40-60% of patients with polyneuropathy
- Allodynia — pain from normally non-painful stimuli such as light touch or clothing contact
- Hyperalgesia — exaggerated pain response to mildly painful stimuli
- Loss of vibration and proprioception — impaired large fiber function causing unsteadiness, particularly in the dark
- Temperature insensitivity — inability to detect hot and cold, increasing burn and frostbite risk
- Sensory ataxia — impaired proprioception causing wide-based gait and positive Romberg sign
Motor Symptoms
- Distal weakness — foot drop (ankle dorsiflexion weakness), difficulty with fine motor tasks (buttons, zippers)
- Muscle atrophy — visible wasting of intrinsic foot and hand muscles
- Cramping — painful involuntary muscle contractions, especially in the calves
- Fasciculations — muscle twitching visible under the skin
- Impaired gait — steppage gait due to foot drop; wide-based gait due to sensory ataxia
- Hyporeflexia or areflexia — diminished or absent deep tendon reflexes, typically ankle jerks lost first
Autonomic Symptoms
- Orthostatic hypotension — lightheadedness or syncope upon standing
- Gastroparesis — nausea, bloating, early satiety, erratic glucose control in diabetics
- Bladder dysfunction — urinary retention, incontinence, frequent urinary tract infections
- Sexual dysfunction — erectile dysfunction in men; vaginal dryness in women
- Sudomotor dysfunction — anhidrosis (absent sweating) distally with compensatory hyperhidrosis proximally
- Pupillary abnormalities — impaired pupillary light reflex
- Cardiac autonomic neuropathy — resting tachycardia, loss of heart rate variability, increased risk of cardiac arrhythmias and sudden death
Patterns by Neuropathy Type
- Distal symmetric polyneuropathy — the most common pattern; gradual, symmetric, length-dependent, sensory-predominant
- Mononeuropathy — single nerve involvement; carpal tunnel syndrome (median nerve) is the most common
- Mononeuropathy multiplex — asymmetric involvement of multiple individual nerves; suggests vasculitis, diabetes, or sarcoidosis
- Polyradiculoneuropathy — involvement of nerve roots and peripheral nerves; suggests GBS or CIDP
6. Diagnosis
A systematic diagnostic approach is essential given the wide range of possible etiologies. History and physical examination narrow the differential before targeted testing.
Clinical Assessment
- Detailed history — onset pattern (acute, subacute, chronic), progression, distribution, associated symptoms, medications, toxin exposures, alcohol use, family history, occupational history
- Neurological examination — sensory testing (light touch, pinprick, vibration with 128 Hz tuning fork, proprioception, temperature), motor testing (strength grading, atrophy, fasciculations), reflex testing, gait assessment, Romberg test
- Validated screening tools — Michigan Neuropathy Screening Instrument (MNSI), Toronto Clinical Neuropathy Score, Total Neuropathy Score
Electrodiagnostic Studies
- Nerve conduction studies (NCS) — measure motor and sensory nerve conduction velocities, amplitudes, and latencies; distinguish axonal (reduced amplitudes) from demyelinating (slowed velocities, prolonged latencies, conduction block, temporal dispersion) neuropathies
- Electromyography (EMG) — assesses muscle denervation and reinnervation; helps localize lesions and determine chronicity
- Note — NCS/EMG evaluates only large myelinated fibers; small fiber neuropathy requires alternative testing
Laboratory Evaluation
Initial screening panel:
- Fasting glucose, hemoglobin A1c, oral glucose tolerance test
- Complete blood count, comprehensive metabolic panel
- Vitamin B12 with methylmalonic acid and homocysteine levels
- Thyroid-stimulating hormone (TSH)
- Serum protein electrophoresis (SPEP) with immunofixation
- Erythrocyte sedimentation rate (ESR), C-reactive protein (CRP)
Expanded testing based on clinical suspicion:
- Autoimmune — ANA, ANCA, anti-SSA/SSB, cryoglobulins, complement levels, anti-ganglioside antibodies (GM1, GD1a, GQ1b), anti-MAG antibodies
- Infectious — HIV, hepatitis B and C, Lyme titers, RPR/VDRL
- Nutritional — copper, zinc, thiamine, vitamin E, folate levels
- Genetic — PMP22 gene duplication/deletion, CMT gene panels, TTR sequencing for amyloidosis
- Paraneoplastic — anti-Hu (ANNA-1), anti-CV2/CRMP5 antibodies
- Urine — 24-hour urine for heavy metals, Bence Jones protein
Specialized Testing
- Skin punch biopsy — measures intraepidermal nerve fiber density (IENFD); the gold standard for diagnosing small fiber neuropathy; abnormal values are below age- and gender-matched normative thresholds
- Nerve biopsy (sural nerve) — reserved for cases of suspected vasculitis, amyloidosis, leprosy, or sarcoidosis; provides histological diagnosis but causes permanent sensory deficit
- Autonomic testing — quantitative sudomotor axon reflex test (QSART), thermoregulatory sweat test, cardiovascular autonomic reflex testing, tilt-table testing
- MRI neurography — high-resolution imaging of peripheral nerves and plexuses; useful for detecting focal nerve enlargement, inflammation, or compression
- Nerve ultrasound — increasingly used to visualize nerve swelling in entrapment neuropathies and CIDP; can measure cross-sectional area of nerves
- Lumbar puncture — elevated CSF protein (albuminocytologic dissociation) in GBS and CIDP
7. Treatment
Treatment focuses on three pillars: addressing the underlying cause, managing neuropathic pain, and providing supportive care and rehabilitation.
Treating Underlying Causes
- Diabetic neuropathy — strict glycemic control (HbA1c target typically below 7%); shown to reduce neuropathy risk by 60% in type 1 diabetes (DCCT/EDIC trial); less clear benefit in type 2 diabetes
- Nutritional deficiencies — B12 supplementation (oral or intramuscular); thiamine replacement; copper supplementation
- Immune-mediated neuropathies — CIDP responds to intravenous immunoglobulin (IVIg), plasmapheresis, or corticosteroids; GBS treated with IVIg or plasmapheresis; MMN responds to IVIg only (corticosteroids can worsen MMN)
- Toxic neuropathies — removal of the offending agent (alcohol cessation, dose reduction or change of chemotherapy, medication discontinuation)
- Vasculitic neuropathy — corticosteroids combined with immunosuppressive agents (cyclophosphamide, azathioprine, rituximab)
- TTR amyloid neuropathy — tafamidis (TTR stabilizer), patisiran or vutrisiran (RNA interference), inotersen (antisense oligonucleotide), liver transplantation
- Fabry disease — enzyme replacement therapy (agalsidase alfa or beta)
Neuropathic Pain Management
First-line agents:
- Gabapentinoids — pregabalin (150-600 mg/day) and gabapentin (900-3600 mg/day); bind alpha-2-delta subunit of voltage-gated calcium channels; NNT approximately 4-7
- Serotonin-norepinephrine reuptake inhibitors (SNRIs) — duloxetine (60-120 mg/day; FDA-approved for diabetic neuropathy) and venlafaxine (150-225 mg/day); NNT approximately 5-7
- Tricyclic antidepressants (TCAs) — amitriptyline, nortriptyline (25-150 mg/day); NNT approximately 3-4; use with caution in elderly due to anticholinergic effects
Second-line and adjunctive agents:
- Topical lidocaine 5% patches — useful for localized neuropathic pain with minimal systemic absorption
- Topical capsaicin 8% patch (Qutenza) — depletes substance P from nociceptors; single 30-60 minute application provides up to 12 weeks of pain relief
- Tramadol — weak opioid with SNRI properties; NNT approximately 4.7
- Strong opioids — oxycodone, morphine; reserved for refractory cases due to dependence risk; NNT approximately 4
- Sodium valproate and carbamazepine — limited evidence for peripheral neuropathy; carbamazepine remains first-line for trigeminal neuralgia
Non-Pharmacological Approaches
- Physical therapy — balance training, gait training, strengthening exercises, fall prevention programs
- Occupational therapy — adaptive strategies for fine motor impairments, assistive devices
- Transcutaneous electrical nerve stimulation (TENS) — may provide modest pain relief with minimal side effects
- Spinal cord stimulation — for refractory painful neuropathy; evidence strongest for diabetic neuropathy
- Acupuncture — limited evidence; some patients report benefit
- Cognitive behavioral therapy (CBT) — helps with pain coping, catastrophizing, and comorbid depression and anxiety
Orthotic and Assistive Devices
- Ankle-foot orthoses (AFOs) — for foot drop to improve gait safety
- Wrist splints — for carpal tunnel syndrome, especially nocturnal use
- Compression stockings — for orthostatic hypotension
- Protective footwear — to prevent ulceration in insensate feet
- Assistive devices — canes, walkers, wheelchairs for balance and mobility impairment
8. Complications
- Falls and fractures — due to sensory ataxia, proprioceptive loss, foot drop, and weakness; fall risk is 15-25 times higher than in age-matched controls
- Foot ulceration and amputation — insensate feet are prone to unrecognized injuries; diabetic foot ulcers affect 15-25% of diabetic patients and precede 85% of lower limb amputations
- Burns and injuries — from inability to detect temperature and pain
- Charcot neuroarthropathy (Charcot foot) — progressive destructive arthropathy of the foot and ankle due to loss of protective sensation and autonomic dysfunction
- Chronic neuropathic pain — persistent, often refractory pain significantly impacting quality of life, sleep, and mental health
- Depression and anxiety — prevalence of depression approximately 30-50% in patients with painful neuropathy
- Autonomic crises — severe orthostatic hypotension, cardiac arrhythmias, gastroparetic crises
- Sleep disturbance — pain and restless legs symptoms frequently disrupt sleep
- Impaired wound healing — autonomic and sensory dysfunction contribute to poor tissue perfusion and delayed healing
- Disability and loss of independence — progressive motor involvement can require assistive devices and lifestyle modifications
9. Prognosis
The prognosis of peripheral neuropathy varies widely depending on the underlying cause, the type and severity of nerve damage, and the timeliness of treatment. Demyelinating neuropathies generally have a better prognosis than axonal neuropathies because the axon remains intact and remyelination can restore function.
Guillain-Barre syndrome has an overall good prognosis, with approximately 80% of patients achieving independent ambulation within 6 months, though 5-10% have significant residual disability and mortality remains approximately 3-7%. CIDP is a chronic condition, but approximately 70-80% of patients respond to immunotherapy and can achieve significant functional improvement.
Diabetic polyneuropathy is typically progressive despite glycemic optimization, though strict control can slow the rate of progression. Toxic and nutritional neuropathies may improve partially or completely after removal of the offending agent and nutritional repletion, though recovery is often incomplete in severe or chronic cases. Hereditary neuropathies (CMT) are slowly progressive over decades and rarely life-threatening but can cause significant disability.
Key prognostic factors include the degree of axonal loss (more axonal damage indicates worse recovery potential), duration of symptoms before treatment, the patient's age (younger patients generally recover better), and the presence of ongoing nerve injury (e.g., continued alcohol use, persistent hyperglycemia). Nerve regeneration occurs at a rate of approximately 1 mm per day (1 inch per month), meaning recovery of distal function after proximal nerve injury can take many months to years.
10. Prevention
- Glycemic control — tight blood glucose management is the most effective strategy for preventing diabetic neuropathy; the Diabetes Control and Complications Trial (DCCT) demonstrated a 60% reduction in neuropathy risk with intensive insulin therapy in type 1 diabetes
- Alcohol moderation — limiting alcohol consumption and ensuring adequate nutritional intake, particularly B vitamins
- Nutritional adequacy — monitoring and supplementing vitamin B12, particularly in vegans, elderly individuals, and patients on metformin or proton pump inhibitors
- Occupational safety — minimizing exposure to heavy metals, solvents, and neurotoxic chemicals; use of protective equipment
- Medication monitoring — dose adjustments and monitoring of neurological function during treatment with neurotoxic medications (e.g., chemotherapy, amiodarone, nitrofurantoin)
- Foot care — daily inspection, proper footwear, regular podiatric care for patients with sensory neuropathy, especially diabetic patients
- Ergonomic practices — proper workstation ergonomics, avoidance of repetitive strain to prevent entrapment neuropathies
- Genetic counseling — for families with hereditary neuropathies, allowing early identification and monitoring
- Fall prevention — home safety modifications, balance exercises, appropriate assistive devices
Interactive Visualization Nerve Impulse — fire an action potential Watch it race down the axon: sodium rushing in, potassium out, a live voltage trace spiking, and neurotransmitter crossing the synapse. Launch → Interactive Visualization Vitamin B12’s Impossible Journey Five stages, two carrier proteins, a working stomach and one specific stretch of gut. Break any link — a PPI, metformin, pernicious anaemia — and absorption collapses. Launch → Interactive Visualization Pain & the Gate Control — close the gate yourself Fire a pain signal up the spinal cord — then rub the skin and watch the gate close, or release endorphins and see the same signal fade before it ever reaches the brain. Launch → Interactive Visualization The Reflex Arc — fire a reflex faster than thought Tap the tendon and watch the signal fire into the spinal cord and straight back out to the muscle in ~50 ms — while the brain only finds out afterward. Launch → Interactive Visualization Why Chili Burns — hijack your heat receptor Discover that chili isn't hot — it hijacks your heat receptor to fake a burn — then reach for water and fail, milk and succeed, and see how the same trick turns nerve pain down in a capsaicin cream. Launch →
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Research Papers
- Connections
- Featured Videos
Research Papers
Curated PubMed topic searches on Peripheral Neuropathy. Each link opens a live PubMed query so the result set stays current as new studies are indexed.
- PubMed topic search: Peripheral neuropathy review
- PubMed topic search: Diabetic peripheral neuropathy
- PubMed topic search: Chemotherapy-induced peripheral neuropathy
- PubMed topic search: Small fiber neuropathy
- PubMed topic search: Vitamin B12 deficiency neuropathy
- PubMed topic search: Alpha lipoic acid neuropathy
- PubMed topic search: Duloxetine neuropathic pain
- PubMed topic search: Gabapentin pregabalin neuropathy
- PubMed topic search: Guillain-Barre syndrome review
- PubMed topic search: CIDP chronic inflammatory demyelinating
- PubMed topic search: Nerve conduction study peripheral neuropathy
- PubMed topic search: Skin biopsy small fiber neuropathy
Connections
- Why Chili Burns: Capsaicin & the TRPV1 Heat Sensor — interactive animation
- The Reflex Arc: Faster Than Thought — interactive animation
- Pain, the Gate Control & Why Rubbing Helps — interactive animation
- Vitamin B12’s Impossible Journey — interactive animation
- Nerve Impulse — interactive animation
- Alpha Lipoic Acid
- Antioxidants
- Vitamin B12
- Numbness & Tingling
- Vitamin B6
- Vitamin D3
- ALS
- Multiple Sclerosis
- Myasthenia Gravis
- Chronic Pain
- Nociceptive vs Neuropathic vs Nociplastic Pain
- Non-Opioid Medications for Chronic Pain
- Diabetes
- Lion's Mane Mushroom
- Magnesium
- Joint Pain
- Alpha-Gal Syndrome
- Depression
- Vitamin E
- Parkinsons Disease
- Addiction
- Herpes Simplex
- Diabetic Retinopathy
- Salt in Socks — why abrasive granules in a sock are a serious hazard on a foot that cannot feel injury