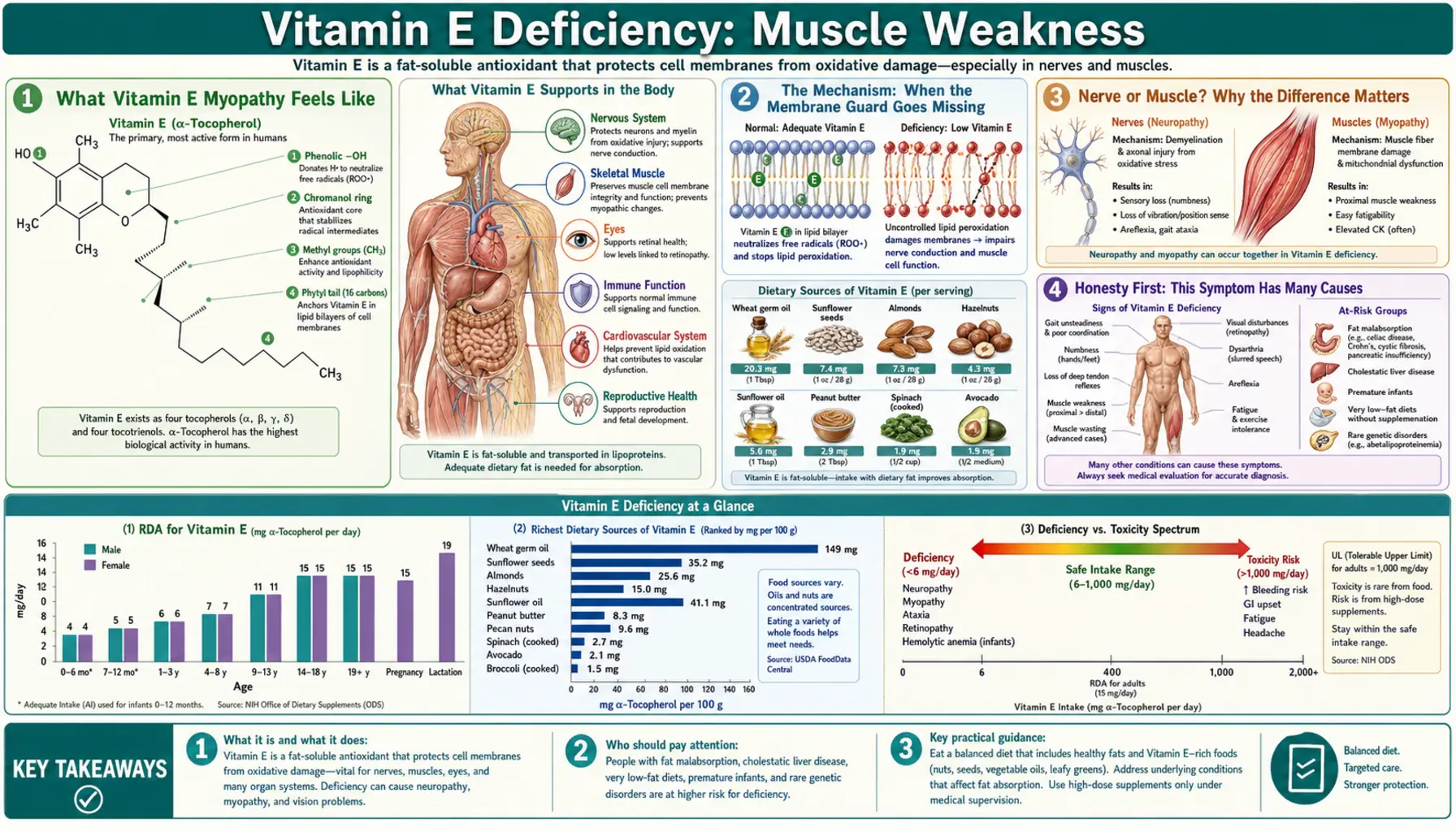
Vitamin E Deficiency: Muscle Weakness
When long-standing vitamin E deficiency reaches the muscles, the result is a slow, painless loss of strength — a true myopathy. People notice that climbing stairs, standing up from a low chair, or lifting things overhead has quietly become harder, with the big muscles of the thighs, hips, and shoulders giving way first. It is important to be honest from the start: muscle weakness from vitamin E deficiency is uncommon, and far more often the muscle complaints of someone who is low in vitamin E come from the accompanying nerve damage (see Nerve Damage & Ataxia) rather than from the muscle itself. This page explains how a lack of this fat-soluble antioxidant can damage muscle fibers directly, why the weakness has the pattern it does, the many other causes that are far more likely, and how the muscle recovers once vitamin E is replaced.
Table of Contents
- What Vitamin E Myopathy Feels Like
- The Mechanism: When the Membrane Guard Goes Missing
- Nerve or Muscle? Why the Difference Matters
- Honesty First: This Symptom Has Many Causes
- Clues That Point Toward Vitamin E
- What Actually Causes Vitamin E Deficiency
- Getting Tested
- Correcting the Deficiency and Recovering Strength
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Vitamin E Myopathy Feels Like
The muscle weakness that can accompany severe, prolonged vitamin E deficiency tends to be proximal — it strikes the large muscles closest to the trunk first. The thighs, hips, and shoulders weaken before the hands and feet, and that produces a recognizable set of everyday complaints:
- Trouble climbing stairs — the thigh and hip muscles that lift the body up each step are the ones that fade first. People describe pulling themselves up by the handrail.
- Difficulty rising from a chair — standing up from a seat is a pure test of hip and thigh strength, so needing to push off with the arms or rock forward for momentum is an early sign.
- Hard to reach overhead — hanging laundry, washing the hair, or putting something on a high shelf becomes tiring because the shoulder girdle is weak.
- Heavy, unreliable legs — the legs can feel leaden and may give way, especially on uneven ground or descending stairs.
Two features are worth holding onto. First, vitamin E myopathy is usually painless in its early stages — there is no soreness or tenderness; the muscle simply does not produce its normal force. Second, it comes on slowly, over months to years, because vitamin E is stored in body fat and the body draws down those stores gradually. Sudden weakness over hours or days is essentially never vitamin E deficiency and points to something else entirely.
Because the onset is so gradual and painless, people very commonly attribute it to ordinary aging, being “out of shape,” or simply slowing down — which is one reason a genuine deficiency myopathy can go unrecognized for a long time. The other reason, covered below, is that the weakness a vitamin E–deficient person reports is often coming from their nerves rather than their muscle.
The Mechanism: When the Membrane Guard Goes Missing
Vitamin E is the body's most important fat-soluble antioxidant. Its single best-understood job is to sit inside the fatty membranes that wrap every cell and protect them from a chain reaction called lipid peroxidation. Cell membranes are built from polyunsaturated fats, and those fats are chemically fragile: a single reactive molecule (a free radical) can rip an electron from one, turning it into a radical that attacks its neighbor, which attacks the next — a self-propagating chain that, unchecked, shreds the membrane. Vitamin E (chiefly α-tocopherol) is the molecule that steps in, donates an electron to quench the radical, and stops the chain — which is why one review summarized decades of work with the deliberately modest title “vitamin E, antioxidant and nothing more.”
Muscle is unusually exposed to this kind of damage. Working muscle burns enormous amounts of oxygen and is dense with mitochondria, the cellular power plants that are themselves a major source of free radicals. A muscle fiber is also an exquisitely engineered electrical and mechanical machine: it depends on intact membranes both at its surface and in an internal network (the sarcoplasmic reticulum) that releases and recaptures the calcium that drives each contraction. When vitamin E is chronically absent, the protective antioxidant shield thins out, oxidative damage to these membranes accumulates, and the fiber's machinery is gradually injured. Over time, fibers degenerate, leak their contents, and in severe cases die — the picture pathologists have long described in vitamin E–deficient muscle, including the accumulation of a brown oxidized-fat pigment called ceroid, the chemical footprint of runaway lipid peroxidation.
An analogy. Think of each muscle fiber's membranes as the rust-proof coating on a machine that runs hot and wet all day. Vitamin E is that coating. With it in place, the metal underneath is protected and the machine keeps working. Strip the coating away and nothing fails overnight — but rust creeps in at the edges, then spreads, and month by month moving parts seize and weaken. Restore the coating and you stop the rust from advancing; the parts that are not yet destroyed can be cleaned up and returned to service. That is why this weakness builds over months, not minutes, and why catching it early matters so much.
It is worth being candid about the limits of certainty here. The membrane-antioxidant mechanism is well established, and animals deprived of vitamin E reliably develop a nutritional muscle disease (so reliably that veterinary medicine has recognized it for the better part of a century). In humans, the muscle component of vitamin E deficiency is real but much less common and harder to disentangle from the nerve damage that usually travels with it — which is the subject of the next section.
Nerve or Muscle? Why the Difference Matters
This is the single most important point on the page. When someone with vitamin E deficiency reports “weakness,” the cause is more often the nervous system than the muscle itself. The hallmark of human vitamin E deficiency is a neurological syndrome — a spinocerebellar disorder with loss of coordination (ataxia), loss of position sense, absent reflexes, and progressive difficulty with steady, controlled movement. That picture comes from damage to the long sensory nerve fibers and the spinal cord pathways that carry balance and position information, not primarily from sick muscle.
The distinction is not academic, because the two produce different problems that feel similar to the person experiencing them:
- True myopathic weakness — the muscle cannot generate force even when the signal to contract arrives intact. This is what this page is about, and it is the less common contributor in human vitamin E deficiency.
- Neuropathic “weakness” — the muscle is fundamentally able to contract, but the nerve signals reaching it are degraded, and the loss of position sense makes movement clumsy, unsteady, and effortful. People describe this as weakness, wobbliness, or legs that “won't do what they're told,” even though formal strength testing may be relatively preserved.
Because the neurological syndrome dominates the human picture, the deep detail on coordination loss, areflexia, and the spinal-cord pathways lives on the sibling page Nerve Damage & Ataxia. If your main experience is unsteadiness, falling, or a clumsy, “drunken” gait rather than a clear-cut inability to push, lift, or rise, that page is the better starting point. In practice the two often coexist, and the doctor's job is to sort out how much of a given person's difficulty is muscle and how much is nerve — which determines what the tests show and what to expect from treatment.
Honesty First: This Symptom Has Many Causes
Muscle weakness is one of the most common and least specific complaints in all of medicine, and the overwhelming majority of cases have nothing to do with vitamin E. Before pinning weakness on a vitamin E deficiency — which is genuinely rare in the general population — it is essential to recognize how many ordinary explanations come first:
- Deconditioning and aging. The gradual, age-related loss of muscle mass (sarcopenia) and the deconditioning that follows illness, inactivity, or bed rest are by far the most common causes of slowly progressive proximal weakness.
- Other nutrient problems. Low potassium is a classic cause of proximal weakness; vitamin D deficiency causes a well-recognized myopathy; low magnesium, low phosphate, and inadequate protein all impair muscle.
- Thyroid disease. Both an overactive and an underactive thyroid produce a proximal myopathy that closely mimics other causes.
- Medications. Statins, corticosteroids, and some other drugs can directly cause muscle weakness or breakdown — one of the first things a clinician reviews.
- Primary neuromuscular disease. The inflammatory myopathies (polymyositis, dermatomyositis), muscular dystrophies, myasthenia gravis, and motor neuron disease all present with weakness and are far more common explanations than a vitamin E deficiency.
- Systemic illness. Anemia, chronic kidney or liver disease, heart failure, infection, and cancer can all leave muscles weak.
The honest bottom line: weakness is not proof of vitamin E deficiency, and vitamin E is rarely the answer. It earns serious consideration only in the specific contexts described next — chiefly people who cannot absorb fat normally. For everyone else, weakness should be worked up on its own merits, and self-treating with vitamin E supplements in the hope of fixing weakness is not supported by evidence.
Clues That Point Toward Vitamin E
So when does vitamin E deserve a place on the list? A handful of features should raise the question:
- A reason fat absorption is impaired. Vitamin E is fat-soluble, so it is absorbed only along with dietary fat. Any condition that blocks fat absorption — see the next section — is the single biggest clue, because that is essentially the only way a person eating a normal diet becomes deficient.
- Neurological signs alongside the weakness. Unsteadiness, a wide-based or clumsy gait, loss of position and vibration sense, and absent ankle reflexes point toward the vitamin E neurological syndrome described on Nerve Damage & Ataxia. Pure muscle weakness with no neurological signs is much less suggestive.
- Other deficiency clues traveling together. Because fat malabsorption depletes all the fat-soluble vitamins (A, D, E, and K), accompanying findings — easy bleeding from low vitamin K, bone or muscle aches from low vitamin D, or night-vision trouble from low vitamin A — make a fat-malabsorption picture, and therefore vitamin E deficiency, more plausible. Severe deficiency can also damage red cell membranes, producing a mild hemolytic anemia, and affect the retina, producing vision problems.
- A long timeline. Symptoms that have crept on over many months to years in someone with chronic digestive disease fit; an abrupt change does not.
None of these is proof on its own, but together — especially fat malabsorption plus neurological signs — they are what move a clinician to actually measure a serum vitamin E level rather than assume it is normal.
What Actually Causes Vitamin E Deficiency
In well-nourished adults, dietary vitamin E deficiency essentially does not occur — the vitamin is widespread in vegetable oils, nuts, seeds, and leafy greens, and the body holds reserves in fat. When deficiency does happen, it almost always comes from one of three routes:
- Fat malabsorption — the main cause. Because vitamin E rides into the body with dietary fat, any disease that prevents fat absorption can starve the tissues of it over time. The classic examples are cystic fibrosis (where the pancreas fails to deliver the enzymes that digest fat), celiac disease, Crohn's disease, chronic liver and biliary disease (especially cholestatic disease in infants, where bile needed for fat absorption is lacking), chronic pancreatitis, and the after-effects of major small-bowel surgery (short bowel syndrome).
- Inherited transport defects. Two rare genetic conditions cause profound deficiency. In ataxia with vitamin E deficiency (AVED), mutations cripple the α-tocopherol transfer protein (α-TTP) that the liver uses to load vitamin E onto the lipoproteins that carry it through the blood — so even with normal absorption, the body cannot keep vitamin E in circulation. In abetalipoproteinemia (Bassen–Kornzweig syndrome), the body cannot build the lipoprotein particles that transport fat and fat-soluble vitamins at all. Both produce severe, early neurological disease unless treated with large doses of vitamin E for life.
- Severe, prolonged malnutrition. Only in the setting of extreme, long-standing dietary deprivation — not a typical Western diet — does intake itself become the limiting factor, and even then it usually compounds an absorption problem. Premature infants are a special case: they are born with very low vitamin E stores and immature absorption, which is why their levels are watched in neonatal care.
The practical message is that identifying why vitamin E is low matters more than the low number itself, because the underlying disease — cystic fibrosis, celiac disease, a genetic transport defect — is what truly needs managing, and the vitamin E is replaced as part of treating it.
Getting Tested
Confirming or excluding vitamin E deficiency starts with a simple blood test: a serum α-tocopherol level. Because vitamin E travels in the blood attached to fats, the result is most meaningful when interpreted alongside blood lipids — in people with very high or very low cholesterol, doctors look at the ratio of vitamin E to total lipids rather than the raw number, so that a normal amount of vitamin E carried on a low amount of fat is not mistaken for deficiency.
Because true deficiency almost always reflects an absorption or transport problem, the testing rarely stops there. A clinician evaluating weakness with possible vitamin E deficiency will typically also:
- Look for fat malabsorption and the disease causing it — reviewing digestive symptoms and, where relevant, checking liver function tests and screening for celiac disease, pancreatic insufficiency, or cystic fibrosis.
- Check the other fat-soluble vitamins (A, D, K), since they tend to fall together and a pattern of multiple low levels strongly supports malabsorption.
- Run a broad comprehensive metabolic panel and other studies to find or rule out the far more common causes of weakness — electrolytes (including potassium), kidney and liver function, glucose, and thyroid tests.
- Measure creatine kinase (CK), an enzyme that leaks from damaged muscle. Modest elevations can occur when muscle fibers are being injured, and a CK level helps gauge whether muscle is actively breaking down.
- When the picture is unclear, refer for nerve conduction studies, electromyography (EMG), or imaging to separate a nerve problem from a muscle problem — the distinction that the nerve-or-muscle section above turns on.
The overall point: a single inexpensive vitamin E level can confirm or exclude the deficiency, but because weakness has so many other causes, it is almost always measured as part of a wider work-up rather than on its own.
Correcting the Deficiency and Recovering Strength
The encouraging news is that vitamin E deficiency myopathy responds to treatment, and muscle that has not been permanently destroyed can recover its strength once the vitamin is restored. How replacement is done depends entirely on the cause:
- Treat the underlying disease first. Because deficiency almost always stems from malabsorption, managing the root cause — pancreatic enzyme replacement in cystic fibrosis, a gluten-free diet in celiac disease, controlling Crohn's disease — is what allows vitamin E (and the other fat-soluble vitamins) to be absorbed and held in the body again.
- Supplement at a dose that matches the problem. Correcting an established deficiency, especially one from malabsorption or a transport defect, requires medical doses prescribed and monitored by a clinician — often much higher than ordinary nutritional amounts, and in malabsorption sometimes given in special water-miscible forms so they can be absorbed without normal fat handling. Inherited disorders such as AVED and abetalipoproteinemia require high-dose vitamin E for life, and starting it early can prevent or limit the neurological damage.
- Food for ordinary maintenance. For preventing deficiency and meeting everyday needs, vitamin E–rich whole foods are the foundation: almonds and other nuts and seeds, vegetable oils, avocado, and leafy greens such as spinach and broccoli. The adult recommended intake is 15 mg (about 22 IU of natural-source) per day. (See the vitamin E food sources page for more.)
Recovery follows the biology. Nerve and muscle damage that has built up over years improves slowly — over months — and the most important determinant of outcome is how early treatment begins, since severe, long-untreated damage can be permanent. This is also why a dose that fully corrects the level is verified with follow-up blood tests rather than assumed.
A word of caution that runs the other way: more is not better. Routinely taking large doses of vitamin E in the absence of a documented deficiency is not a way to build strength, and high-dose supplements carry their own risks — chiefly an increased tendency to bleed, because vitamin E interferes with vitamin K–dependent clotting. High-dose vitamin E is a treatment for a specific, diagnosed problem, not a general tonic for tired muscles.
When to Seek Care / Red Flags
Vitamin E myopathy itself comes on slowly and is rarely an emergency. But weakness has dangerous mimics, and certain features mean you should be evaluated promptly rather than waiting:
- Weakness that comes on over hours or a few days. This is the opposite of the vitamin E pattern and can signal a stroke, an acute nerve syndrome (such as Guillain–Barré), a severe electrolyte disturbance, or another urgent problem. Sudden weakness, facial droop, or difficulty speaking warrants emergency care.
- Weakness spreading toward the chest, with breathing or swallowing trouble. Shortness of breath, an inability to take a full breath, or difficulty swallowing alongside spreading weakness is an emergency, regardless of the suspected cause.
- Dark (tea- or cola-colored) urine with muscle pain and weakness. This can indicate muscle breakdown (rhabdomyolysis), which threatens the kidneys and needs urgent treatment.
- Easy bruising or abnormal bleeding together with the weakness — a possible sign of the vitamin K deficiency that travels with fat malabsorption, which should be checked.
- Falls and loss of balance. If unsteadiness and falling are prominent, the issue may be the vitamin E nerve syndrome rather than muscle, and fall prevention becomes an immediate safety priority.
Short of those alarms, the right step for slowly progressive, painless weakness is a non-urgent but real medical evaluation — not a bottle of supplements. A clinician can sort out whether vitamin E is even part of the story and, far more often, find the more common cause that is.
Key Research Papers
- Traber MG, Atkinson J (2007). Vitamin E, antioxidant and nothing more. Free Radical Biology and Medicine;43(1):4-15. — DOI: 10.1016/j.freeradbiomed.2007.03.024
- Traber MG, Arai H (1999). Molecular mechanisms of vitamin E transport. Annual Review of Nutrition;19:343-355. — DOI: 10.1146/annurev.nutr.19.1.343
- Muller DPR (2010). Vitamin E and neurological function. Molecular Nutrition & Food Research;54(5):710-718. — DOI: 10.1002/mnfr.200900460
- Traber MG, Sokol RJ, Ringel SP, et al. (1987). Lack of tocopherol in peripheral nerves of vitamin E-deficient patients with peripheral neuropathy. New England Journal of Medicine;317(5):262-265. — DOI: 10.1056/NEJM198707303170502
- Harding AE, Matthews S, Jones S, et al. (1985). Spinocerebellar degeneration associated with a selective defect of vitamin E absorption. New England Journal of Medicine;313(1):32-35. — DOI: 10.1056/NEJM198507043130107
- Yokota T, Wada Y, Furukawa T, et al. (1987). Adult-onset spinocerebellar syndrome with idiopathic vitamin E deficiency. Annals of Neurology;22(1):84-87. — DOI: 10.1002/ana.410220119
- Ouahchi K, Arita M, Kayden H, et al. (1995). Ataxia with isolated vitamin E deficiency is caused by mutations in the α-tocopherol transfer protein. Nature Genetics;9(2):141-145. — DOI: 10.1038/ng0295-141
- Stamp GWH, Evans DJ (1987). Accumulation of ceroid in smooth muscle indicates severe malabsorption and vitamin E deficiency. Journal of Clinical Pathology;40(7):798-802. — DOI: 10.1136/jcp.40.7.798
- Meacci E, Vasta V, Garcia-Gil M, et al. (2024). Potential Vitamin E Signaling Mediators in Skeletal Muscle. Antioxidants;13(11):1383. — DOI: 10.3390/antiox13111383
- Goss-Sampson MA, Muller DPR (1989). Clinical importance of vitamin E: a review. Journal of Human Nutrition and Dietetics;2(3):145-150. — DOI: 10.1111/j.1365-277X.1989.tb00018.x
- Neville HE, Ringel SP, Guggenheim MA, et al. (1983). Ultrastructural and histochemical abnormalities of skeletal muscle in patients with chronic vitamin E deficiency. Neurology;33(4):483-488. — PubMed
- National Institutes of Health, Office of Dietary Supplements (2021). Vitamin E — Health Professional Fact Sheet. — PubMed (vitamin E deficiency reviews)
PubMed Topic Searches
- PubMed — Vitamin E deficiency and skeletal muscle myopathy
- PubMed — Vitamin E deficiency in fat malabsorption and cystic fibrosis
- PubMed — Ataxia with vitamin E deficiency and α-TTP
- PubMed — Abetalipoproteinemia and neuromuscular disease
- PubMed — Lipid peroxidation, muscle membranes, and vitamin E
Connections
- Vitamin E Deficiency Hub
- Vitamin E Deficiency: Nerve Damage & Ataxia
- Vitamin E Deficiency: Hemolytic Anemia
- Vitamin E Deficiency: Vision Problems
- Vitamin E Toxicity Hub
- Vitamin E Overview
- Vitamin E Benefits
- Vitamin E Food Sources
- Hypokalemia and Muscle Weakness
- Vitamin D
- Selenium
- Cystic Fibrosis
- Celiac Disease
- Crohn's Disease
- Peripheral Neuropathy
- Comprehensive Metabolic Panel
- Liver Function Tests
- Almonds
- Spinach
- Avocado