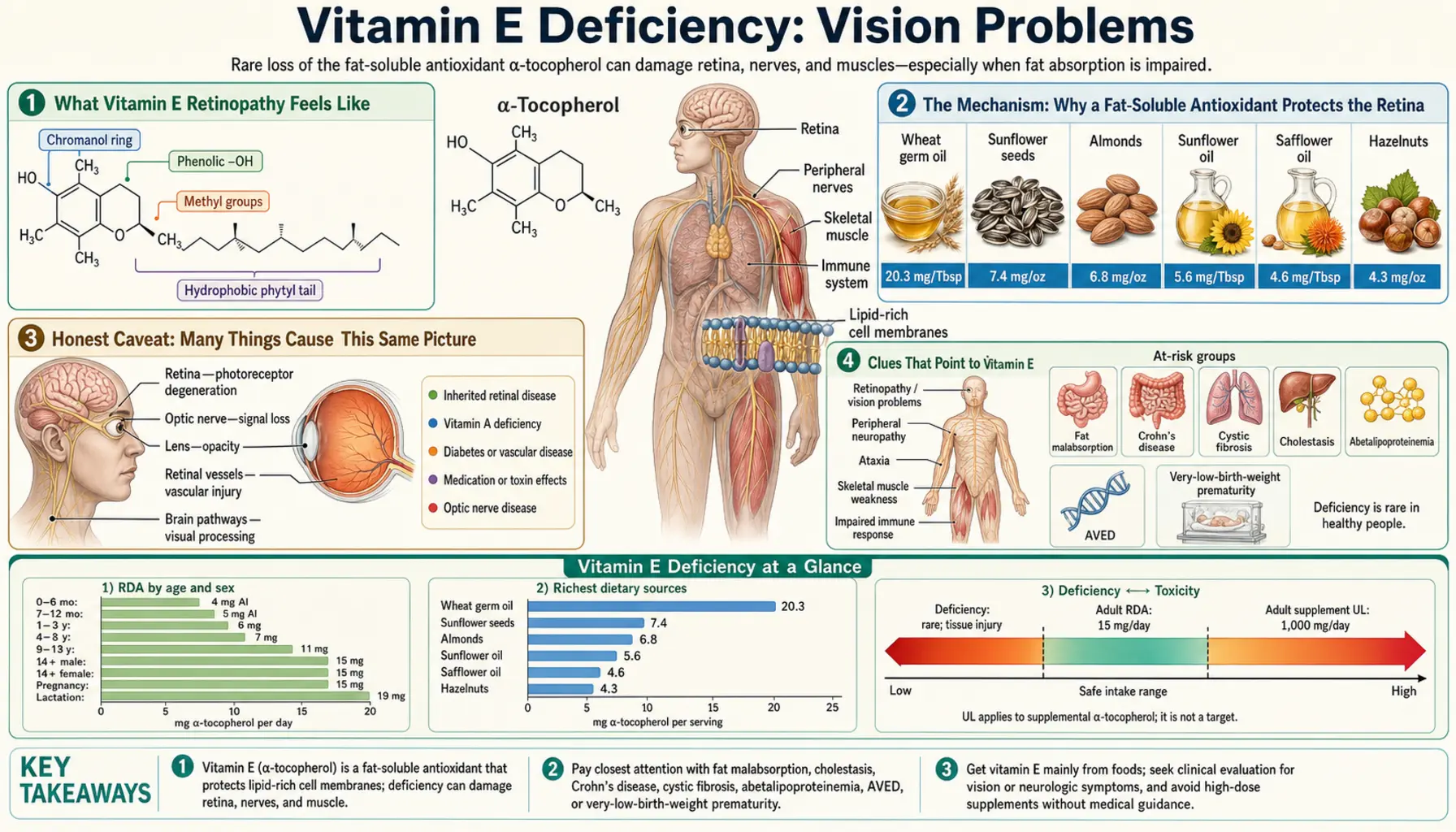
Vitamin E Deficiency: Vision Problems
When vitamin E runs low for years, one of the organs that quietly pays the price is the retina — the light-sensing tissue at the back of the eye. The damage is slow and often silent at first: trouble seeing in dim light, a gradual narrowing of side vision, and a creeping loss of sharpness that can eventually be mistaken for “just getting older.” On an eye exam it can look like a pigment-scattered, degenerating retina — a picture doctors call a pigmentary retinopathy, sometimes indistinguishable from retinitis pigmentosa. The crucial point, and the reason this page exists, is that this particular cause of failing vision is one of the very few that can be halted, and sometimes partly reversed, simply by restoring vitamin E early enough. This page explains why the retina is so dependent on vitamin E, how the vision loss unfolds, the much more common conditions it can be confused with, and how it is diagnosed and treated.
Table of Contents
- What Vitamin E Retinopathy Feels Like
- The Mechanism: Why a Fat-Soluble Antioxidant Protects the Retina
- Honest Caveat: Many Things Cause This Same Picture
- Clues That Point to Vitamin E
- What Drives Vitamin E Low Enough to Harm the Eye
- Getting Tested
- Correcting the Deficiency and Protecting Vision
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Vitamin E Retinopathy Feels Like
Retinopathy from vitamin E deficiency does not announce itself. It does not cause pain, redness, or a sudden change you would rush to the emergency room for. Instead it behaves like a slow dimming of a room over months and years — so gradual that people adapt without realizing how much they have lost. The symptoms follow the part of the retina that suffers first, and they tend to appear in a recognizable order:
- Night blindness (nyctalopia) — usually the earliest complaint. The rod photoreceptors, which handle dim-light and peripheral vision, are especially vulnerable. People notice they can no longer find their seat in a dark cinema, that driving at night has become frightening, or that it takes far too long for their eyes to adjust when they walk into a dim room.
- Shrinking side vision (peripheral field loss) — because the damage often spreads inward from the mid-periphery, the field of view narrows over time. People bump into door frames, miss a hand held out beside them, or stop noticing cars and cyclists approaching from the side. In advanced cases this becomes a true tunnel vision.
- Slower light/dark adaptation — stepping from bright sunlight into a shop, or from a lit room into a dark hallway, leaves them effectively blind for an uncomfortably long time.
- Gradual loss of sharpness — central detail and reading vision usually hold up until later, but over years the overall crispness of the world fades.
- Trouble with contrast and color — faded, washed-out colors and difficulty telling similar shades apart can appear as the retina degenerates.
On an eye exam, the back of the eye can show the hallmarks of a pigmentary retinopathy: scattered clumps of pigment in the retina (sometimes in the “bone-spicule” pattern of retinitis pigmentosa), a pale optic disc, and narrowed retinal blood vessels. An electroretinogram (ERG) — a test that measures the retina's electrical response to flashes of light — typically shows a reduced or delayed signal, with the rods affected before the cones. Crucially, in the early stages all of this can be present while the person still reads the eye chart reasonably well, which is exactly why it is so easy to overlook.
The Mechanism: Why a Fat-Soluble Antioxidant Protects the Retina
To understand why a vitamin shortage attacks the eye, start with what vitamin E actually is and what it does. Vitamin E (the most active human form is alpha-tocopherol) is the body's principal fat-soluble antioxidant. Its single most important job is to sit inside cell membranes and protect their fatty building blocks — the polyunsaturated fatty acids (PUFAs) — from a destructive chain reaction called lipid peroxidation. When an oxygen free radical attacks a PUFA, it rips off an electron and turns that fat into a radical itself, which then attacks the next fat, and the next, like a fuse burning along a row of membrane. Vitamin E stops the fuse: it donates an electron to the radical, neutralizing it, and converts a dangerous propagating chain into a harmless dead end (Traber & Atkinson, 2007).
Now consider why the retina is uniquely exposed to exactly this kind of damage — it is, in a sense, the perfect storm for lipid peroxidation:
- It is drenched in light. Light is energy, and absorbing it generates reactive oxygen species as a byproduct of vision itself.
- It burns enormous amounts of oxygen. The retina has one of the highest metabolic and oxygen-consumption rates of any tissue in the body, and oxygen is the raw material for free radicals.
- Its membranes are extraordinarily rich in PUFAs. Photoreceptor outer segments are packed with stacks of membranes loaded with docosahexaenoic acid (DHA), one of the most peroxidation-prone fats there is — precisely the fuel that vitamin E exists to protect.
So the retina combines the three things that drive lipid peroxidation — light, oxygen, and vulnerable fat — in one small patch of tissue. Vitamin E is the fire blanket that keeps those membranes from oxidizing. Take the blanket away for long enough and the photoreceptor membranes slowly oxidize, the cells are injured, pigment is released and migrates (producing the speckled look on exam), and the rods — the most numerous and most lipid-dense photoreceptors — begin to die first. That is why night and peripheral vision go before central sharpness.
An analogy. Think of each photoreceptor membrane as a stretch of dry, oil-soaked rope strung through a room full of sparks (the light and oxygen of vision). Vitamin E molecules are flame retardant woven into the rope: when a spark lands and starts to char a fiber, the retardant smothers it before the burn can travel. With plenty of vitamin E, sparks land and fizzle harmlessly all day long. Remove the retardant and each spark now starts a small creeping burn — no single one is dramatic, but over months and years the rope frays and finally parts. Restore the retardant in time and you stop new burns from spreading; what has already charred, though, may not grow back — which is why early treatment matters so much.
There is also a delivery problem unique to vitamin E. Because it is fat-soluble, vitamin E rides through the body inside fat-carrying lipoproteins, and a specialized liver protein called alpha-tocopherol transfer protein (α-TTP) loads alpha-tocopherol back into the bloodstream so it can reach tissues like the retina. When fat absorption fails, or when α-TTP is genetically broken, vitamin E never makes it to the eye in the first place — and these are exactly the situations in which retinopathy appears (Brigelius-Flohé & Traber, 1999).
Honest Caveat: Many Things Cause This Same Picture
It is important to be straight about this: vitamin E deficiency is an uncommon cause of vision loss, and night blindness or a degenerating retina is almost never due to low vitamin E in an otherwise healthy, well-fed person. The symptoms described above — night blindness, shrinking side vision, a pigmentary retinopathy — are shared by a long list of conditions, most of them far more common. Before anyone concludes that vitamin E is the culprit, these have to be on the table:
- Retinitis pigmentosa (genetic) — a group of inherited retinal degenerations is the classic cause of night blindness plus tunnel vision plus a bone-spicule, pigmentary retina. Vitamin E deficiency can mimic it almost exactly, which is the whole point of testing rather than assuming.
- Vitamin A deficiency — vitamin A is the other fat-soluble vitamin essential for vision, and it is the more famous cause of night blindness because it is the raw material for the light-detecting pigment rhodopsin. Low vitamin A and low vitamin E often travel together (both depend on fat absorption), so the two are easy to confuse and frequently coexist. See Vitamin A and Vision.
- Diabetic eye disease — diabetic retinopathy is one of the leading causes of vision loss in adults and has nothing to do with vitamin E.
- Age-related macular degeneration — macular degeneration attacks central vision in older adults and is far more common than any vitamin-deficiency retinopathy.
- Cataract and glaucoma — clouding of the lens and optic-nerve damage are extremely common and cause their own patterns of blur and field loss.
- Medication-related retinopathy — certain long-term drugs (for example hydroxychloroquine) can damage the retina.
The honest bottom line: a single symptom like trouble seeing at night is not proof of vitamin E deficiency. What raises vitamin E up the list is not the eye finding alone but the company it keeps — a person who also has a fat-absorption problem, neurological signs, or a known genetic condition. That context is what the next section is about.
Clues That Point to Vitamin E
Because the retinal picture is non-specific, the clue to vitamin E is usually that the eye is not the only thing affected. Vitamin E deficiency severe enough to harm the retina almost always reflects either a long-standing fat-malabsorption problem or a rare genetic defect, and those conditions leave other fingerprints. The combination that should make a clinician think of vitamin E is a pigmentary retinopathy together with one or more of the following:
- Neurological signs — the same antioxidant failure that injures the retina also injures long nerve fibers. Unsteady walking (ataxia), loss of position and vibration sense, absent reflexes, and clumsy hands often accompany the eye changes. In fact, “ataxia with retinitis pigmentosa” is a recognized presentation of vitamin E deficiency (Yokota et al., 1996). See the sibling page Vitamin E Deficiency: Nerve Damage & Ataxia.
- A known fat-malabsorption condition — cystic fibrosis, cholestatic (bile-blocked) liver disease, severe celiac or Crohn's disease, chronic pancreatitis, short-bowel syndrome after surgery, or the rare inherited fat-handling disorder abetalipoproteinemia. In all of these, dietary fat — and the fat-soluble vitamins riding with it — is poorly absorbed.
- Other fat-soluble vitamin deficiencies — low vitamin A (night blindness, dry eyes), low vitamin D (bone problems), or easy bruising/bleeding from low vitamin K commonly appear alongside low vitamin E, because they all share the same absorption pathway.
- A childhood onset or a family history — when retinopathy plus ataxia appears in a child, a teenager, or several relatives, an inherited cause such as abetalipoproteinemia or ataxia with isolated vitamin E deficiency (AVED) — caused by mutations in the α-TTP gene — rises to the top of the list (Hoshino et al., 1999).
Put simply: an isolated retinopathy in a healthy adult is very unlikely to be vitamin E; a retinopathy in someone who also has wobbly balance, a malabsorption diagnosis, or a suggestive family history is the pattern worth chasing — because it is treatable.
What Drives Vitamin E Low Enough to Harm the Eye
Dietary vitamin E deficiency from simply eating poorly is rare in healthy people — vitamin E is widespread in nuts, seeds, vegetable oils, and leafy greens, and the body holds reserves in fat tissue. When deficiency becomes severe enough to damage the retina, there is almost always a reason the vitamin cannot be absorbed or transported. The main culprits:
- Fat malabsorption (the usual route). Vitamin E is fat-soluble, so anything that blocks fat digestion or absorption blocks vitamin E. This includes cystic fibrosis (pancreatic enzyme failure), chronic cholestatic liver disease in which bile cannot reach the gut to emulsify fat (Sokol et al., 1983; Alvarez et al., 1985), celiac disease, Crohn's disease, chronic pancreatitis, and surgical short-bowel syndrome.
- Abetalipoproteinemia. This rare inherited disorder prevents the body from making the lipoproteins that carry fat (and vitamin E) through the blood. Affected children malabsorb fat and develop a slowly progressive retinopathy plus neurological degeneration — and the landmark finding is that high-dose vitamin E can prevent the retinopathy if started early (Runge et al., 1986).
- Ataxia with isolated vitamin E deficiency (AVED). Here the gut absorbs vitamin E normally, but mutations in the α-tocopherol transfer protein gene mean the liver cannot reload alpha-tocopherol into the bloodstream, so it is rapidly lost and tissues are starved. The result is a Friedreich-like ataxia, sometimes with retinitis pigmentosa, that responds to lifelong vitamin E (Schuelke et al., 1999; Yokota, 2000).
- Severe, prolonged malnutrition — in extreme cases of starvation or in premature, very-low-birth-weight infants (who are born with negligible vitamin E stores), deficiency can occur, though the eye consequences in adults specifically arise from the malabsorption and genetic causes above.
The thread running through all of these is the same: it is not that the person ate too little vitamin E, but that it could not get from the plate to the retina.
Getting Tested
Sorting out whether vitamin E is behind a retinopathy is done with a combination of an eye assessment and a few targeted blood tests — and the reason it is worth doing is that, unlike most causes of a degenerating retina, this one is treatable.
- Serum vitamin E (alpha-tocopherol) level — a simple blood test that measures circulating vitamin E. Because vitamin E travels in blood fats, the result is most meaningful when interpreted alongside blood lipids; clinicians often use the ratio of vitamin E to total lipids (or cholesterol) rather than the raw number, especially when fat levels are abnormal (as they are in abetalipoproteinemia, where they are very low).
- The eye exam — a dilated retinal examination looks for the pigmentary changes, vessel narrowing, and optic-disc pallor described above. An electroretinogram (ERG) objectively measures photoreceptor function and can detect rod dysfunction before the person notices much, and visual-field testing maps the extent of peripheral loss.
- Tests for the underlying cause — since deficiency points to malabsorption or a genetic defect, the workup usually includes the other fat-soluble vitamins (A, D, and a clotting test for K), liver and pancreatic studies, celiac antibodies, and — in the right setting — a blood film and lipid panel (the absent lipoproteins and spiky red cells of abetalipoproteinemia) or genetic testing for the α-TTP gene.
A low vitamin E level in someone with a compatible retinopathy and a malabsorption or genetic context essentially makes the diagnosis — and, importantly, it identifies a cause of vision loss that can be acted on rather than only watched.
Correcting the Deficiency and Protecting Vision
The central, hopeful message of this whole topic is that vitamin E retinopathy is one of the few retinal degenerations that can be stopped — and the earlier it is caught, the more vision is preserved. Treatment is straightforward in principle: get vitamin E back into the tissues and keep it there. How that is done depends on the cause.
- Food first, for ordinary low-normal levels. When vitamin E is only modestly low and absorption is intact, the foundation is vitamin-E-rich whole foods: almonds and other nuts and seeds, vegetable oils, wheat germ, peanut butter, avocado, and leafy greens such as spinach. The adult recommended intake is about 15 mg of alpha-tocopherol per day (roughly 22 IU of the natural form). For the well-fed, this alone keeps the retina supplied. (See Vitamin E food sources.)
- High-dose oral supplementation, for malabsorption. In cystic fibrosis, cholestatic liver disease, and similar conditions, ordinary doses cannot get past the absorption block, so clinicians use substantially higher oral doses — and sometimes a water-miscible form of vitamin E that is absorbed even when fat absorption is poor. In abetalipoproteinemia, large daily doses of vitamin E are the cornerstone of treatment and were shown decades ago to prevent the retinopathy when begun early (Runge et al., 1986; Granot & Kohen, 2004).
- Lifelong replacement, for the genetic forms. In AVED, vitamin E must be taken for life because the body cannot retain its own; consistent supplementation can halt and sometimes improve the neurological and retinal disease (Schuelke et al., 1999).
- Treat the whole deficiency picture. Because the fat-soluble vitamins travel together, vitamin A, D, and K are usually checked and replaced alongside E — and correcting vitamin A matters independently for night vision.
- Fix the underlying cause where possible. Pancreatic enzyme replacement in cystic fibrosis, a gluten-free diet in celiac disease, and management of cholestatic liver disease all improve absorption and help keep vitamin E up.
A word of realism: restoring vitamin E reliably prevents further photoreceptor loss and can stabilize vision, but it cannot regrow photoreceptors that have already died. That is precisely why the discovery of a low vitamin E level in someone losing vision is treated with urgency — every month of deficiency caught and reversed is retina saved. A caution in the other direction also applies: very high-dose vitamin E should be taken only under medical supervision, because excess vitamin E carries its own risks — chiefly an increased tendency to bleed (it interferes with vitamin K–dependent clotting). See the Vitamin E toxicity hub for the other side of the dose curve.
When to Seek Care / Red Flags
Vitamin E retinopathy itself is slow and painless, so the “red flags” here are less about a single emergency and more about not letting treatable vision loss slide — and about recognizing the few eye symptoms that always need prompt evaluation regardless of cause. Seek medical attention if you have:
- New or worsening trouble seeing at night, or a sense that your side vision is narrowing — especially if you also have a digestive/malabsorption condition, balance problems, or a family history of retinal disease. This is the pattern that should prompt both an eye exam and a vitamin E (and vitamin A) level.
- Any vitamin E retinopathy already diagnosed — this is a reason to be proactive, not to wait: get the deficiency corrected and the cause treated quickly, because preserved photoreceptors cannot be recovered once lost.
- Unsteady walking, numbness, or clumsiness developing alongside the vision changes — this suggests the deficiency is also damaging the nervous system and warrants prompt assessment (see Nerve Damage & Ataxia).
And separately, the following eye symptoms are not typical of slow vitamin E retinopathy and are urgent in their own right — treat them as an emergency and be seen the same day:
- Sudden loss of vision in one or both eyes.
- A shower of new floaters, flashing lights, or a dark “curtain” coming across your vision — possible signs of a retinal detachment.
- A painful red eye, or sudden severe eye pain with halos around lights — possible acute glaucoma.
The guiding idea is simple: gradual night-vision and side-vision loss deserves a careful, unhurried workup that includes checking vitamin E when the context fits — but any sudden change in vision is an emergency no matter what your vitamin levels are.
Key Research Papers
- Runge P, Muller DP, McAllister J, et al. (1986). Oral vitamin E supplements can prevent the retinopathy of abetalipoproteinaemia. British Journal of Ophthalmology;70(3):166-173. — DOI: 10.1136/bjo.70.3.166
- Yokota T, Shiojiri T, Gotoda T, et al. (1996). Retinitis Pigmentosa and Ataxia Caused by a Mutation in the Gene for the α-Tocopherol–Transfer Protein. New England Journal of Medicine;335(23):1770-1771. — DOI: 10.1056/nejm199612053352315
- Yokota T (2000). Postmortem study of ataxia with retinitis pigmentosa by mutation of the α-tocopherol transfer protein gene. Journal of Neurology, Neurosurgery & Psychiatry;68(4):521-525. — DOI: 10.1136/jnnp.68.4.521
- Granot E, Kohen R (2004). Oxidative stress in abetalipoproteinemia patients receiving long-term vitamin E and vitamin A supplementation. The American Journal of Clinical Nutrition;79(2):226-230. — DOI: 10.1093/ajcn/79.2.226
- Sokol RJ (1988). Vitamin E Deficiency and Neurologic Disease. Annual Review of Nutrition;8:351-373. — DOI: 10.1146/annurev.nu.08.070188.002031
- Iannaccone ST, Sokol RJ (1986). Vitamin E deficiency in neuropathy of abetalipoproteinemia. Neurology;36(7):1009. — DOI: 10.1212/wnl.36.7.1009
- Sokol RJ, Heubi JE, Balistreri WF (1983). Vitamin E deficiency in cholestatic liver disease. The Journal of Pediatrics;103(4):663-664. — DOI: 10.1016/s0022-3476(83)80622-2
- Alvarez F, Landrieu P, Feo C, et al. (1985). Vitamin E deficiency is responsible for neurologic abnormalities in cholestatic children. The Journal of Pediatrics;107(3):422-425. — DOI: 10.1016/s0022-3476(85)80525-4
- Traber MG, Atkinson J (2007). Vitamin E, antioxidant and nothing more. Free Radical Biology and Medicine;43(1):4-15. — DOI: 10.1016/j.freeradbiomed.2007.03.024
- Brigelius-Flohé R, Traber MG (1999). Vitamin E: function and metabolism. The FASEB Journal;13(10):1145-1155. — DOI: 10.1096/fasebj.13.10.1145
- Hoshino M, Masuda N, Ito Y, et al. (1999). Ataxia with isolated vitamin E deficiency: a Japanese family carrying a novel mutation in the α-tocopherol transfer protein gene. Annals of Neurology;45(6):809-812. — DOI: 10.1002/1531-8249(199906)45:6<809::aid-ana19>3.0.co;2-9
- Schuelke M, Mayatepek E, Inter M, et al. (1999). Treatment of ataxia in isolated vitamin E deficiency caused by α-tocopherol transfer protein deficiency. The Journal of Pediatrics;134(2):240-244. — DOI: 10.1016/s0022-3476(99)70424-5
PubMed Topic Searches
- PubMed — Vitamin E deficiency and retinopathy
- PubMed — Abetalipoproteinemia, retinitis pigmentosa, and vitamin E
- PubMed — α-tocopherol transfer protein, retinitis pigmentosa, and ataxia
- PubMed — Vitamin E, night blindness, and malabsorption
- PubMed — Vitamin E, photoreceptors, and retinal lipid peroxidation
Connections
- Vitamin E Deficiency Hub
- Vitamin E Deficiency: Nerve Damage & Ataxia
- Vitamin E Deficiency: Muscle Weakness
- Vitamin E Deficiency: Hemolytic Anemia
- Vitamin E Toxicity
- Vitamin E Overview
- Vitamin E Food Sources
- Vitamin A and Vision
- Vitamin A Overview
- Ophthalmology (Eye Diseases)
- Macular Degeneration
- Diabetic Retinopathy
- Cystic Fibrosis
- Celiac Disease
- Liver Disease
- Almonds