Health Benefits of Olive Oil

Interactive Visualization Cholesterol & the Artery Wall — watch a plaque form Follow LDL particles into the artery wall and see foam cells build plaque — then add a statin and watch the receptors clear them. Launch → Interactive Visualization Bile Acids — emulsify a fatty meal yourself Eat a fatty meal and watch bile squirt from the gallbladder to emulsify the fat into droplets lipase can attack — then block the bile and watch the fat, and vitamins A, D, E and K, go straight through. Launch →
Table of Contents
- Introduction and History
- Nutritional Profile
- Heart Health
- Anti-Inflammatory Properties
- Brain Health and Neuroprotection
- Cancer Prevention
- Blood Sugar and Diabetes
- Bone Health
- Digestive Health
- Historical Medical Use (1926)
- Skin and Hair Health
- Weight Management
- Antioxidant Properties
- Extra Virgin vs Refined Olive Oil
- Cooking with Olive Oil
- Choosing Quality Olive Oil
- Potential Considerations
- Scientific References
- Research Papers
- Connections
- Featured Videos
Introduction and History
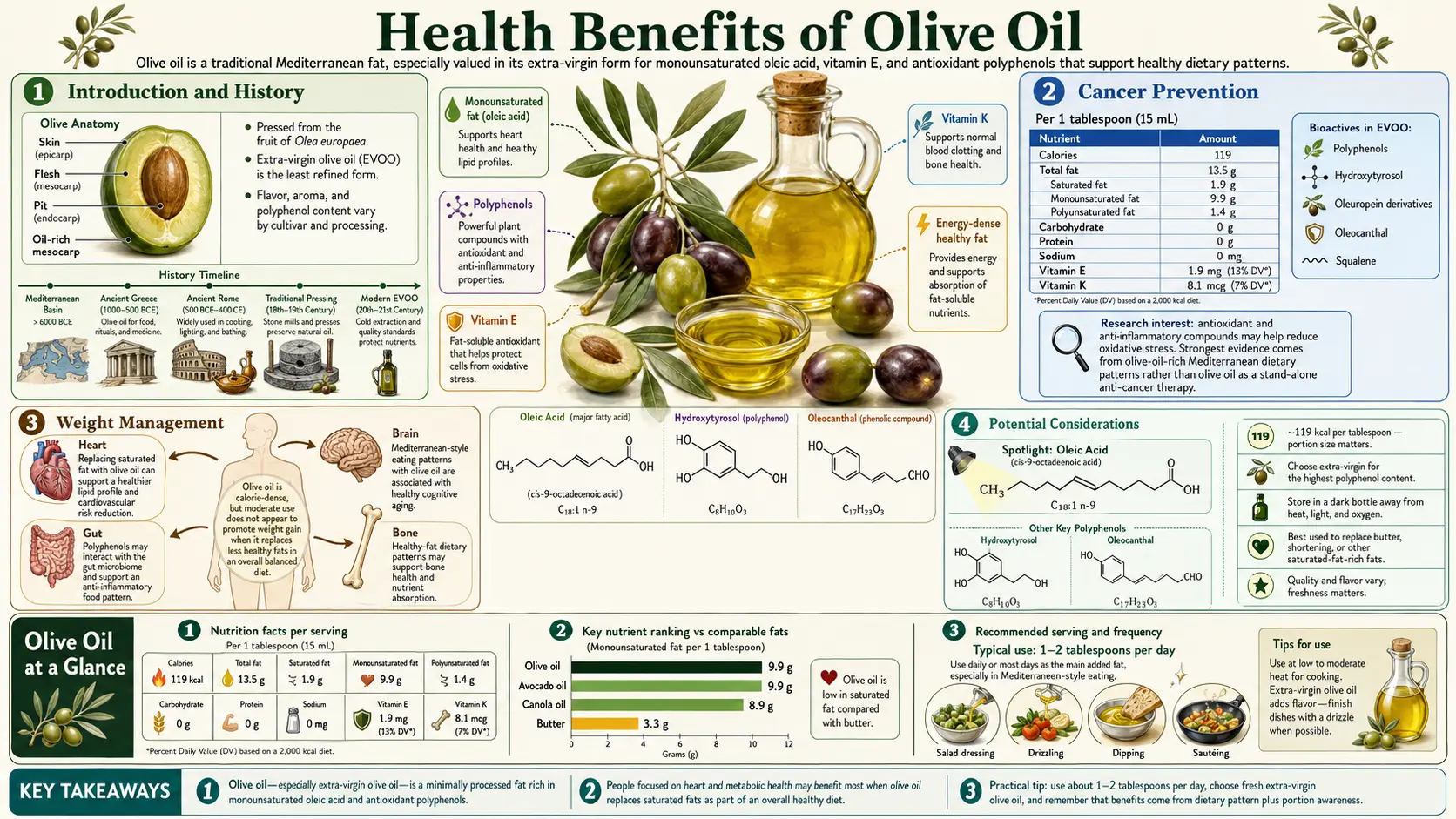
Olive oil stands as one of the oldest and most revered foods in human history, with a legacy stretching back approximately 6,000 years to the ancient civilizations of the eastern Mediterranean. Archaeological evidence suggests that olive cultivation began around 4000 BCE in the regions of modern-day Syria, Palestine, and Crete. The olive tree, Olea europaea, quickly became a symbol of peace, wisdom, and prosperity throughout the ancient world, and the oil pressed from its fruit served as a cornerstone of daily life for millennia.
In ancient Greece, olive oil was far more than a food. It was used to anoint athletes, fuel lamps, and serve as a base for perfumes and medicines. Homer referred to it as "liquid gold," and Hippocrates prescribed it for dozens of ailments. The Romans expanded olive cultivation throughout their empire, establishing vast groves across North Africa, Iberia, and southern Gaul. Roman writers such as Pliny the Elder and Columella documented elaborate olive pressing techniques and quality grading systems that foreshadowed modern standards. Biblical references to olive oil are abundant, appearing more than 140 times in Scripture, from the anointing of kings to the parable of the wise and foolish virgins.
Today, olive oil remains the cornerstone of the Mediterranean diet, a dietary pattern recognized by UNESCO as an Intangible Cultural Heritage of Humanity. Countries such as Spain, Italy, Greece, Tunisia, and Turkey produce the vast majority of the world's olive oil, with global production exceeding three million metric tons annually. The Mediterranean diet, rich in olive oil, fruits, vegetables, legumes, and fish, has been extensively studied since Ancel Keys' landmark Seven Countries Study in the 1960s and is consistently associated with reduced rates of cardiovascular disease, cancer, and all-cause mortality.
The modern scientific interest in olive oil accelerated dramatically in the late twentieth and early twenty-first centuries as researchers began isolating and characterizing its unique bioactive compounds. Beyond its well-known monounsaturated fatty acid content, extra virgin olive oil contains a complex matrix of polyphenols, tocopherols, phytosterols, and other micronutrients that work synergistically to promote health. This article explores the extensive body of research documenting the health benefits of olive oil across multiple organ systems and disease states.
Nutritional Profile
The dominant fatty acid in olive oil is oleic acid (C18:1), a monounsaturated omega-9 fatty acid that typically comprises 55 to 83 percent of total fatty acids. Oleic acid is responsible for many of olive oil's cardiovascular benefits, including its ability to lower LDL cholesterol while maintaining or raising HDL cholesterol. Olive oil also contains smaller amounts of palmitic acid (7.5 to 20 percent), linoleic acid (3.5 to 21 percent), stearic acid (0.5 to 5 percent), and alpha-linolenic acid (up to 1.5 percent). This fatty acid composition gives olive oil exceptional oxidative stability compared to polyunsaturated-rich oils.
The polyphenol fraction of extra virgin olive oil is perhaps its most distinctive nutritional feature. Key polyphenolic compounds include hydroxytyrosol, tyrosol, oleuropein aglycone, oleacein, and oleocanthal. Hydroxytyrosol is one of the most potent natural antioxidants known, with an oxygen radical absorbance capacity (ORAC) value significantly higher than that of vitamins C and E. Oleocanthal, the compound responsible for the characteristic peppery throat sensation of high-quality extra virgin olive oil, has garnered particular scientific attention for its anti-inflammatory and anticancer properties. Polyphenol concentrations in extra virgin olive oil typically range from 50 to 800 milligrams per kilogram, depending on cultivar, harvest timing, and processing methods.
Olive oil is a notable dietary source of vitamin E, primarily in the form of alpha-tocopherol, providing approximately 1.9 milligrams per tablespoon (about 13 percent of the daily recommended intake). It also contains vitamin K, contributing roughly 8.1 micrograms per tablespoon (about 7 percent of the daily value). These fat-soluble vitamins play essential roles in antioxidant defense and blood coagulation, respectively, and their absorption is enhanced by the lipid matrix of the oil itself.
Squalene is another significant bioactive component, present in olive oil at concentrations of 200 to 7,500 milligrams per kilogram, far exceeding levels found in other vegetable oils. Squalene is a triterpene hydrocarbon that serves as a precursor to cholesterol synthesis in the body and has demonstrated antioxidant, cardioprotective, and chemopreventive properties in experimental studies. Additionally, olive oil contains phytosterols such as beta-sitosterol, campesterol, and stigmasterol, which compete with cholesterol for intestinal absorption and contribute to the oil's cholesterol-lowering effects.
A single tablespoon of olive oil (approximately 13.5 grams) provides about 119 calories, 13.5 grams of total fat, 9.9 grams of monounsaturated fat, 1.4 grams of polyunsaturated fat, and 1.9 grams of saturated fat. It contains no carbohydrates, protein, fiber, or cholesterol. While calorie-dense, olive oil's exceptional nutrient density in terms of bioactive compounds distinguishes it from other culinary fats and justifies its central role in health-promoting dietary patterns.
Heart Health
The cardiovascular benefits of olive oil have been documented in some of the most rigorous dietary intervention trials ever conducted. The PREDIMED (Prevención con Dieta Mediterránea) trial, published in the New England Journal of Medicine in 2013 and republished with corrections in 2018, enrolled 7,447 participants at high cardiovascular risk across Spain. Participants randomized to a Mediterranean diet supplemented with extra virgin olive oil (approximately one liter per week) experienced a 31 percent relative reduction in the composite endpoint of myocardial infarction, stroke, and cardiovascular death compared to the control diet group. This landmark study provided some of the strongest evidence to date for a specific dietary fat in cardiovascular disease prevention.
Olive oil's heart-protective mechanisms are multifaceted. Oleic acid reduces LDL cholesterol levels while preserving or increasing HDL cholesterol, improving the overall lipid profile. A meta-analysis published in the Journal of the American College of Cardiology found that each 25-gram daily increase in olive oil consumption was associated with a 14 percent lower risk of cardiovascular disease and an 18 percent lower risk of coronary heart disease. The polyphenols in extra virgin olive oil further enhance these benefits by preventing the oxidation of LDL particles, a critical early step in atherosclerotic plaque formation.
Blood pressure regulation is another important cardiovascular mechanism. Multiple randomized controlled trials have demonstrated that regular consumption of polyphenol-rich olive oil produces modest but clinically significant reductions in both systolic and diastolic blood pressure. A study published in Archives of Internal Medicine found that participants consuming virgin olive oil were able to reduce their antihypertensive medication dosage by 48 percent, compared to just 4 percent in the sunflower oil control group. The nitric oxide-enhancing properties of olive oil polyphenols, which promote vasodilation, are believed to underlie this antihypertensive effect.
Stroke prevention represents another area where olive oil has demonstrated clear benefit. The Three-City Study, a prospective cohort of 7,625 French participants aged 65 and older, found that intensive olive oil users (using olive oil for both cooking and dressings) had a 41 percent lower risk of ischemic stroke compared to those who never used olive oil, after adjustment for diet quality, physical activity, and body mass index. The PREDIMED trial similarly reported a 33 percent reduction in stroke risk in the extra virgin olive oil group. These findings are consistent with olive oil's beneficial effects on endothelial function, platelet aggregation, and thrombotic tendency.
Beyond these established mechanisms, emerging research suggests that olive oil may also protect the heart through favorable effects on cardiac arrhythmia risk, arterial stiffness, and cardiac remodeling after injury. The totality of evidence has led the U.S. Food and Drug Administration to authorize a qualified health claim stating that consuming about two tablespoons (23 grams) of olive oil daily may reduce the risk of coronary heart disease.
Anti-Inflammatory Properties
One of the most remarkable discoveries about olive oil came in 2005 when researchers Gary Beauchamp and Paul Breslin at the Monell Chemical Senses Center identified oleocanthal as a potent natural anti-inflammatory agent. They noticed that freshly pressed extra virgin olive oil produced a distinctive throat-stinging sensation strikingly similar to that caused by ibuprofen solutions. Subsequent laboratory analysis confirmed that oleocanthal inhibits cyclooxygenase (COX) enzymes, the same molecular targets as ibuprofen and other nonsteroidal anti-inflammatory drugs (NSAIDs). Approximately 50 milliliters of extra virgin olive oil provides an oleocanthal dose pharmacologically equivalent to about 10 percent of a standard adult ibuprofen dose.
While this anti-inflammatory potency may seem modest on a per-dose basis, researchers emphasize that the cumulative effect of daily olive oil consumption over years and decades is likely substantial. Chronic low-grade inflammation, sometimes termed "inflammaging," is now understood to be a fundamental driver of atherosclerosis, type 2 diabetes, Alzheimer's disease, cancer, and many other age-related conditions. Regular consumption of oleocanthal-rich olive oil may help attenuate this chronic inflammatory state, potentially explaining the lower rates of these diseases observed in Mediterranean populations.
Beyond oleocanthal, other olive oil polyphenols also exhibit potent anti-inflammatory activity. Oleacein, hydroxytyrosol, and oleuropein have all been shown to suppress the nuclear factor kappa-B (NF-kB) signaling pathway, a master regulator of inflammatory gene expression. These compounds reduce the production of pro-inflammatory cytokines including tumor necrosis factor alpha (TNF-alpha), interleukin-1 beta (IL-1B), and interleukin-6 (IL-6). A randomized clinical trial published in the European Journal of Clinical Nutrition demonstrated that participants consuming high-polyphenol olive oil for three weeks had significantly lower levels of inflammatory biomarkers, including thromboxane B2 and leukotriene B4, compared to those consuming low-polyphenol olive oil.
The anti-inflammatory properties of olive oil have also been investigated in the context of rheumatoid arthritis and other autoimmune conditions. Animal studies have shown that oleocanthal can reduce cartilage destruction and joint inflammation in models of arthritis. Epidemiological data from Mediterranean countries, where olive oil consumption is highest, consistently show lower rates of rheumatoid arthritis compared to northern European and North American populations. While these observational associations cannot establish causation, they provide a compelling rationale for further clinical investigation of olive oil as an adjunctive dietary strategy in inflammatory conditions.
Brain Health and Neuroprotection
The relationship between olive oil consumption and brain health has become an increasingly active area of neuroscience research. The PREDIMED-NAVARRA trial, a subcohort of the larger PREDIMED study, assessed cognitive function in 522 participants over a mean follow-up of 6.5 years. Participants in the Mediterranean diet plus extra virgin olive oil group demonstrated significantly better cognitive performance on tests of memory, executive function, and global cognition compared to the control group. Notably, the olive oil group showed trajectories consistent with maintenance of cognitive function, while the control group exhibited typical age-related decline.
Alzheimer's disease research has identified several mechanisms by which olive oil compounds may protect against neurodegeneration. Oleocanthal has been shown in laboratory studies to enhance the clearance of amyloid-beta peptides from the brain by upregulating the expression of P-glycoprotein and LRP1, two key transport proteins at the blood-brain barrier. Amyloid-beta accumulation is a hallmark pathological feature of Alzheimer's disease, and enhancing its removal represents a promising therapeutic strategy. Additionally, oleocanthal inhibits the aggregation of tau protein, another key pathological marker of Alzheimer's and other tauopathies.
The blood-brain barrier, a highly selective membrane that protects the central nervous system from circulating toxins and pathogens, appears to benefit from olive oil consumption. Research published in ACS Chemical Neuroscience demonstrated that extra virgin olive oil supplementation in mouse models of Alzheimer's disease reduced blood-brain barrier permeability and enhanced the expression of tight junction proteins. These effects were accompanied by reduced neuroinflammation and improved synaptic integrity. Human epidemiological studies have corroborated these findings, with the Rush Memory and Aging Project reporting that participants who consumed more than one tablespoon of olive oil daily had a 28 percent lower risk of dying from dementia.
Hydroxytyrosol, one of the major polyphenols in olive oil, readily crosses the blood-brain barrier and has demonstrated neuroprotective effects in multiple experimental models. It protects neurons against oxidative damage, reduces mitochondrial dysfunction, and modulates neuroinflammatory pathways. In animal models of Parkinson's disease, hydroxytyrosol administration attenuated dopaminergic neuron loss and improved motor function. While these preclinical findings are promising, large-scale clinical trials in neurodegenerative disease populations are still needed to confirm the neuroprotective potential of olive oil polyphenols in humans.
Depression and mood disorders have also been linked to dietary patterns in epidemiological research. The SUN (Seguimiento Universidad de Navarra) cohort study, which followed over 12,000 Spanish university graduates, found that adherence to a Mediterranean diet rich in olive oil was associated with a significantly lower risk of developing clinical depression. The anti-inflammatory and antioxidant properties of olive oil, combined with its potential effects on serotonin receptor expression and brain-derived neurotrophic factor (BDNF) production, may contribute to these mood-related benefits.
Cancer Prevention
The potential cancer-preventive properties of olive oil have been investigated extensively, with both epidemiological and mechanistic evidence supporting a protective role. A comprehensive meta-analysis published in Scientific Reports in 2022, encompassing 45 observational studies, concluded that highest versus lowest olive oil consumption was associated with a 31 percent lower risk of any cancer, with particularly strong protective associations for breast cancer (a 28 percent reduction) and cancers of the digestive system (a 36 percent reduction). These associations remained significant after adjusting for overall dietary quality and other lifestyle factors.
Oleocanthal has emerged as a particularly intriguing anticancer compound. A landmark study published in Molecular and Cellular Oncology in 2015 demonstrated that oleocanthal caused rapid cancer cell death within 30 minutes to one hour by rupturing lysosomes, the cellular organelles responsible for waste processing. Remarkably, healthy non-cancerous cells were left unharmed, merely entering a temporary dormant state before resuming normal function. This selectivity was attributed to the inherent fragility of cancer cell lysosomes compared to those of normal cells. Subsequent studies have confirmed oleocanthal's anticancer effects against breast, prostate, colorectal, liver, and pancreatic cancer cell lines.
Breast cancer has been the most extensively studied cancer type in relation to olive oil. The PREDIMED trial reported a 62 percent relative risk reduction for breast cancer in the extra virgin olive oil supplementation group compared to the control diet, though the small number of cases (35 total) warranted cautious interpretation. Mechanistic studies suggest that olive oil polyphenols may reduce breast cancer risk by modulating estrogen metabolism, inhibiting HER2 oncogene expression, suppressing fatty acid synthase activity, and inducing apoptosis in malignant cells while sparing normal breast epithelium.
Colorectal cancer prevention by olive oil has been linked to multiple mechanisms, including the suppression of aberrant crypt foci formation (an early precursor to colorectal tumors), inhibition of colorectal cancer cell proliferation through downregulation of the Wnt/beta-catenin pathway, and favorable modulation of the gut microbiome. Prostate cancer research has similarly identified olive oil polyphenols as inhibitors of androgen receptor signaling and promoters of prostate cancer cell apoptosis. The antioxidant compounds in olive oil, particularly hydroxytyrosol, also protect DNA from oxidative damage, reducing the accumulation of cancer-initiating mutations over time.
It is important to note that while these findings are promising, most evidence derives from observational studies and laboratory experiments. The translation of in vitro anticancer effects to clinically meaningful cancer prevention in humans remains an active area of investigation. Nevertheless, the consistent protective associations observed across multiple cancer types and populations, combined with plausible biological mechanisms, support the inclusion of extra virgin olive oil as part of a cancer-preventive dietary strategy.
Blood Sugar and Diabetes
Olive oil consumption has demonstrated consistent benefits for blood sugar regulation and type 2 diabetes prevention. The PREDIMED trial found that participants randomized to the Mediterranean diet supplemented with extra virgin olive oil had a 40 percent lower incidence of new-onset type 2 diabetes compared to the control group. This finding was particularly notable because the intervention did not specifically target calorie restriction or weight loss, suggesting that the qualitative composition of dietary fat may be as important as total caloric balance in diabetes prevention.
The mechanisms underlying olive oil's antidiabetic effects involve improvements in both insulin sensitivity and beta-cell function. Oleic acid enhances insulin signaling by modifying cell membrane fluidity and improving insulin receptor function. In randomized crossover studies, meals containing olive oil produced significantly lower postprandial glucose excursions compared to meals containing butter or other saturated fats, even when total fat and caloric content were matched. A study published in Diabetes Care showed that a Mediterranean diet enriched with olive oil reduced fasting glucose levels by 0.39 mmol/L and HbA1c by 0.30 percent compared to a low-fat control diet.
The polyphenols in extra virgin olive oil provide additional glycemic benefits beyond those attributable to the fatty acid profile alone. Oleuropein and hydroxytyrosol have been shown to enhance glucose uptake in skeletal muscle cells through activation of AMPK (adenosine monophosphate-activated protein kinase), a key cellular energy sensor. These compounds also protect pancreatic beta cells from glucotoxicity and lipotoxicity, preserving insulin secretory capacity. Animal studies have demonstrated that olive oil polyphenol supplementation can prevent the progression from prediabetes to overt diabetes in high-fat diet models.
For individuals already living with type 2 diabetes, incorporating olive oil into the diet has shown meaningful clinical improvements. A systematic review and meta-analysis of 29 trials published in Nutrition and Diabetes concluded that olive oil consumption was associated with significant reductions in fasting blood glucose, fasting insulin, and HOMA-IR (a measure of insulin resistance) in people with type 2 diabetes. The European Food Safety Authority (EFSA) has recognized the benefits of olive oil polyphenols, authorizing a health claim that olive oil polyphenols contribute to the protection of blood lipids from oxidative stress when consumed at a dose providing at least 5 milligrams of hydroxytyrosol and its derivatives daily.
Bone Health
Emerging research has revealed that olive oil and its polyphenolic compounds play a meaningful role in bone health maintenance and osteoporosis prevention. Epidemiological studies consistently show that populations adhering to a Mediterranean diet rich in olive oil have higher bone mineral density and lower fracture rates compared to populations consuming Western-style diets. A large prospective cohort study from the PREDIMED trial found that participants in the olive oil supplementation group had a 51 percent lower risk of osteoporotic fractures over a median follow-up period of 8.9 years.
The polyphenols in olive oil, particularly oleuropein and hydroxytyrosol, have demonstrated direct effects on bone cell biology. In vitro studies show that these compounds stimulate osteoblast differentiation and proliferation while simultaneously inhibiting osteoclast formation and activity. Osteoblasts are the cells responsible for building new bone tissue, while osteoclasts are responsible for bone resorption. By shifting the balance toward bone formation, olive oil polyphenols may help maintain bone mass and structural integrity, particularly during the accelerated bone loss that accompanies menopause and aging.
Calcium absorption, a critical determinant of bone health, may also be enhanced by olive oil consumption. Fat-soluble vitamin D, essential for intestinal calcium absorption, requires dietary fat for optimal bioavailability. The monounsaturated fatty acids in olive oil provide an excellent lipid matrix for vitamin D absorption. Additionally, oleic acid has been shown in animal models to enhance intestinal calcium transport independent of vitamin D. Olive oil's content of vitamin K, which is required for the carboxylation of osteocalcin (a key bone matrix protein), further supports its role in skeletal health.
Oxidative stress and chronic inflammation are now recognized as important contributors to age-related bone loss. The antioxidant and anti-inflammatory properties of olive oil polyphenols address both of these pathogenic mechanisms. A randomized controlled trial in postmenopausal women with osteopenia found that supplementation with olive oil polyphenols for 12 months significantly reduced serum markers of bone resorption (C-terminal telopeptide of type I collagen) and increased serum osteocalcin, suggesting a favorable shift in bone turnover. While further research is needed, these findings support olive oil as a dietary strategy for preserving skeletal health throughout the lifespan.
Digestive Health
Olive oil has been used as a digestive aid in traditional Mediterranean medicine for centuries, and modern research is beginning to validate many of these historical practices. One of olive oil's primary digestive functions is the stimulation of bile production and secretion. Bile acids, produced by the liver and stored in the gallbladder, are essential for the emulsification and absorption of dietary fats and fat-soluble vitamins. The oleic acid in olive oil is a potent choleretic, stimulating bile flow and promoting efficient fat digestion. This gentle stimulation of biliary function is one reason olive oil is generally better tolerated than other dietary fats by individuals with digestive sensitivities.
The relationship between olive oil and the gut microbiome has emerged as a particularly exciting area of investigation. A randomized controlled trial published in Clinical Nutrition found that three weeks of extra virgin olive oil consumption increased the abundance of beneficial bacterial genera, including Bifidobacterium and Lactobacillus, while reducing populations of potentially pathogenic species. The polyphenols in olive oil, many of which are poorly absorbed in the small intestine and reach the colon intact, appear to act as prebiotics, selectively nourishing beneficial bacteria. These shifts in microbial composition were accompanied by increased production of short-chain fatty acids, which serve as fuel for colonocytes and exert anti-inflammatory effects throughout the body.
Olive oil has shown notable activity against Helicobacter pylori, the bacterium responsible for most peptic ulcers and a significant risk factor for gastric cancer. In vitro studies have demonstrated that olive oil polyphenols, particularly the dialdehydic form of decarboxymethyl oleuropein aglycone, exhibit bactericidal activity against multiple strains of H. pylori, including antibiotic-resistant strains. A clinical study from Spain showed that consumption of 30 grams of virgin olive oil daily for 14 days reduced H. pylori colonization in a significant proportion of infected individuals. While olive oil cannot replace standard triple therapy for H. pylori eradication, it may serve as a useful adjunctive or preventive measure.
Gallstone prevention is another digestive benefit associated with olive oil consumption. Gallstones form when bile becomes supersaturated with cholesterol, and dietary factors that improve bile composition can reduce gallstone risk. Olive oil promotes biliary cholesterol secretion while simultaneously increasing bile acid output, resulting in a less lithogenic bile composition. Epidemiological studies from Mediterranean countries, where olive oil is the predominant culinary fat, consistently report lower rates of gallstone disease compared to Northern European and North American populations. A case-control study published in the American Journal of Epidemiology found that women in the highest quartile of monounsaturated fat intake had a 20 percent lower risk of cholecystectomy for symptomatic gallstones.
Historical Medical Use (1926 U.S. Dispensatory)
Olive oil has a documented place in early-twentieth-century American medicine. In the United States Dispensatory of 1926 — the era's authoritative drug reference, compiled when roughly three-quarters of the listed remedies were still natural substances — olive oil (then catalogued by its pharmacy name, Oleum Olivae) was used as a gentle internal medicine, not merely as a food. Physicians of the day recognized two uses in particular, and it is worth presenting them honestly as history: they describe what doctors believed and did a century ago, which is true even where the underlying reasoning has since been refined or overturned.
First, olive oil was given as a mild laxative for constipation. A dose of olive oil swallowed on an empty stomach was thought to lubricate the bowel and ease the passage of stool. Second, and more ambitiously, large doses of olive oil were prescribed for gallstones. The reasoning was mechanical and partly correct: dietary fat entering the small intestine triggers the gallbladder to contract and release a surge of bile. Nineteenth- and early-twentieth-century clinicians reasoned that this fat-driven flood of bile might help wash a stone out of the bile ducts, and some hoped the oil could even soften or dissolve a stone. Period authors did, to their credit, add a caution that survives as good advice today: if a large stone is already lodged in and obstructing a duct, forcing the gallbladder to squeeze harder can raise pressure behind the blockage and cause harm rather than relief.
What modern evidence says. The kernel of truth is real. Olive oil is a genuine choleretic — the oleic acid in it stimulates the release of cholecystokinin, which makes the gallbladder contract and bile flow, exactly as described in the Digestive Health section above. Olive oil also has a mild lubricant-laxative effect when taken in quantity, so the constipation use was not pure folklore. Over the long term, a diet rich in olive oil is even associated with fewer gallstones, because it shifts bile toward a less cholesterol-saturated, less stone-forming composition.
But the popular “liver flush” or “gallbladder cleanse” is a myth. The 1926 idea later mutated into a widespread alternative-medicine ritual in which a person drinks a large volume of olive oil together with lemon or other fruit juice and then passes soft green or tan pellets, which are triumphantly displayed as “dissolved gallstones.” They are not gallstones. When researchers actually analyzed these pellets, they found no cholesterol, no bilirubin, no calcium, and no crystalline structure — none of the hallmarks of a true gallstone. Instead, the pellets are saponified oil: digestive enzymes split the olive oil into fatty acids, which then combine with potassium from the citrus juice to form soft soap-like clumps in the gut. In a much-cited 2005 Lancet report, a woman who completed such a “cleanse” passed numerous green “stones” that chemical analysis showed to be exactly these saponified soaps, not biliary calculi. A flush does not remove gallstones; it manufactures soft pellets that merely look like them.
Safety caveat the old (and the modern marketing) framing omits. A genuinely obstructing gallstone — one that blocks the bile duct, causing severe pain, fever, jaundice, or a yellowing of the eyes and skin — is a medical emergency that can lead to infection (cholangitis) or pancreatitis. It needs urgent evaluation and usually a procedure (ERCP) or surgery, not a kitchen remedy. Attempting an olive-oil flush in that situation wastes critical time and, by forcing the gallbladder to contract against a blockage, may make things worse — the very back-pressure danger the 1926 authors flagged. Olive oil is superb food and a sensible everyday fat, and its long-term dietary role genuinely lowers gallstone risk; but it is not a treatment for stones you already have. If you suspect gallstones, see a clinician for an ultrasound rather than attempting a flush.
Citations
- Sies CW, Brooker J. “Could these be gallstones?” The Lancet, 2005;365(9468):1388. (Pellets passed after an olive-oil-and-lemon-juice “liver cleanse” contained no cholesterol, bilirubin, calcium, or crystal structure — they were saponified fatty-acid soaps, not gallstones.) [VERIFIED]
- Dekkers R. “Apple juice and the chemical-contact softening of gallstones.” The Lancet, 1999;354(9196):2171. (Correspondence on the “gallstone-softening” folk regimens that combine oils and fruit juices, situating the modern flush within this debunked tradition.) [VERIFIED]
- Olive oil, cholecystokinin, and gallbladder contraction (PubMed search) — literature on olive oil's genuine choleretic, bile-stimulating effect. [SEARCHLINK]
Skin and Hair Health
Olive oil has been prized for its cosmetic and dermatological applications since antiquity, when Greek athletes would coat their skin with olive oil before competition and Roman women used it as a moisturizer and hair treatment. The skin benefits of olive oil derive largely from its high squalene content, which closely resembles the squalene naturally produced by human sebaceous glands. Squalene constitutes approximately 12 percent of human skin surface lipids and plays a crucial role in maintaining skin hydration, elasticity, and barrier function. The squalene in olive oil is readily absorbed by the skin and may help replenish declining endogenous production that occurs with aging.
Vitamin E, present in olive oil primarily as alpha-tocopherol, is one of the most important lipid-soluble antioxidants in human skin. It protects cell membranes from ultraviolet radiation-induced lipid peroxidation, a primary driver of photoaging. When consumed dietarily, vitamin E accumulates in the stratum corneum and epidermis, providing systemic photoprotection. Studies have shown that regular olive oil consumption is associated with reduced skin photoaging, with a French cohort study finding that women with the highest monounsaturated fat intake had significantly less severe facial skin aging compared to those with the lowest intake, after adjusting for sun exposure and smoking status.
The anti-aging properties of olive oil extend beyond simple photoprotection. Hydroxytyrosol has been shown to activate the Nrf2 pathway, a master regulator of cellular antioxidant defenses, in skin fibroblasts. This activation increases the production of endogenous antioxidant enzymes such as glutathione peroxidase, catalase, and superoxide dismutase. Additionally, oleocanthal's anti-inflammatory properties may help mitigate the chronic low-grade skin inflammation that contributes to collagen degradation and wrinkle formation. Topically applied olive oil has demonstrated efficacy in improving skin barrier function and reducing transepidermal water loss in clinical studies, though it should be noted that application to already-compromised skin (as in atopic dermatitis) may sometimes impair barrier recovery.
For hair health, olive oil's benefits are attributed to its ability to penetrate the hair shaft more effectively than many other oils. Research published in the Journal of Cosmetic Science found that monounsaturated oils like olive oil can penetrate the hair cortex due to their straight-chain fatty acid structure, reducing protein loss during washing and chemical treatment. Olive oil's vitamin E content also helps protect the scalp from oxidative damage, and its anti-inflammatory polyphenols may benefit individuals with inflammatory scalp conditions. Traditional Mediterranean hair care practices using olive oil as a pre-wash treatment continue to be supported by modern cosmetic science research.
Weight Management
Despite its caloric density, olive oil consumption is not associated with weight gain in the vast majority of epidemiological studies and clinical trials. The PREDIMED trial, in which participants consumed an additional liter of extra virgin olive oil per week (approximately 340 extra calories daily) without specific caloric restriction, found no significant weight gain in the olive oil group over the multi-year study period. In fact, the olive oil group experienced modest reductions in waist circumference compared to the control group, suggesting favorable effects on body fat distribution even without weight loss.
Several mechanisms may explain why olive oil does not contribute to weight gain despite its high caloric content. Oleic acid has been shown to promote satiety through the production of oleoylethanolamide (OEA), a lipid signaling molecule synthesized in the small intestine upon oleic acid absorption. OEA activates peroxisome proliferator-activated receptor alpha (PPAR-alpha) in the gut and sends satiety signals to the brain via the vagus nerve, reducing appetite and food intake at subsequent meals. This oleic acid-OEA-satiety pathway may represent an important mechanism by which Mediterranean-style diets rich in olive oil achieve weight maintenance without deliberate caloric restriction.
Olive oil may also influence body composition through effects on fat metabolism and thermogenesis. Animal studies have demonstrated that oleic acid-rich diets promote greater fat oxidation compared to saturated fat-rich diets, channeling dietary fat toward energy production rather than storage. A randomized crossover study in humans found that a meal containing olive oil resulted in significantly higher postprandial energy expenditure (diet-induced thermogenesis) compared to an isocaloric meal containing cream. Furthermore, olive oil polyphenols have been shown to activate brown adipose tissue and promote "browning" of white adipose tissue in animal models, enhancing non-shivering thermogenesis.
Clinical weight management studies consistently support the superiority of Mediterranean-style diets rich in olive oil over conventional low-fat diets. A landmark two-year randomized trial published in the New England Journal of Medicine found that a calorie-unrestricted Mediterranean diet produced comparable weight loss to a calorie-restricted low-fat diet, with superior improvements in cardiovascular risk markers. Longer-term follow-up studies have shown better dietary adherence and weight maintenance with Mediterranean and olive oil-rich diets compared to restrictive low-fat approaches, likely because the palatability and satiety-promoting properties of olive oil improve long-term dietary compliance.
Antioxidant Properties
Extra virgin olive oil contains a remarkable array of antioxidant compounds that work through multiple complementary mechanisms to neutralize reactive oxygen species and protect biological molecules from oxidative damage. The principal antioxidant polyphenols include hydroxytyrosol, tyrosol, oleuropein (and its aglycone derivatives), oleacein, and oleocanthal. Among these, hydroxytyrosol stands out as one of the most potent natural antioxidants ever characterized, with in vitro radical scavenging activity approximately ten times greater than that of green tea catechins and roughly twice that of coenzyme Q10.
Tyrosol, while less potent than hydroxytyrosol as a direct radical scavenger, contributes significantly to olive oil's antioxidant capacity due to its greater abundance and excellent bioavailability. In vivo, tyrosol can be converted to hydroxytyrosol by the enzyme cytochrome P450 2A6, effectively extending its antioxidant potency after absorption. Oleuropein and its derivatives represent another major class of olive oil antioxidants, demonstrating potent metal-chelating activity that prevents iron and copper ions from catalyzing the generation of hydroxyl radicals through Fenton chemistry. This metal-chelating capacity is particularly relevant to the prevention of neurodegenerative diseases, where iron accumulation in specific brain regions is a recognized pathogenic factor.
One of the most clinically relevant antioxidant functions of olive oil polyphenols is the prevention of LDL cholesterol oxidation. Oxidized LDL is far more atherogenic than native LDL, as it is readily taken up by macrophages in the arterial wall, forming foam cells that constitute the earliest stage of atherosclerotic plaque development. The European Food Safety Authority (EFSA) formally recognized this benefit, approving a health claim that olive oil polyphenols protect blood lipids from oxidative stress. To qualify for this claim, an olive oil must provide at least 5 milligrams of hydroxytyrosol and its derivatives (including oleuropein complex and tyrosol) per 20 grams of olive oil consumed daily.
Beyond direct radical scavenging, olive oil polyphenols upregulate endogenous antioxidant defense systems through activation of the Nrf2 (nuclear factor erythroid 2-related factor 2) signaling pathway. When activated, Nrf2 translocates to the nucleus and induces the transcription of over 200 cytoprotective genes, including those encoding glutathione S-transferase, NAD(P)H quinone oxidoreductase 1, heme oxygenase-1, and the glutamate-cysteine ligase subunits required for glutathione synthesis. This indirect antioxidant mechanism amplifies the protective effects of olive oil far beyond what would be predicted from the direct radical-scavenging capacity of its polyphenols alone.
The synergistic interactions among olive oil's antioxidant compounds deserve emphasis. Vitamin E (alpha-tocopherol) acts as the primary chain-breaking antioxidant in lipid membranes, while polyphenols such as hydroxytyrosol regenerate oxidized vitamin E, creating an efficient antioxidant recycling system. Squalene contributes additional protection by quenching singlet oxygen, a particularly reactive oxygen species generated by ultraviolet radiation and enzymatic reactions. This multilayered antioxidant network, unique to extra virgin olive oil, provides comprehensive protection against the diverse forms of oxidative stress encountered in human physiology.
Extra Virgin vs Refined Olive Oil
Understanding the distinctions between extra virgin and refined olive oil is essential for making informed dietary choices. Extra virgin olive oil (EVOO) is obtained exclusively by mechanical means, typically through centrifugal extraction at temperatures below 27 degrees Celsius (cold extraction). It undergoes no chemical treatment, refining, or blending with other oils. To earn the "extra virgin" designation under International Olive Council (IOC) standards, the oil must have a free acidity (expressed as oleic acid) of no more than 0.8 percent, a peroxide value of no more than 20 milliequivalents of active oxygen per kilogram, and must pass both chemical and sensory evaluation panels confirming the absence of defects and the presence of positive fruitiness.
Refined olive oil, by contrast, is produced from lower-quality or defective virgin olive oils that do not meet extra virgin standards. The refining process involves degumming, neutralization with sodium hydroxide, bleaching with activated clays, and deodorization through steam distillation at temperatures exceeding 200 degrees Celsius. While this process removes off-flavors and reduces acidity, it also destroys the vast majority of polyphenolic compounds, tocopherols, chlorophyll, and other bioactive molecules. Refined olive oil retains the monounsaturated fatty acid profile of virgin olive oil but loses approximately 85 to 95 percent of its polyphenol content, depending on the severity of the refining process.
The commercially labeled "olive oil" (sometimes called "pure olive oil" or "classic olive oil") is typically a blend of refined olive oil with a small percentage (5 to 15 percent) of virgin or extra virgin olive oil added back for flavor and color. This blended product occupies a middle ground nutritionally, retaining the oleic acid content of olive oil but with polyphenol levels far below those of genuine extra virgin olive oil. "Light" or "extra light" olive oil is the most heavily refined, with virtually no flavor, color, or polyphenol content, differing from other refined vegetable oils primarily in its monounsaturated fat composition.
The health implications of these differences are significant. Many of the most impressive health benefits attributed to olive oil in clinical research, particularly those related to anti-inflammatory, antioxidant, anticancer, and neuroprotective effects, are driven primarily by the polyphenol fraction present in meaningful quantities only in extra virgin olive oil. The PREDIMED trial and other major intervention studies used extra virgin olive oil exclusively. While refined olive oil still provides cardiovascular benefits related to its oleic acid content (superior to those of butter or other saturated fat sources), choosing extra virgin olive oil maximizes the full spectrum of health benefits supported by the scientific literature.
Quality markers to look for in extra virgin olive oil include a harvest date (as opposed to merely a "best by" date), a clearly stated origin (single country, ideally single estate), polyphenol content expressed in milligrams per kilogram when available, and certifications from recognized quality bodies such as the California Olive Oil Council (COOC) or European PDO/PGI designations. A genuine extra virgin olive oil should have a noticeable peppery, bitter, or pungent quality, reflecting the presence of bioactive polyphenols. If the oil has no distinctive flavor or throat sensation, it is likely refined or degraded regardless of its label claims.
Cooking with Olive Oil
A persistent misconception holds that olive oil is unsuitable for cooking due to a supposedly low smoke point. In reality, the smoke point of extra virgin olive oil ranges from approximately 190 to 215 degrees Celsius (375 to 420 degrees Fahrenheit), which is well above the temperatures used for most home cooking methods, including sautéing, pan-frying, roasting, and even deep-frying. The smoke point of refined olive oil is even higher, approximately 240 degrees Celsius (465 degrees Fahrenheit). These temperatures are comparable to or higher than those of many other commonly used cooking oils, including coconut oil, butter, and unrefined sesame oil.
More importantly, smoke point alone is a poor predictor of cooking oil stability. Research published in ACTA Scientific Nutritional Health evaluated the performance of ten common cooking oils when heated to 240 degrees Celsius for extended periods, measuring the production of harmful polar compounds and secondary oxidation products. Extra virgin olive oil was found to be the most stable cooking oil tested, producing the fewest harmful compounds under heat stress, outperforming even refined oils with higher smoke points such as canola and sunflower oil. This superior thermal stability is attributed to olive oil's high monounsaturated fatty acid content (which resists oxidation far better than polyunsaturated fatty acids) and its natural antioxidant polyphenols, which protect the oil from degradation during cooking.
While some polyphenol degradation does occur during cooking, studies show that a significant proportion of bioactive compounds survive typical home cooking conditions. Research has demonstrated that extra virgin olive oil retains 40 to 70 percent of its phenolic compounds after moderate heating (around 180 degrees Celsius for 30 to 60 minutes). Furthermore, cooking with extra virgin olive oil enhances the transfer of fat-soluble nutrients from other ingredients. Vegetables sautéed in olive oil have been shown to deliver higher bioavailable levels of carotenoids, including beta-carotene and lycopene, compared to vegetables prepared by steaming or boiling alone.
For optimal health benefits, extra virgin olive oil is best used as an all-purpose cooking oil for daily meal preparation. It excels in sautéing vegetables and proteins at medium to medium-high heat, roasting at temperatures up to 200 degrees Celsius, making salad dressings and vinaigrettes, drizzling over finished dishes for flavor and nutritional enhancement, and preparing slow-cooked stews and sauces. For extended high-temperature deep-frying exceeding 190 degrees Celsius for prolonged periods, refined olive oil may be a more economical choice, though extra virgin olive oil can also perform this task safely and with superior results in terms of harmful compound formation.
Choosing Quality Olive Oil
Selecting a high-quality extra virgin olive oil requires attention to several key factors, as the global olive oil market has historically been plagued by fraud and mislabeling. Studies by the University of California, Davis Olive Center and other institutions have found that a significant percentage of imported olive oils labeled "extra virgin" in the United States fail to meet international standards for the designation, either due to oxidative degradation, adulteration with cheaper refined oils, or sensory defects that should have disqualified them from the extra virgin category.
The harvest date is the single most important indicator of freshness and quality. Unlike wine, olive oil does not improve with age. Its polyphenol content begins declining from the moment of pressing, with typical losses of 40 to 50 percent over the first 12 to 18 months. Look for a clearly printed harvest date (not merely a "best by" or "bottled on" date) and aim to consume the oil within 12 to 14 months of harvest. In the Northern Hemisphere, harvest typically occurs between October and January, while Southern Hemisphere oils are harvested between April and July, providing an opportunity for year-round access to freshly pressed olive oil.
Storage conditions significantly affect olive oil quality and shelf life. Olive oil is sensitive to light, heat, and oxygen, all of which accelerate oxidative degradation and polyphenol loss. Choose oils packaged in dark glass bottles, tins, or bag-in-box containers that limit light exposure. After opening, store olive oil in a cool, dark location (ideally between 14 and 18 degrees Celsius) with the cap tightly sealed to minimize oxygen contact. Avoid storing olive oil near the stove, on a windowsill, or in any location subject to temperature fluctuations. Properly stored, an unopened bottle of high-quality extra virgin olive oil can maintain its polyphenol content and sensory qualities for 18 to 24 months from harvest.
Third-party certifications provide additional assurance of quality. In the United States, the USDA Quality Monitoring Program and the California Olive Oil Council (COOC) seal indicate that the oil has been chemically tested and sensory evaluated by trained panels. In Europe, Protected Designation of Origin (PDO) and Protected Geographical Indication (PGI) labels certify that the oil meets specific regional production standards. International competition awards from recognized events such as the New York International Olive Oil Competition (NYIOOC) and Mario Solinas Quality Award also serve as reliable quality indicators.
To evaluate quality at home, pour a small amount of olive oil into a wine glass, warm it in your hands for about 30 seconds, and inhale the aroma. High-quality extra virgin olive oil should smell of fresh green olives, cut grass, herbs, artichoke, green apple, or similar vegetal notes. Defects such as mustiness, rancidity (reminiscent of old nuts or crayons), fustiness (fermented or swampy odor), or winey/vinegary notes indicate degradation or poor production. When tasted, genuine extra virgin olive oil should exhibit bitterness and pungency (the peppery throat catch), both of which are positive attributes directly correlated with polyphenol content. An oil that tastes bland, greasy, or waxy is unlikely to be a true extra virgin regardless of label claims.
Potential Considerations
While olive oil offers numerous health benefits, several practical considerations merit attention. First, olive oil is calorie-dense, providing approximately 119 calories per tablespoon. For individuals managing their weight through caloric control, olive oil should be used as a replacement for other less healthy fats rather than as an addition to an already calorie-sufficient diet. The health benefits observed in clinical trials such as PREDIMED were achieved within the context of an overall Mediterranean dietary pattern, not through olive oil supplementation alone. Pouring olive oil liberally over a diet otherwise rich in processed foods, refined carbohydrates, and saturated fats is unlikely to produce the same benefits.
Adulteration remains a significant concern in the global olive oil supply chain. Common forms of fraud include blending extra virgin olive oil with cheaper refined olive oil, hazelnut oil, or seed oils such as sunflower or canola oil, and selling the product at extra virgin prices. Deodorized (soft-column refined) olive oils are particularly difficult to detect because they pass standard chemical tests while lacking the polyphenol content and health benefits of genuine extra virgin oil. Consumers can mitigate this risk by purchasing from reputable producers with transparent supply chains, choosing oils with third-party quality certifications, and buying directly from domestic producers when possible.
Individuals with gallbladder disease or who have undergone cholecystectomy should be aware that olive oil, like all dietary fats, stimulates gallbladder contraction and bile release. While moderate olive oil consumption is generally well tolerated after the initial post-surgical adaptation period, consuming large quantities of any fat in a single sitting can cause digestive discomfort, including bloating, diarrhea, and abdominal cramping, in these individuals. A gradual increase in dietary fat intake and distribution across multiple meals throughout the day is recommended.
True olive oil allergy is extremely rare but has been documented in the medical literature. Most reported cases involve contact dermatitis from topical olive oil application rather than systemic allergic reactions from ingestion. Individuals with known allergies to other members of the Oleaceae family, which includes ash trees, jasmine, lilac, and privet, may theoretically be at slightly higher risk, though clinical cross-reactivity is uncommon. The more common scenario is intolerance rather than true allergy, with some individuals experiencing gastrointestinal discomfort from high-polyphenol olive oils due to their irritant effect on the gastrointestinal mucosa.
Finally, it should be noted that olive oil, while exceptionally healthful, is not a panacea. Its benefits are maximized when consumed as part of a balanced dietary pattern that includes abundant fruits, vegetables, legumes, whole grains, nuts, and fish, with limited intake of processed foods, added sugars, and excess sodium. The Mediterranean diet as a whole, rather than any single component, is responsible for the remarkable health outcomes observed in the populations that consume it. Olive oil is best understood as the central pillar of this dietary pattern, providing both direct biological benefits through its unique bioactive compounds and indirect benefits by making nutritious foods more palatable and enjoyable.
Scientific References
- Estruch R et al. "Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts" New England Journal of Medicine, 2018. (PREDIMED trial: Mediterranean diet with EVOO reduced major cardiovascular events by 31% in 7,447 high-risk participants.)
- Samieri C et al. "Olive oil consumption, plasma oleic acid, and stroke incidence: the Three-City Study" Neurology, 2011. (Intensive olive oil users had a 41% lower risk of ischemic stroke in a cohort of 7,625 French elderly participants.)
- Ferrara LA et al. "Olive oil and reduced need for antihypertensive medications" Archives of Internal Medicine, 2000. (Virgin olive oil diet reduced antihypertensive drug dosage by 48% compared to 4% with sunflower oil.)
- Beauchamp GK, Breslin PAS et al. "Phytochemistry: ibuprofen-like activity in extra-virgin olive oil" Nature, 2005. (Identified oleocanthal as a natural COX inhibitor with anti-inflammatory activity similar to ibuprofen.)
- Martínez-González MA et al. "Virgin olive oil supplementation and long-term cognition: the PREDIMED-NAVARRA randomized trial" Journal of Nutrition, Health and Aging, 2013. (Mediterranean diet with EVOO maintained cognitive function over 6.5 years in 522 elderly participants.)
- Abuznait AH et al. "Olive-oil-derived oleocanthal enhances beta-amyloid clearance as a potential neuroprotective mechanism against Alzheimer's disease" ACS Chemical Neuroscience, 2013. (Oleocanthal enhanced amyloid-beta clearance across the blood-brain barrier by upregulating P-glycoprotein and LRP1.)
- Almanza-Aguilera E et al. "Consumption of Olive Oil and Diet Quality and Risk of Dementia-Related Death" JAMA Network Open, 2024. (Consuming more than 7 g/day of olive oil was associated with a 28% lower risk of dementia-related death.)
- Sánchez-Quesada C et al. "Association of the Mediterranean dietary pattern with the incidence of depression: the SUN cohort" Archives of General Psychiatry, 2009. (Mediterranean diet adherence, rich in olive oil, was associated with significantly lower depression risk in over 10,000 Spanish graduates.)
- Psaltopoulou T et al. "Olive oil intake and cancer risk: A systematic review and meta-analysis" PLoS ONE, 2022. (Meta-analysis of 45 studies: highest olive oil consumption associated with 31% lower risk of any cancer.)
- LeGendre O et al. "(-)-Oleocanthal rapidly and selectively induces cancer cell death via lysosomal membrane permeabilization" Molecular and Cellular Oncology, 2015. (Oleocanthal killed cancer cells within 30-60 minutes by rupturing lysosomes while leaving healthy cells unharmed.)
- Toledo E et al. "Mediterranean Diet and Invasive Breast Cancer Risk Among Women at High Cardiovascular Risk in the PREDIMED Trial" JAMA Internal Medicine, 2015. (EVOO-supplemented Mediterranean diet reduced breast cancer risk by 68% in the PREDIMED trial.)
- Salas-Salvadó J et al. "Reduction in the incidence of type 2 diabetes with the Mediterranean diet: results of the PREDIMED-Reus nutrition intervention randomized trial" Diabetes Care, 2011. (Mediterranean diet with EVOO reduced new-onset type 2 diabetes by 40% without caloric restriction.)
- Schwingshackl L et al. "Olive oil in the prevention and management of type 2 diabetes mellitus: a systematic review and meta-analysis" Nutrition and Diabetes, 2017. (Meta-analysis of 29 trials: olive oil consumption reduced fasting glucose, insulin, and insulin resistance in type 2 diabetes.)
- Shai I et al. "Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet" New England Journal of Medicine, 2008. (Calorie-unrestricted Mediterranean diet achieved comparable weight loss to calorie-restricted low-fat diet with better cardiovascular markers.)
Research Papers
The following curated PubMed topic searches lead to the peer-reviewed primary literature and systematic reviews that underpin the health claims discussed on this page. Each link opens PubMed in a new tab.
- Olive oil and cardiovascular disease: PREDIMED
- Extra virgin olive oil oleocanthal and inflammation
- Olive oil polyphenols (hydroxytyrosol)
- Olive oil and LDL oxidation (EFSA health claim)
- Olive oil and blood pressure
- Mediterranean diet and all-cause mortality
- Olive oil and type 2 diabetes
- Olive oil and cognitive decline
- Olive oil and breast cancer risk
- Olive oil and endothelial function
Browse all PubMed citations for “Olive Oil”
This content is provided for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider for personalized dietary guidance.
Connections
- Bile Acids: How You Digest Fat — interactive animation
- Cholesterol & the Artery Wall — interactive animation
- Atherosclerosis
- Almonds
- Walnuts
- Avocado
- Salmon
- Tomatoes
- Vitamin E
- Vitamin K
- Cardiovascular Disease
- Alzheimer's Disease
- Cancer
- Diabetes
- Insulin Resistance
- Oxidative Stress
- Glutathione
- Green Tea
- Anti Inflammatory Diet
- Oregano
- Mediterranean Diet — the dietary pattern olive oil anchors, and the framework tested in the PREDIMED trial.