Sjogren's Syndrome
1. Overview
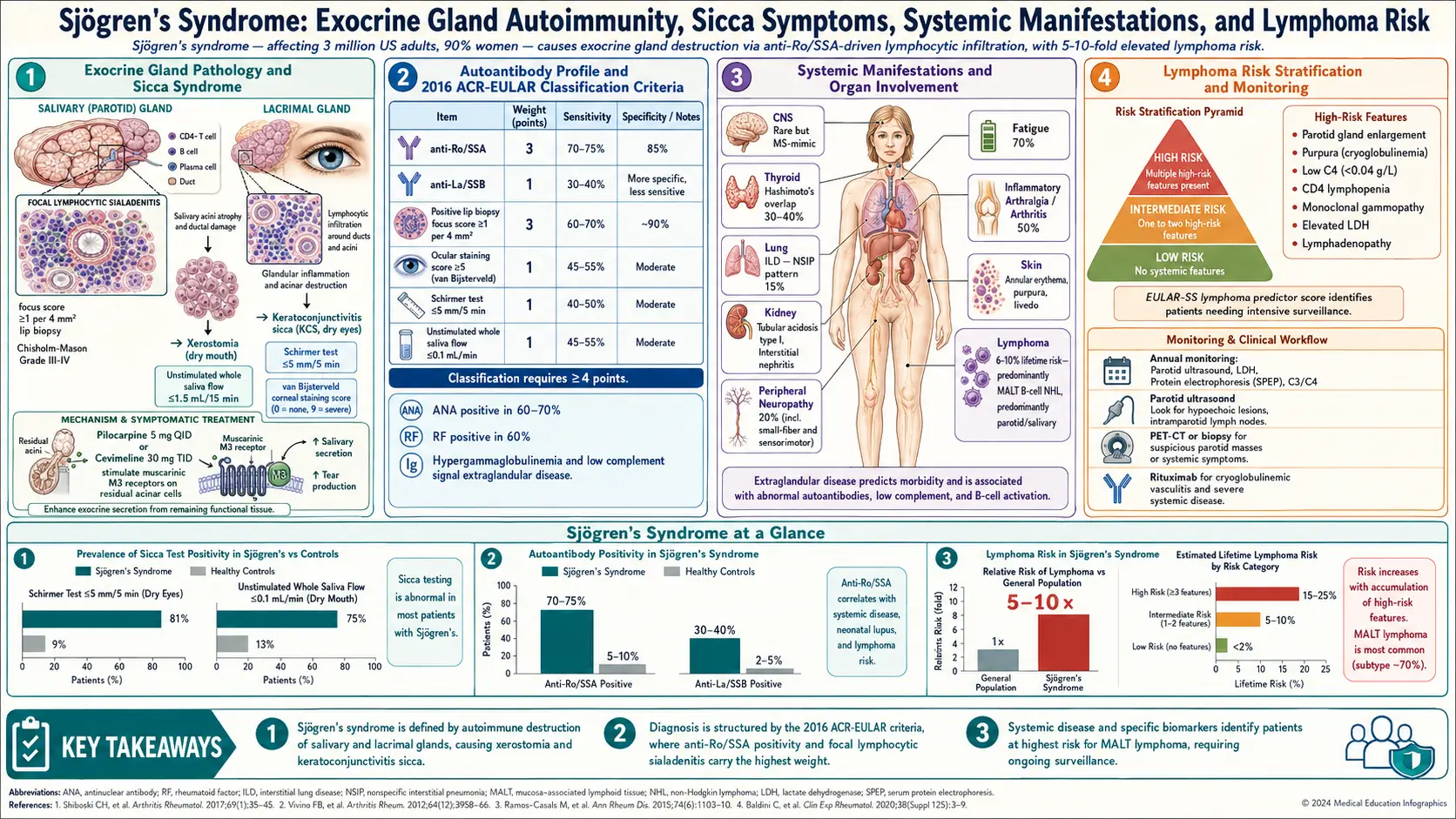
Sjogren's syndrome (SS) is a chronic, systemic autoimmune disease characterized by lymphocytic infiltration and destruction of exocrine glands, predominantly the salivary and lacrimal glands, leading to the hallmark symptoms of dry mouth (xerostomia) and dry eyes (keratoconjunctivitis sicca). This triad of autoimmune-mediated glandular destruction and sicca symptoms defines the disease, though Sjogren's syndrome is far more than a simple "dryness disease" and frequently involves extraglandular organ systems.
Sjogren's syndrome is classified as primary when it occurs independently, or secondary when it develops in association with another autoimmune connective tissue disease, most commonly rheumatoid arthritis, systemic lupus erythematosus (SLE), or systemic sclerosis. Primary Sjogren's syndrome tends to have more prominent extraglandular manifestations and a distinct serological profile, including anti-Ro/SSA and anti-La/SSB antibodies.
A critically important feature of Sjogren's syndrome is its association with an elevated risk of B-cell non-Hodgkin lymphoma (NHL), particularly marginal zone lymphoma (MALT lymphoma) of the parotid gland. This risk is estimated to be 15-20 times greater than in the general population, making lymphoma surveillance a key component of ongoing management. The disease has a significant impact on quality of life, with fatigue, chronic pain, and sicca symptoms contributing to substantial functional impairment.
2. Epidemiology
Sjogren's syndrome is one of the most common systemic autoimmune diseases, with an estimated prevalence of 0.5-1.0% of the general population. It has one of the most striking sex disparities of any autoimmune disease, with a female-to-male ratio of approximately 9:1. The incidence rate is approximately 4-7 per 100,000 person-years. Peak age of onset is between 40 and 60 years, though the disease can occur at any age, including in children and adolescents.
The estimated number of affected individuals in the United States is 1-4 million, making it one of the most prevalent autoimmune diseases after rheumatoid arthritis. However, Sjogren's syndrome remains significantly underdiagnosed, with an average diagnostic delay of 3-7 years from symptom onset. Prevalence is relatively consistent across ethnic groups and geographic regions, though some studies suggest slightly higher rates in Northern European and East Asian populations. Secondary Sjogren's syndrome is found in approximately 20-30% of patients with rheumatoid arthritis, 15-36% of patients with SLE, and 20-25% of patients with systemic sclerosis.
3. Pathophysiology
Glandular Pathology
The hallmark histological finding in Sjogren's syndrome is focal lymphocytic sialadenitis (FLS), the organized infiltration of salivary gland tissue by lymphocytes, predominantly CD4+ T cells in early disease and B cells in established disease. These lymphocytic infiltrates organize into periductal aggregates called foci, quantified as the focus score (number of foci per 4 mm squared of glandular tissue). A focus score of 1 or greater is the histological diagnostic criterion. Progressive glandular infiltration leads to acinar cell destruction, ductal dilation, fibrosis, and ultimately glandular atrophy with loss of secretory function.
Autoantibody Production and B-Cell Hyperactivity
B-cell hyperactivity is a central feature of Sjogren's syndrome pathogenesis. Characteristic autoantibodies include anti-Ro/SSA (present in 60-80% of primary SS) and anti-La/SSB (present in 30-50%). These antibodies target intracellular ribonucleoprotein complexes and may precede clinical disease by years. Additional immunological features include hypergammaglobulinemia (reflecting polyclonal B-cell activation), rheumatoid factor positivity (60-70%), cryoglobulinemia (type II mixed cryoglobulins in 5-20%), and formation of ectopic germinal center-like structures within salivary glands. The chronic B-cell stimulation and germinal center formation create the immunological substrate for lymphomagenesis.
Role of Innate Immunity and Interferons
The type I interferon (IFN) pathway is strongly activated in Sjogren's syndrome. Salivary gland epithelial cells produce type I and type III interferons in response to activation of innate immune sensors, including Toll-like receptors (TLR3, TLR7, TLR9) and cytoplasmic nucleic acid sensors. This "IFN signature" is present in the peripheral blood of approximately 50-80% of primary SS patients and is associated with higher disease activity, more autoantibodies, and greater extraglandular involvement. The epithelial cells themselves are active participants in the autoimmune process, expressing HLA class II molecules and co-stimulatory ligands, effectively acting as non-professional antigen-presenting cells.
The Epithelial Cell as Central Player
The concept of "autoimmune epithelitis" recognizes the central role of epithelial cells in Sjogren's syndrome pathogenesis. Salivary and lacrimal gland epithelial cells are not merely passive targets of autoimmune attack but actively participate in disease perpetuation by expressing inflammatory mediators, presenting autoantigens, producing B-cell activating factors (BAFF/BLyS), and undergoing apoptosis that releases intracellular autoantigens (Ro/SSA, La/SSB) to the cell surface, perpetuating the autoimmune cycle.
4. Etiology and Risk Factors
Genetic Factors
- HLA associations — HLA-DR3 (DRB1*03:01) and HLA-DR2 (DRB1*15:01) are the strongest genetic risk factors; HLA-DR3 is particularly associated with anti-Ro/SSA and anti-La/SSB positivity
- Non-HLA genes — STAT4, IRF5, BLK, TNFAIP3, EBF1, IL12A, and CXCR5 polymorphisms have been identified through genome-wide association studies; many overlap with SLE susceptibility genes
- Familial clustering — first-degree relatives have increased risk of Sjogren's syndrome and other autoimmune diseases
- X chromosome — the extreme female predominance and association with X chromosome abnormalities (47,XXY Klinefelter syndrome is a risk factor) suggest a role for X-linked genes
Environmental Triggers
- Viral infections — Epstein-Barr virus (EBV) is the most studied trigger; EBV DNA and proteins are found in salivary gland epithelial cells of SS patients; other implicated viruses include cytomegalovirus (CMV), hepatitis C virus (HCV), human T-lymphotropic virus type 1 (HTLV-1), and coxsackievirus
- Hepatitis C virus — HCV infection can produce a Sjogren's-like syndrome with sicca symptoms, cryoglobulinemia, and lymphoma risk; must be excluded before diagnosing primary SS
- Hormonal factors — estrogen deficiency (postmenopause) may contribute to disease onset or worsening; androgen deficiency impairs lacrimal gland function
Demographic Risk Factors
- Female sex — approximately 90% of patients are women
- Age — peak onset in the 4th-6th decade of life
- Pre-existing autoimmune disease — patients with RA, SLE, or systemic sclerosis have markedly elevated risk of secondary SS
- History of other autoimmune conditions — autoimmune thyroiditis, primary biliary cholangitis, and celiac disease are frequently comorbid
5. Clinical Presentation
Glandular (Sicca) Manifestations
- Keratoconjunctivitis sicca (dry eyes) — foreign body sensation, burning, grittiness, photosensitivity, blurred vision, eye fatigue; may lead to corneal damage and filamentary keratitis
- Xerostomia (dry mouth) — difficulty swallowing dry foods, need to sip water frequently, altered taste, burning sensation, difficulty speaking for prolonged periods
- Dental complications — accelerated dental caries (especially cervical and incisal edge caries), periodontal disease, oral candidiasis, and difficulty wearing dentures
- Parotid gland enlargement — recurrent or persistent bilateral parotid swelling occurs in approximately 30-50% of patients; unilateral or rapidly progressive enlargement raises concern for lymphoma
- Other exocrine involvement — vaginal dryness, dry skin, nasal dryness and crusting, dry cough, and reduced pancreatic exocrine secretion
Extraglandular Systemic Manifestations
- Fatigue — reported by 70-80% of patients; often the most debilitating symptom; not well correlated with disease activity markers
- Arthralgia and arthritis — non-erosive, symmetric polyarthritis or arthralgias affecting 50-70% of patients; resembles rheumatoid arthritis but typically non-deforming
- Raynaud's phenomenon — occurs in approximately 15-30% of primary SS patients
- Interstitial lung disease — nonspecific interstitial pneumonia (NSIP) and lymphocytic interstitial pneumonia (LIP) are the most common patterns; clinical lung disease in 10-20%
- Renal involvement — tubulointerstitial nephritis (most common), type I distal renal tubular acidosis, and rarely glomerulonephritis; clinically apparent in 5-10%
- Peripheral neuropathy — sensory neuropathy (including small fiber neuropathy), sensorimotor polyneuropathy, and mononeuritis multiplex; affects 10-20% of patients
- Central nervous system involvement — controversial; reported manifestations include cognitive dysfunction, focal deficits, and myelopathy
- Vasculitis — cutaneous vasculitis (palpable purpura) in 5-10%; cryoglobulinemic vasculitis is a marker of lymphoma risk
- Hematological abnormalities — leukopenia, lymphopenia, mild anemia, and thrombocytopenia
Constitutional Symptoms
- Myalgia and widespread pain — fibromyalgia-like symptoms common, with approximately 20-30% of SS patients meeting fibromyalgia criteria
- Low-grade fever — may occur during disease flares
- Depression and cognitive difficulties — high prevalence of mood disorders and subjective cognitive impairment ("brain fog")
6. Diagnosis
2016 ACR/EULAR Classification Criteria
The 2016 ACR/EULAR classification criteria for primary Sjogren's syndrome apply to individuals with at least one symptom of ocular or oral dryness. The criteria use a weighted scoring system (threshold score of 4 or greater):
- Labial salivary gland biopsy with focus score of 1 or greater — 3 points
- Anti-Ro/SSA antibody positive — 3 points
- Ocular staining score of 5 or greater (or van Bijsterveld score of 4 or greater) — 1 point
- Schirmer's test of 5 mm or less per 5 minutes — 1 point
- Unstimulated salivary flow rate of 0.1 mL/min or less — 1 point
These criteria have a sensitivity of 96% and specificity of 95%. Exclusion criteria include prior head and neck radiation, active hepatitis C infection, AIDS, sarcoidosis, amyloidosis, graft-versus-host disease, and IgG4-related disease.
Ocular Assessment
- Schirmer's test — measures tear production; filter paper strip placed in the lower conjunctival fornix for 5 minutes; 5 mm or less of wetting is abnormal
- Ocular surface staining — using lissamine green, rose bengal, or fluorescein to detect conjunctival and corneal epithelial damage
- Tear break-up time — less than 10 seconds indicates tear film instability
- Slit-lamp examination — to assess corneal damage, filamentary keratitis, and other complications
Salivary Gland Assessment
- Labial salivary gland biopsy — the most specific diagnostic test; minor salivary glands obtained from the inner lower lip; focus score of 1 or greater (1 or more foci of 50 or more lymphocytes per 4 mm squared) is diagnostic
- Unstimulated whole salivary flow rate — collection by spitting method over 15 minutes; 0.1 mL/min or less is abnormal
- Parotid sialography — shows characteristic "pruned tree" or "branchless fruit-laden tree" appearance; largely replaced by MRI and ultrasound
- Salivary gland ultrasound — increasingly used; shows hypoechoic areas and inhomogeneous gland structure; scoring systems (OMERACT) being validated
Serological Studies
- Anti-Ro/SSA antibodies — present in 60-80% of primary SS; most important serological marker
- Anti-La/SSB antibodies — present in 30-50%; almost always coexists with anti-Ro/SSA; high specificity for SS
- Antinuclear antibodies (ANA) — positive in 70-90% of primary SS patients
- Rheumatoid factor — positive in 60-70%
- Hypergammaglobulinemia — polyclonal IgG elevation in 50-80%
- Complement levels (C3, C4) — low complement, especially C4, is associated with increased lymphoma risk and extraglandular disease
- Cryoglobulins — type II mixed cryoglobulins in 5-20%; a major risk factor for lymphoma development
- Beta-2 microglobulin — elevated levels associated with lymphoma risk
7. Treatment
Management of Sicca Symptoms
- Artificial tears — preservative-free formulations for frequent use; lipid-containing preparations for evaporative dry eye; gels and ointments for nighttime use
- Topical cyclosporine (Restasis, 0.05%) or lifitegrast (Xiidra, 5%) — anti-inflammatory eye drops that increase tear production; require 4-8 weeks for full effect
- Punctal occlusion — silicone plugs or cautery of lacrimal puncta to reduce tear drainage
- Saliva substitutes and oral moisturizers — carboxymethylcellulose-based products, xylitol-containing lozenges
- Muscarinic agonists — pilocarpine (5 mg three to four times daily) and cevimeline (30 mg three times daily) stimulate residual salivary and lacrimal gland secretion; sweating is the most common side effect
- Dental care — frequent dental examinations, fluoride treatments, antimicrobial rinses, and sugar-free gum to stimulate saliva
Systemic Therapy for Extraglandular Disease
- Hydroxychloroquine — 200-400 mg/day; most commonly used systemic agent; may improve fatigue, arthralgias, and arthritis; requires annual ophthalmologic screening for retinal toxicity
- Methotrexate — 10-25 mg/week for arthritis not responsive to hydroxychloroquine
- Corticosteroids — used for severe extraglandular manifestations (interstitial lung disease, glomerulonephritis, vasculitis, peripheral neuropathy); lowest effective dose for shortest duration
- Azathioprine, mycophenolate mofetil — steroid-sparing immunosuppressants for organ-threatening disease
- Cyclophosphamide — reserved for severe, life-threatening complications such as pulmonary hemorrhage, progressive glomerulonephritis, or severe vasculitis
- Rituximab (anti-CD20) — used off-label for severe extraglandular manifestations, particularly vasculitis, cytopenias, and cryoglobulinemia; evidence from clinical trials has been mixed for overall disease activity but more consistent for specific organ involvement
Lymphoma Surveillance
- Risk stratification — patients with persistent parotid swelling, palpable purpura, low C4, cryoglobulinemia, lymphopenia, and monoclonal gammopathy are at highest risk
- Monitoring — regular clinical assessment, serum protein electrophoresis, complement levels, and complete blood count
- Imaging — PET/CT or contrast-enhanced CT when lymphoma is suspected
- Biopsy — tissue biopsy for definitive diagnosis of any suspicious lymphoproliferative process
8. Complications
- B-cell non-Hodgkin lymphoma — lifetime risk of 5-10% (15-20-fold increased risk); most commonly MALT lymphoma of the parotid gland; also diffuse large B-cell lymphoma; annual incidence approximately 1% per year in high-risk patients
- Corneal ulceration and perforation — from severe, untreated keratoconjunctivitis sicca
- Dental caries and tooth loss — rampant cervical caries from severe xerostomia
- Oral candidiasis — recurrent fungal infections due to reduced salivary antimicrobial factors
- Interstitial lung disease — NSIP, LIP, and organizing pneumonia patterns; may progress to pulmonary fibrosis
- Renal tubular acidosis — type I distal RTA with hypokalemia, nephrocalcinosis, and kidney stones
- Peripheral neuropathy — sensory neuropathy may cause significant pain and functional limitation
- Cryoglobulinemic vasculitis — palpable purpura, arthralgias, glomerulonephritis, and peripheral neuropathy
- Neonatal lupus and congenital heart block — in offspring of mothers with anti-Ro/SSA antibodies (risk approximately 2% for complete heart block)
- Severe fatigue and impaired quality of life — often the most functionally limiting aspect of the disease
9. Prognosis
The overall prognosis of Sjogren's syndrome is generally favorable for the majority of patients, with normal or near-normal life expectancy in those without serious extraglandular complications. However, quality of life is significantly impaired, with sicca symptoms, fatigue, and chronic pain contributing to functional disability comparable to that seen in rheumatoid arthritis and systemic lupus erythematosus.
Patients with extraglandular disease have a less favorable prognosis. The standardized mortality ratio for primary Sjogren's syndrome is approximately 1.3-1.6, primarily driven by lymphoproliferative disease, infections, and cardiovascular complications. The ESSDAI (EULAR Sjogren's Syndrome Disease Activity Index) is the primary tool for assessing systemic disease activity, while the ESSPRI (EULAR Sjogren's Syndrome Patient Reported Index) captures patient-reported symptom burden.
The most significant prognostic concern is the development of B-cell lymphoma. Predictors of lymphoma include persistent parotid enlargement, palpable purpura, low C4 complement levels, type II cryoglobulinemia, lymphopenia, monoclonal gammopathy, and germinal center-like structures on salivary gland biopsy. These features have been incorporated into prognostic scoring systems and guide the intensity of lymphoma surveillance.
10. Prevention
There are no established strategies for preventing the development of Sjogren's syndrome. Management focuses on preventing complications and preserving quality of life:
- Aggressive dental hygiene — regular dental visits every 3-4 months, daily fluoride application, sugar avoidance, xylitol-containing products, and treatment of oral candidiasis to prevent tooth loss
- Ocular surface protection — regular use of artificial tears, avoidance of low-humidity environments, protective eyewear in windy conditions, humidifiers at home and work, and avoidance of medications that worsen dryness (antihistamines, decongestants, tricyclic antidepressants)
- Adequate hydration — frequent small sips of water, keeping water available at all times
- Medication review — many common medications (anticholinergics, antidepressants, antihistamines, diuretics) can exacerbate sicca symptoms
- Lymphoma awareness — patients should be educated about warning signs (persistent gland swelling, unexplained weight loss, night sweats, new lymphadenopathy) and undergo regular monitoring based on risk stratification
- Pregnancy planning — women with anti-Ro/SSA antibodies should be counseled about the risk of neonatal lupus and congenital heart block; fetal heart rate monitoring is recommended from weeks 16-26 of gestation
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Research Papers
- Connections
- Featured Videos
Research Papers
Curated PubMed topic searches on Sjogren's Syndrome. Each link opens a live PubMed query so the result set stays current as new studies are indexed.
- PubMed topic search: Sjogren syndrome review
- PubMed topic search: Primary Sjogren classification criteria
- PubMed topic search: Anti-Ro SSA SSB Sjogren
- PubMed topic search: Sjogren lip biopsy
- PubMed topic search: Pilocarpine cevimeline dry mouth
- PubMed topic search: Hydroxychloroquine Sjogren
- PubMed topic search: Sjogren lymphoma risk
- PubMed topic search: Sjogren pulmonary involvement
- PubMed topic search: Sjogren neurological manifestations
- PubMed topic search: Rituximab Sjogren trial
- PubMed topic search: Schirmer test dry eye
- PubMed topic search: ESSDAI Sjogren activity
Connections
- Lupus
- Arthritis
- Raynaud's Disease
- Lupus-Sjogren's Overlap
- ANA, dsDNA and Lupus Autoantibodies
- Hydroxychloroquine and Antimalarials
- Ankylosing Spondylitis
- Myasthenia Gravis
- Magnesium
- Vitamin D3
- Turmeric
- Low Dose Naltrexone
- Lymphoma
- Peripheral Neuropathy
- Glomerulonephritis
- Fatigue
- Interstitial Lung Disease
- Lupus Nephritis and Kidney Involvement
- Rheumatoid Arthritis
- Dry Eye Disease