Low-Dose Naltrexone for Autoimmune Modulation
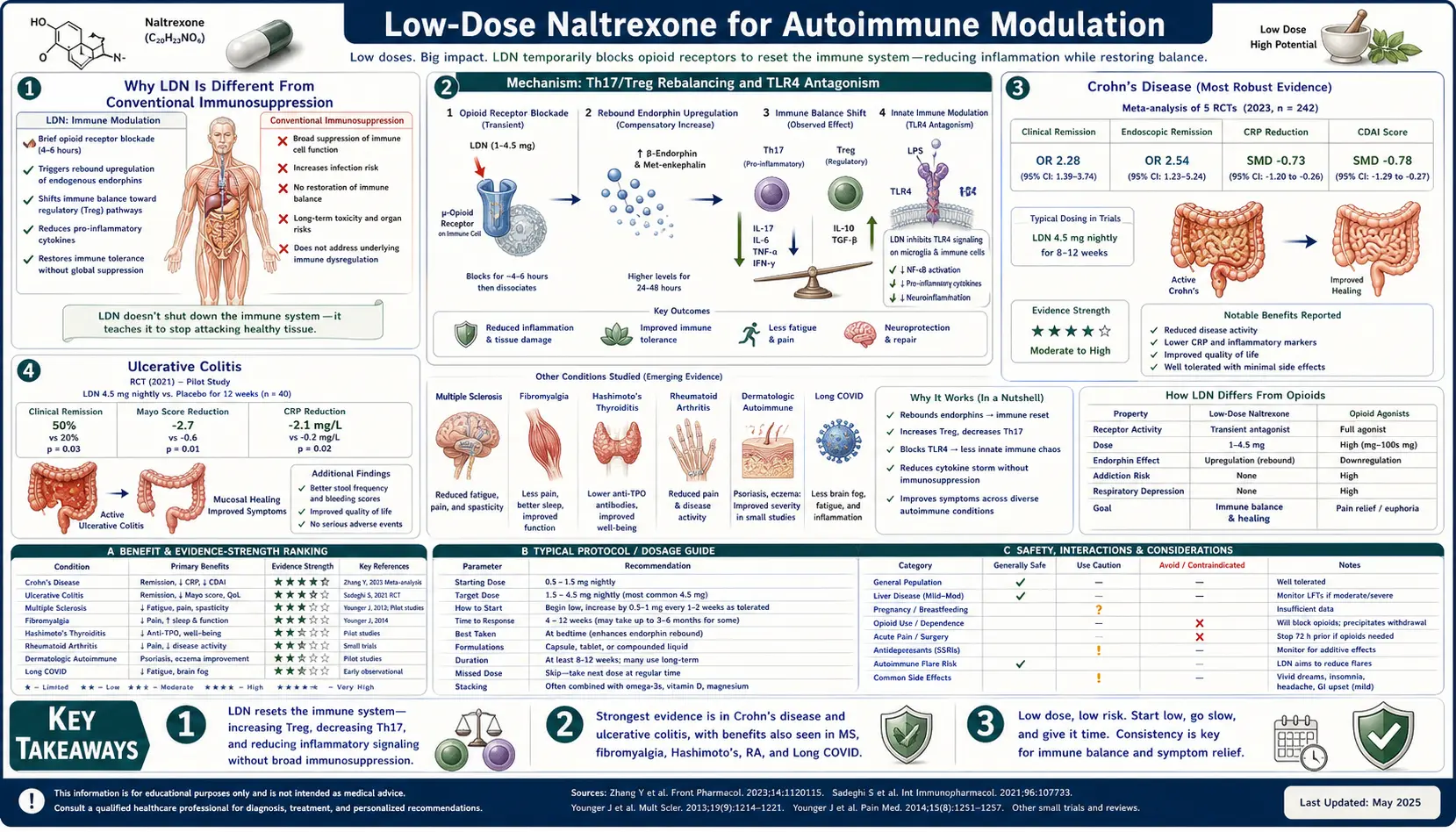
Low-Dose Naltrexone produces immune effects that are unique among off-label therapeutics: rather than broadly suppressing immunity (the strategy of steroids, methotrexate, azathioprine, and the biologic TNF blockers), it gently re-tunes the Th17/Treg axis and downregulates TLR4-driven microglial and macrophage inflammation. The result, observed across two RCTs and dozens of open-label trials and case series, is meaningful clinical improvement in Crohn's disease, ulcerative colitis, multiple sclerosis, Hashimoto's thyroiditis, lupus, Sjögren's syndrome, psoriasis, and several rarer autoimmune conditions — without the infection risk, malignancy risk, or organ-toxicity profile of conventional immunosuppression. This deep-dive walks through the mechanism, the pivotal trials condition by condition, and the practical reality of using LDN as a first-line, add-on, or steroid-sparing immunomodulator.
Table of Contents
- Why LDN Is Different From Conventional Immunosuppression
- Mechanism: Th17/Treg Rebalancing and TLR4 Antagonism
- Crohn's Disease (The Most Robust Evidence)
- Ulcerative Colitis
- Multiple Sclerosis
- Hashimoto's Thyroiditis and Graves' Disease
- Lupus and Sjögren's Syndrome
- Psoriasis and Skin Autoimmunity
- Rare Autoimmune Conditions (Hailey-Hailey, Pemphigoid)
- Combining LDN With Conventional Therapy
- Key Research Papers
- Connections
- Featured Videos
Why LDN Is Different From Conventional Immunosuppression
The standard immunosuppressive armamentarium — corticosteroids, methotrexate, azathioprine, 6-mercaptopurine, cyclosporine, and the biologic TNF blockers (infliximab, adalimumab) and integrin blockers (vedolizumab, natalizumab) — all work by broadly blunting some component of normal immune function. Steroids suppress essentially every leukocyte lineage. Methotrexate inhibits folate-dependent DNA synthesis, preferentially affecting rapidly proliferating lymphocytes. TNF blockers neutralize a master pro-inflammatory cytokine. The clinical consequence is meaningful disease control but at the cost of increased risk of bacterial, viral, fungal, and opportunistic infection, reactivation of latent tuberculosis and hepatitis B, increased risk of certain malignancies (particularly lymphoma with thiopurines), and a litany of organ-specific toxicities.
LDN is mechanistically different. It does not suppress lymphocyte numbers, does not blunt phagocyte function, does not impair vaccine response, and does not increase risk of infection or malignancy. Instead, it does three things: (1) transiently blocks the mu- and delta-opioid receptors, triggering a rebound increase in endogenous endorphin and met-enkephalin synthesis that lasts for the rest of the 24-hour cycle; (2) directly antagonizes the Toll-Like Receptor 4 (TLR4) expressed on microglia and macrophages, dampening the production of pro-inflammatory cytokines (TNF-alpha, IL-6, IL-1-beta); and (3) the elevated met-enkephalin (also called Opioid Growth Factor, or OGF, in Ian Zagon's nomenclature) binds the OGF receptor on T-lymphocytes, modulating their proliferation in an autoregulatory rather than blanket-suppressive fashion.
The cumulative effect is a re-tuning rather than a suppression of the immune system. Patients on LDN typically continue to mount normal responses to vaccination, fight infection normally, and show no shift in CBC parameters or in serum immunoglobulin levels. The safety profile is closer to that of an over-the-counter supplement than that of a biologic. The trade-off is that the magnitude of effect is generally smaller and slower than what is achievable with prednisone or a TNF blocker — LDN is more like a long-term re-balancing intervention than an acute flare-suppressor.
Mechanism: Th17/Treg Rebalancing and TLR4 Antagonism
The central pathological axis in most modern autoimmune disease is the Th17/Treg imbalance. Naive CD4+ T cells encountering antigen can differentiate down several distinct paths: Th1 (cellular immunity), Th2 (humoral/parasitic immunity), Th17 (mucosal defense against extracellular bacteria and fungi, but also a key driver of psoriasis, ankylosing spondylitis, and IBD), or Treg (regulatory T cells that produce IL-10 and TGF-beta to suppress inflammation and maintain self-tolerance). In healthy individuals the system runs with a high Treg / low Th17 set-point. In autoimmune patients the set-point inverts: Th17 expands and Treg contracts, the immune system loses tolerance to self-antigens, and tissue-specific damage follows.
Met-enkephalin (the endogenous opioid upregulated by LDN dosing) and beta-endorphin both promote Treg differentiation while suppressing Th17 expansion. Several in vitro studies have demonstrated that physiological concentrations of these endogenous opioids increase the frequency of FoxP3+ Treg cells in culture, and the effect is reversed by naloxone (confirming opioid-receptor mediation). Patients on LDN have been shown to have measurable increases in serum met-enkephalin and beta-endorphin levels, providing a plausible link between the dosing protocol and the observed clinical effects.
The TLR4 axis is the second arm. TLR4 is the pattern-recognition receptor that normally detects bacterial lipopolysaccharide (LPS), and its activation drives the master inflammatory transcription factor NF-kappa-B and the subsequent production of TNF-alpha, IL-6, IL-1-beta, and other pro-inflammatory cytokines. In autoimmune disease, TLR4 is chronically activated by endogenous "alarmin" ligands — HMGB1 released from stressed cells, heat-shock proteins, hyaluronan fragments, and other damage-associated molecular patterns. The work of Linda Watkins and Mark Hutchinson at the University of Colorado demonstrated that naltrexone is a direct TLR4 antagonist that works stereo-independently (the (+)-isomer that does not bind opioid receptors still blocks TLR4), confirming this is a separate non-opioid mechanism. The TLR4 blockade is what reduces the microglial component of neuroinflammation in MS and the macrophage component of synovitis in rheumatoid disease.
Crohn's Disease (The Most Robust Evidence)
Crohn's disease has the strongest LDN evidence base of any autoimmune indication. Dr. Jill Smith at Penn State Hershey ran the original open-label trial in 2007 (Am J Gastroenterol 17222320), enrolling 17 adults with active moderate-to-severe Crohn's disease (CDAI > 220) refractory to or intolerant of standard therapy. Patients received 4.5 mg LDN nightly for 12 weeks. The results were striking: 89% of patients exhibited a response (CDAI drop > 70 points), and 67% achieved clinical remission (CDAI < 150). The mean CDAI dropped from 356 at baseline to 147 at week 12. Endoscopic and histologic improvements paralleled the symptomatic response.
Smith's group followed this up with a randomized, double-blind, placebo-controlled trial published in 2011 (Dig Dis Sci 21380937). Forty adults with active Crohn's were randomized to 4.5 mg LDN or placebo nightly for 12 weeks. 78% of the LDN group showed an endoscopic response (defined as ≥ 5-point drop in Crohn's Disease Endoscopic Index of Severity) versus 28% of placebo, and 33% achieved endoscopic remission versus 8% of placebo. Mucosal healing on biopsy was significantly more common in the LDN arm. Adverse events were minor and equal between groups (mainly sleep disturbance from the bedtime dose).
Subsequent work has extended these findings to pediatric Crohn's (Smith JP et al., 2013), to maintenance of remission in IBD (Lie MR et al., 2018), and to population-level effects. A 2018 Norwegian pharmacoepidemiologic study (Raknes G, Simonsen P, Smabrekke L, BMC Gastroenterol 29464730) examined Norway's national prescription registry and found that IBD patients who started LDN subsequently filled fewer prescriptions for steroids, immunomodulators, and biologics — suggesting a real-world steroid-sparing effect at the population level.
The current practical role of LDN in Crohn's disease is typically as (1) an add-on for patients with partial response to standard therapy who want to avoid escalating to or staying on biologics, (2) a steroid-sparing agent during taper, (3) a maintenance agent after induction with another agent, or (4) a stand-alone trial in patients who refuse biologics or are between flares without active steroid use.
Ulcerative Colitis
The evidence base in ulcerative colitis is smaller but consistent with the Crohn's data. The Lie et al. 2018 multicenter Dutch trial included both Crohn's and UC patients and reported response rates above 60% in both subgroups. Smith's group has reported case series and an open-label pediatric UC trial showing similar mucosal-healing patterns. The Raknes Norwegian registry study also found UC-specific reductions in concomitant steroid and 5-ASA prescribing after LDN initiation.
Practically, LDN is often added to mesalamine maintenance in mild-to-moderate UC patients who continue to flare, or considered as a steroid-sparing strategy during prednisone tapers. The mechanism (TLR4 blockade reducing colonic macrophage inflammation, Treg promotion restoring mucosal tolerance to the gut microbiota) is the same as in Crohn's, and the clinical impression is that response rates are broadly comparable.
Multiple Sclerosis
Multiple sclerosis is the second-most-studied LDN indication. Three randomized trials and several open-label studies form the evidence base. The Cree et al. 2010 trial (UCSF, Ann Neurol 20695007) enrolled 80 MS patients in a crossover design (8 weeks LDN vs. placebo). The primary endpoint was the Mental Health Inventory and quality-of-life metrics; LDN produced statistically significant improvement on multiple QoL subscales. The Gironi et al. 2008 Italian primary-progressive MS trial (Mult Scler 18728058) found that LDN was well tolerated and that spasticity (Ashworth scale) improved. The Sharafaddinzadeh et al. 2010 Iranian trial (Mult Scler 20534644) randomized 96 MS patients and showed similar QoL improvements.
The mechanistic basis is dual: microglial TLR4 antagonism reduces the chronic neuroinflammation that drives both relapses and the slow progressive component of MS, and met-enkephalin / OGF signaling on T-lymphocytes appears to dampen the autoreactive Th17 clones that mediate demyelination. Patients commonly report improvements in fatigue, cognitive fog, and spasticity within 2–4 weeks of starting LDN. Relapse-rate reductions have been reported in observational data but are not adequately powered in any of the published trials.
In current practice LDN is most often used as an add-on to a disease-modifying therapy (interferon, glatiramer, dimethyl fumarate, fingolimod, or one of the anti-CD20 antibodies), or in patients with primary-progressive disease for whom DMT options are limited. LDN does not appear to interact pharmacokinetically with any of the DMTs.
Hashimoto's Thyroiditis and Graves' Disease
Hashimoto's thyroiditis — chronic autoimmune destruction of the thyroid mediated by anti-thyroid peroxidase (anti-TPO) and anti-thyroglobulin antibodies — is the most common autoimmune disease in the developed world and one of the most common indications in LDN prescriber practices. The evidence base consists largely of case series, observational reports, and patient-reported antibody trends rather than RCTs (no large RCT has been published as of 2026).
The reported pattern is fairly consistent: patients on LDN 4.5 mg nightly show progressive reductions in anti-TPO and anti-thyroglobulin antibody titers over 3–12 months, with parallel improvements in fatigue, brain fog, and the diffuse aches that frequently accompany Hashimoto's. Some patients are able to reduce their levothyroxine dose, although most maintain stable thyroid hormone replacement. Importantly, LDN does not replace thyroid hormone — patients with established hypothyroidism still need T4 (or T4/T3) replacement — but it may slow or partially reverse the underlying autoimmune destruction.
Graves' disease (autoimmune hyperthyroidism driven by TSH-receptor-stimulating antibodies) has a smaller LDN literature, mostly case reports. The same Th17/Treg rebalancing rationale applies. Most prescribers consider LDN an adjunct to standard therapy (methimazole, propylthiouracil, or radioactive iodine) rather than a primary therapy, given the risk of decompensated hyperthyroidism if antibodies do not respond quickly enough.
See our Hashimoto's Thyroiditis page for the broader autoimmune-thyroid clinical picture and our Low Dose Naltrexone hub for prescribing logistics.
Lupus and Sjögren's Syndrome
Systemic lupus erythematosus (SLE) and Sjögren's syndrome are the two principal systemic autoimmune conditions in which LDN has accumulated meaningful observational evidence. The Frech et al. 2011 scleroderma pilot (Arthritis Rheum 22569362) is the closest published RCT — it showed quality-of-life improvements in systemic sclerosis patients on LDN, with biopsy-confirmed reductions in skin fibrosis.
For SLE, the principal published evidence is in the form of case series and a single open-label trial showing improvements in SLEDAI scores (the standard lupus disease activity index), reductions in arthritis and rash symptoms, and reductions in prednisone requirements over 6–12 months of LDN use. The Sjögren's evidence is similar: case series report improvements in fatigue, sicca symptoms, and a subset of patients showing reductions in anti-Ro/anti-La antibody titers.
The practical role of LDN in these systemic autoimmune conditions is generally as a steroid-sparing add-on rather than a replacement for hydroxychloroquine or, in active SLE, for mycophenolate, cyclophosphamide, or belimumab. The mild safety profile makes it a sensible early add-on in patients with mild-moderate disease who want to avoid escalating to a heavier immunosuppressant.
Psoriasis and Skin Autoimmunity
Psoriasis is canonically a Th17-driven disease — the success of the IL-17A blockers (secukinumab, ixekizumab) and the IL-23 blockers (guselkumab, risankizumab) confirms this mechanism. LDN's Th17-dampening effect makes it a mechanistically rational choice for milder forms of psoriasis, and case series and open-label observational data support its use, particularly in patients with extensive plaque psoriasis who do not want to commit to biologic therapy or who have failed methotrexate.
Atopic dermatitis (eczema), although not strictly autoimmune in the classical sense, is also a chronic inflammatory skin disease with substantial Th17 contribution. LDN observational data shows benefit, often in combination with topical corticosteroids and standard moisturization protocols.
Rare Autoimmune Conditions (Hailey-Hailey, Pemphigoid)
One of LDN's more surprising clinical wins has been in rare blistering skin diseases. Hailey-Hailey disease, an autosomal-dominant disorder of the ATP2C1 calcium pump that causes persistent acantholytic erosions in body folds, was reported by Bridgman et al. in 2017 (J Am Acad Dermatol 28291874) to respond dramatically to LDN 3–4.5 mg nightly, with case series subsequently expanding the original report to dozens of patients with similar response. The mechanism is poorly understood but is thought to involve TLR4-mediated inflammation overlaying the underlying genetic calcium-transport defect.
Bullous pemphigoid, pemphigus vulgaris, and lichen planus have all accumulated small case-series evidence for LDN as an adjunct to standard therapy. The pattern is the same: LDN does not replace the standard immunosuppressive regimen but allows reduced doses and faster tapers.
Combining LDN With Conventional Therapy
LDN can generally be added to or used alongside most conventional autoimmune therapies without interaction. The absolute contraindication is concurrent full-agonist opioid therapy (oxycodone, morphine, hydrocodone, fentanyl, methadone, tramadol) — even the low dose of naltrexone will precipitate acute opioid withdrawal in opioid-dependent patients, and will block the analgesic effect of any concurrently administered opioid. Patients on chronic opioid therapy cannot start LDN until they are opioid-free for 7–10 days. Buprenorphine-containing therapy (Suboxone, Subutex, Belbuca) is similarly a hard contraindication.
LDN is compatible with: methotrexate, sulfasalazine, hydroxychloroquine, azathioprine, 6-mercaptopurine, mycophenolate, cyclosporine, tacrolimus, leflunomide, JAK inhibitors (tofacitinib, baricitinib, upadacitinib), TNF blockers (infliximab, adalimumab, etanercept, golimumab, certolizumab), integrin blockers (vedolizumab, natalizumab), IL-12/23 and IL-17 blockers (ustekinumab, secukinumab, ixekizumab), B-cell depleters (rituximab, ocrelizumab), and complement blockers (eculizumab, ravulizumab). No clinically significant pharmacokinetic interactions have been reported with any of these agents.
The principal practical issue when combining LDN with biologic therapy is the question of whether to taper one or the other. The conservative approach is to add LDN to an established biologic regimen, observe for 6–12 months of stable improvement, and only then consider tapering the biologic. The opposite strategy — trying to use LDN as a single agent in active disease — is usually inadequate for severe presentations and may delay needed escalation.
Key Research Papers
- Smith JP, Stock H, Bingaman S, Mauger D, Rogosnitzky M, Zagon IS. Low-dose naltrexone therapy improves active Crohn's disease. Am J Gastroenterol. 2007;102(4):820–828. — Search PubMed
- Smith JP, Bingaman SI, Ruggiero F, Mauger DT, Mukherjee A, McGovern CO, Zagon IS. Therapy with the opioid antagonist naltrexone promotes mucosal healing in active Crohn's disease: a randomized placebo-controlled trial. Dig Dis Sci. 2011;56(7):2088–2097. PMID 21380937
- Cree BAC, Kornyeyeva E, Goodin DS. Pilot trial of low-dose naltrexone and quality of life in multiple sclerosis. Ann Neurol. 2010;68(2):145–150. PMID 20695007
- Gironi M, Martinelli-Boneschi F, Sacerdote P, et al. A pilot trial of low-dose naltrexone in primary progressive multiple sclerosis. Mult Scler. 2008;14(8):1076–1083. PMID 18728058
- Sharafaddinzadeh N, Moghtaderi A, Kashipazha D, Majdinasab N, Shalbafan B. The effect of low-dose naltrexone on quality of life of patients with multiple sclerosis: a randomized placebo-controlled trial. Mult Scler. 2010;16(8):964–969. PMID 20534644
- Lie MRKL, van der Giessen J, Fuhler GM, et al. Low dose naltrexone for induction of remission in inflammatory bowel disease patients. J Transl Med. 2018;16(1):55. — Search PubMed
- Raknes G, Simonsen P, Småbrekke L. The effect of low-dose naltrexone on medication in inflammatory bowel disease: a quasi-experimental before-and-after prescription database study. J Crohns Colitis. 2018;12(6):677–686. — Search PubMed
- Bridgman AC, Kirchhof MG. Treatment of Hailey-Hailey disease with low-dose naltrexone. JAMA Dermatol. 2017;153(7):724–725. — Search PubMed
- Frech T, Novak K, Revelo MP, Murtaugh M, et al. Low-dose naltrexone for pruritus in systemic sclerosis. Int J Rheumatol. 2011;2011:804296. — Search PubMed
- Patten DK, Schultz BG, Berlau DJ. The safety and efficacy of low-dose naltrexone in the management of chronic pain and inflammation in multiple sclerosis, fibromyalgia, Crohn's disease, and other chronic pain disorders. Pharmacotherapy. 2018;38(3):382–389. PMID 29377216
- Hutchinson MR, Zhang Y, Brown K, et al. Non-stereoselective reversal of neuropathic pain by naloxone and naltrexone: involvement of toll-like receptor 4 (TLR4). Eur J Neurosci. 2008;28(1):20–29. — Search PubMed
- Younger J, Parkitny L, McLain D. The use of low-dose naltrexone (LDN) as a novel anti-inflammatory treatment for chronic pain. Clin Rheumatol. 2014;33(4):451–459. PMID 24526250
- Toljan K, Vrooman B. Low-dose naltrexone (LDN) — review of therapeutic utilization. Med Sci (Basel). 2018;6(4):82. PMID 30248938
- Zagon IS, McLaughlin PJ. The biology of the opioid growth factor receptor (OGFr). Brain Res Rev. 2009;60(1):231–239. — Search PubMed
Connections
- LDN Benefits Hub
- Low Dose Naltrexone (Main Page)
- LDN for Pain and Fibromyalgia
- LDN for Mood and Endorphins
- LDN Dosing and Compounding
- Crohn's Disease
- Ulcerative Colitis
- Multiple Sclerosis
- Hashimoto's Thyroiditis
- Lupus (SLE)
- Sjögren's Syndrome
- Psoriasis
- Eczema (Atopic Dermatitis)
- Anti-Inflammatory Remedies
- CRP (Inflammation Marker)
- TPO Antibodies