Low-Dose Naltrexone Dosing and Compounding Pharmacies
Low-Dose Naltrexone is one of the very few prescription medications in routine use that cannot be filled at a standard retail pharmacy. Commercial naltrexone is manufactured only as a 50 mg tablet (Revia) or a 380 mg monthly intramuscular depot (Vivitrol), both indicated and dosed for opioid and alcohol use disorder. The low-dose use requires custom compounding from bulk naltrexone hydrochloride into 0.5–4.5 mg capsules, liquid suspension, or sublingual troches — a process that only compounding pharmacies are equipped to perform. This deep-dive walks through the standard titration protocol, the various formulation options, the cost and insurance landscape, the practical logistics of ordering and refilling from a compounding pharmacy, the absolute and relative contraindications, and the common side effects and their management.
Table of Contents
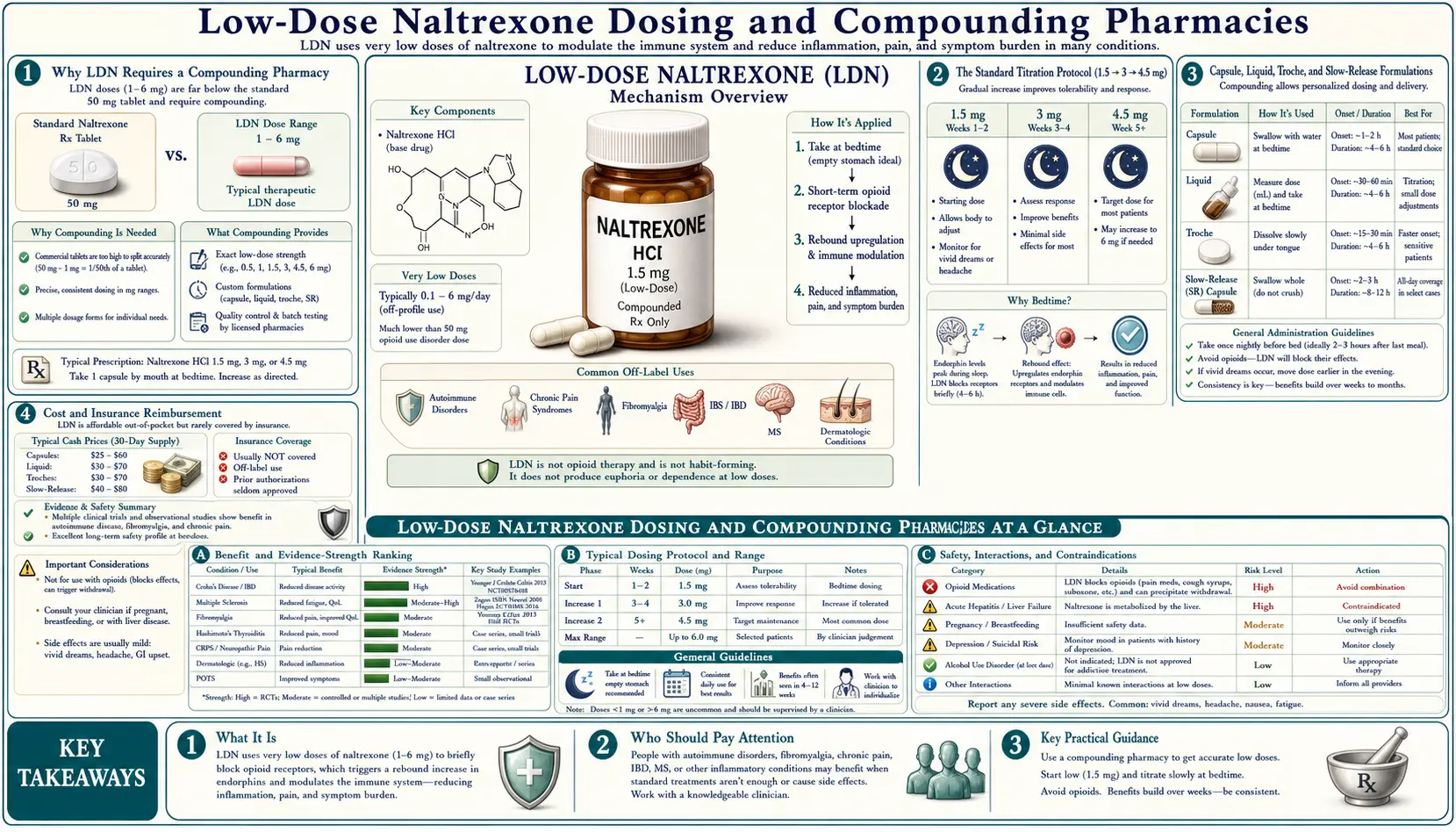
- Why LDN Requires a Compounding Pharmacy
- The Standard Titration Protocol (1.5 → 3 → 4.5 mg)
- Capsule, Liquid, Troche, and Slow-Release Formulations
- Cost and Insurance Reimbursement
- Finding a Compounding Pharmacy and a Willing Prescriber
- Common Side Effects and Their Management
- Absolute Contraindications
- Relative Cautions and Drug Interactions
- Treatment Duration and Monitoring
- Discontinuation and Tapering
- Key Research Papers
- Connections
- Featured Videos
Why LDN Requires a Compounding Pharmacy
Naltrexone was originally developed by Endo Laboratories in the 1960s and approved by the FDA in 1984 for the treatment of opioid use disorder, with the alcohol use disorder indication added in 1995. The standard commercial product (originally branded ReVia, now generic) is a 50 mg tablet intended for once-daily dosing in opioid- or alcohol-dependent patients. The depot intramuscular formulation (Vivitrol) provides 380 mg of naltrexone released over approximately one month. Neither product is manufactured in the 0.5–4.5 mg dose range used for low-dose indications.
The patent on naltrexone expired in 2003, which removed any commercial incentive for a pharmaceutical company to develop, test, and market a low-dose formulation. The new indication (off-label autoimmune, pain, mood) cannot be repatented for the original molecule, and the new-drug-application costs of formal indication-extension would be unrecoverable. The economic structure of the pharmaceutical industry essentially guarantees that a 1.5–4.5 mg naltrexone tablet will never be commercially manufactured.
This leaves three practical options for patients: (1) splitting a 50 mg tablet into approximately 1/11 to 1/33 fractions (impractical and inaccurate), (2) compounding from bulk naltrexone hydrochloride powder into custom 0.5–4.5 mg capsules or liquid (the standard solution), or (3) the relatively new "do-it-yourself" liquid LDN technique of dissolving a 50 mg tablet in 50 mL of water to create a 1 mg/mL liquid (which works but introduces measurement and stability concerns and is not how prescribers typically dispense).
The standard compounding approach uses bulk naltrexone hydrochloride USP (United States Pharmacopeia grade) as the active ingredient. The compounding pharmacist measures the bulk powder, mixes it with appropriate fillers (typically microcrystalline cellulose, lactose-free options available for sensitive patients), and encapsulates into gelatin or vegetable capsules at the prescribed dose. Liquid formulations use water or a flavored vehicle as the carrier. Sublingual troches use a polyethylene glycol or gelatin base. Slow-release formulations require a sustained-release matrix that not all compounding pharmacies stock.
The Standard Titration Protocol (1.5 → 3 → 4.5 mg)
The standard LDN titration is:
- 1.5 mg at bedtime × 2–4 weeks — allows the patient to adapt to the brief receptor blockade, identify any sleep disturbance or vivid-dreams sensitivity, and establish that the medication is tolerated.
- 3 mg at bedtime × 2–4 weeks — intermediate dose; some patients stabilize at this dose and do not need further escalation. Particularly relevant for smaller patients, sensitive patients, or patients with persistent sleep disturbance.
- 4.5 mg at bedtime as maintenance dose — the dose used in the Crohn's and fibromyalgia RCTs and most published trials. This is the maintenance dose for most adult patients with autoimmune, pain, or mood indications.
Some practitioners titrate faster (1.5 mg × 1 week, 3 mg × 1 week, then 4.5 mg) and some slower (1.5 mg × 4–6 weeks before escalating). Faster titration is appropriate in patients who are tolerating the medication well and want to reach the target dose quickly. Slower titration is appropriate in patients who are particularly sensitive or who develop side effects that take time to adapt.
A subset of patients do better at doses lower than 4.5 mg. The most common observation is that some patients respond optimally at 3 mg, with no additional benefit and increased side effects at 4.5 mg. A minority do better at 1.5 mg or even at 0.5–1 mg (ultra-low-dose naltrexone, ULDN). The general principle is to find the minimum effective dose for the individual patient, which may require some experimentation.
A small group of patients reportedly do better at higher doses (6–9 mg). These doses are still well below the opioid-blocking dose (which is 50 mg+ for clinical opioid antagonism) but are above the standard LDN range. The evidence for high-dose LDN is limited and the safety profile is less well-characterized; most prescribers reserve doses above 4.5 mg for patients who have clearly tolerated the standard dose but had inadequate clinical response.
Capsule, Liquid, Troche, and Slow-Release Formulations
The most common formulations are:
- Capsules — the standard formulation. Compounded in fixed doses (1.5 mg, 3 mg, 4.5 mg) as gelatin or vegetable capsules. Stable, easy to dose, easy to ship. Cost is typically $30–$60 per month for a 30-capsule supply. Most compounding pharmacies offer capsules as the default option.
- Liquid suspension — naltrexone HCl dissolved in water or flavored vehicle at 1 mg/mL. Allows for fine titration (e.g., 0.5, 0.75, 1, 1.5 mg) and is easier for patients with swallowing difficulties. Stability is typically 30–60 days refrigerated. Used for pediatric patients and for ultra-low-dose titration.
- Sublingual troches — lozenge-style formulation that dissolves under the tongue. May produce slightly different pharmacokinetics (more first-pass-bypass absorption) but the differences are minor and most clinicians do not differentiate between capsule and troche. Some patients prefer troches for taste/texture reasons.
- Slow-release — compounded with a sustained-release matrix (typically methylcellulose or hydroxypropyl methylcellulose) to extend the absorption profile over 6–12 hours rather than the 30–60 minute peak of immediate-release. May reduce vivid-dreams and acute side effects but the clinical efficacy evidence is more limited. Not all compounding pharmacies offer this option.
- Transdermal cream — an experimental option that some compounding pharmacies offer. Not commonly used; the oral routes are more established.
For new patients, the standard starting formulation is the immediate-release capsule taken at bedtime. Other formulations are reserved for specific situations (sleep disturbance issues, swallowing difficulties, pediatric use, or specific patient preferences).
Cost and Insurance Reimbursement
The cash price for a 30-day supply of LDN capsules is typically $30–$60 USD, depending on the compounding pharmacy, the geographic region, and whether discount codes are used. Some advocacy-focused compounding pharmacies (Skip's in Idaho, Belmar in Colorado, Lee Silsby in Ohio, Olympia in Washington) have developed LDN as a specialty service and often offer competitive pricing for the indication.
Insurance reimbursement for compounded LDN is highly variable. The main barriers are: (1) most US insurance formularies do not cover compounded medications, (2) compounded medications often have to be processed through the insurance company's "compound rider" if one exists, (3) the off-label indication means that even when compounded medications are covered in principle, the specific use may not be, and (4) the relatively low cash price often makes pursuing insurance coverage not worth the administrative effort.
Practical strategies for cost management include: (1) Manufacturer-direct or pharmacy-direct discount programs (some compounding pharmacies offer 90-day supplies at lower per-month pricing), (2) FSA/HSA reimbursement (compounded LDN is generally an eligible expense), (3) GoodRx and similar discount cards which sometimes have coupons for specific compounding pharmacies, (4) Veterans Affairs and Indian Health Service systems where compounded LDN is sometimes available at no cost to eligible patients, (5) The $0.07/day cost of unprocessed naltrexone hydrochloride means the compounding fee dominates — cooperatives and clinics that compound in larger batches can be substantially cheaper.
Some Medicare patients can get LDN covered through Part D depending on the specific plan. Most patients on private insurance pay cash regardless of their coverage tier. The cash price of $30–$60/month is generally manageable for most patients, particularly compared to the cost of biologic therapy ($1,000–$5,000/month) that LDN may help reduce or replace.
Finding a Compounding Pharmacy and a Willing Prescriber
The LDN Research Trust maintains a directory of compounding pharmacies experienced with LDN at ldnresearchtrust.org. The directory is searchable by country, US state, and pharmacy specialty. In the United States, several pharmacies have developed LDN as a specialty service and ship nationally:
- Skip's Pharmacy (Boca Raton, Florida) — long-established LDN-specialist compounding pharmacy
- Belmar Pharmacy (Lakewood, Colorado) — major LDN compounder, ships nationally
- Lee Silsby Compounding Pharmacy (Beachwood, Ohio) — LDN-specialist with a research arm
- Olympia Compounding Pharmacy (Lacey, Washington) — west-coast LDN compounder
- Innovative Compounding Pharmacy (Sacramento, California)
- The Compounder Pharmacy (Aurora, Illinois)
Finding a prescriber willing to write for off-label LDN can be more challenging than finding a compounding pharmacy. Most conventional primary care physicians, rheumatologists, gastroenterologists, and pain specialists have varying levels of familiarity with LDN — some are highly experienced and routinely prescribe it, others are unfamiliar and reluctant. The LDN Research Trust prescriber directory and similar online listings can help patients locate experienced prescribers in their area.
Telemedicine has substantially expanded prescriber access. Several US telemedicine practices specialize in LDN evaluation and prescribing (often with a same-day or next-day initial visit), bridge prescriptions to a chosen compounding pharmacy, and provide follow-up monitoring. The typical cost is $150–$300 for an initial evaluation plus a per-month or per-quarter follow-up fee. For patients whose local providers will not prescribe LDN, telemedicine is often the most practical pathway to therapy.
Common Side Effects and Their Management
The reported side effect profile of LDN is remarkably benign — the safety database now spans over four decades of use and tens of thousands of patient-years, with no signal of organ toxicity, hematologic suppression, infection risk, or carcinogenicity. The common side effects are:
- Vivid dreams (30–50% during first 1–3 weeks, typically resolves) — usually not distressing; some patients find them interesting. If unsettling, can move dose to early evening, split the dose, or try slow-release.
- Sleep disturbance (insomnia, mid-night awakenings; 10–20%, often transient) — same workarounds as vivid dreams. Persistent sleep disturbance is the most common reason for therapy discontinuation.
- Mild headache (5–10%, usually transient) — if persistent, dose reduction or slower titration can help.
- GI upset (mild nausea, occasional diarrhea; 5–10%) — usually transient; taking with food can help.
- Mood lability or irritability (uncommon, <5%) — usually transient; if persistent may indicate the dose is too high for the patient.
- Skin reactions (rash, pruritus; rare) — may reflect sensitivity to a capsule filler rather than to naltrexone itself; trying a different filler (lactose-free, microcrystalline cellulose-free, etc.) can resolve.
Serious adverse events from LDN are uncommon. There is no signal of liver toxicity at low doses (despite a black-box warning on the standard 50 mg dose related to high-dose hepatotoxicity in early studies that has not been replicated). There is no signal of hematologic, renal, or cardiac toxicity. There is no signal of infection or malignancy risk, which is one of the major safety advantages over conventional immunosuppressants.
Absolute Contraindications
The absolute contraindications to LDN are:
- Current use of any full-agonist opioid — oxycodone, hydrocodone, morphine, fentanyl, methadone, tramadol, codeine, oxymorphone, hydromorphone, and any combination products containing these. Even brief exposure to LDN will precipitate acute opioid withdrawal in a dependent patient and block the analgesic effect of any opioid administered concurrently. A 7–10 day complete opioid-free interval is required before starting LDN.
- Current use of buprenorphine (Suboxone, Subutex, Belbuca, Butrans) — partial agonist activity sufficient to be antagonized by LDN. Same 7–10 day washout required.
- Severe acute liver failure — not because LDN is hepatotoxic at this dose, but because the metabolism may be unpredictable in severe hepatic dysfunction. Stable chronic liver disease is not a contraindication.
- Allergy or sensitivity to naltrexone or to the compounding excipients — rare, but if a patient has had a previous severe allergic reaction to naltrexone, LDN is contraindicated.
Pregnancy is a relative rather than absolute contraindication. Most prescribers recommend discontinuation during pregnancy and lactation given limited human safety data, though some continue LDN through pregnancy in patients with active autoimmune disease where the maternal benefit clearly outweighs the unknown fetal risk.
Relative Cautions and Drug Interactions
Beyond the absolute contraindications, several situations warrant caution or modified dosing:
- Anticipated surgery — patients on LDN may have reduced opioid responsiveness in the immediate post-LDN dosing window. Discuss with anesthesia preoperatively. Most LDN patients can hold their dose for 24–48 hours before surgery to ensure opioid responsiveness if needed.
- Acute trauma or injury requiring opioid analgesia — same consideration; LDN may need to be held briefly.
- Kratom use — kratom contains the mu-opioid agonist mitragynine and should be discontinued before LDN (treat as opioid).
- Anti-diarrheal loperamide — loperamide has peripheral mu-opioid activity. At standard antidiarrheal doses this is not a clinically significant interaction with LDN, but at very high loperamide doses (such as those used in opioid-substitution misuse) the interaction would be more relevant.
- Dextromethorphan — has some opioid-like activity but the interaction with LDN is generally not clinically significant at OTC cough-suppressant doses.
LDN does not have clinically significant pharmacokinetic interactions with the major immunosuppressants, biologics, antidepressants, anticonvulsants, antihypertensives, or other commonly co-prescribed medications. The only meaningful drug-drug interactions are with the opioid agonists listed above.
Treatment Duration and Monitoring
LDN is generally a long-term therapy. The clinical effects on autoimmune disease, chronic pain, and mood are sustained as long as the medication is continued and typically diminish over weeks to months after discontinuation. Most patients who respond to LDN remain on it indefinitely or until the underlying condition resolves spontaneously.
Routine monitoring on LDN is minimal. No specific laboratory monitoring is required for LDN itself — there is no signal of liver, kidney, or hematologic toxicity that would justify routine screening. Disease-specific monitoring continues as appropriate for the underlying condition (CRP, ESR, disease-activity indices, organ-specific function tests). Patients on LDN as an adjunct to conventional immunosuppression should continue the standard monitoring for the conventional agent (CBC, LFTs, methotrexate levels, etc.).
The typical clinical follow-up cadence is: initial visit, 4–6 week follow-up to assess tolerance and dose, 12–16 week follow-up to assess clinical response at the target dose, and then 6–12 month follow-up intervals once stable. Many telemedicine LDN practices use a quarterly follow-up model with refill renewals contingent on a brief check-in visit.
If a patient has been on LDN at the target dose for 12–16 weeks with no perceived clinical benefit, the medication is unlikely to produce future benefit and can be discontinued. Some patients have a delayed response (improvement noticed only after 4–6 months); the conservative approach in a partially responding patient is to continue for at least 6 months before concluding the trial has failed.
Discontinuation and Tapering
LDN does not produce physiological dependence, tolerance, or withdrawal. It can be stopped abruptly without medical risk. The clinical effects (improved autoimmune disease control, reduced pain, improved mood) tend to fade over weeks to months as the rebound endogenous opioid upregulation reverts to baseline.
For patients discontinuing LDN, the common patterns are: (1) gradual return of pre-treatment symptoms over 4–12 weeks, (2) flare of underlying autoimmune disease in some patients (often within 1–3 months of discontinuation), and (3) generally easy resumption of LDN if needed, with re-establishment of clinical benefit usually within 2–4 weeks of restart.
A formal taper is not necessary but some practitioners taper from 4.5 mg to 3 mg to 1.5 mg over a few weeks to assess whether a lower dose might still maintain clinical benefit. This can be useful in patients who are stable and exploring dose minimization. There is no medical reason that abrupt discontinuation would be unsafe.
For patients who need to start opioid therapy (acute injury, surgery, or new chronic pain requiring opioid management), LDN should be discontinued at least 24–48 hours before the planned opioid initiation. Restarting LDN requires the standard 7–10 day opioid-free interval.
Key Research Papers
- Verebey K, Volavka J, Mulé SJ, Resnick RB. Naltrexone: disposition, metabolism, and effects after acute and chronic dosing. Clin Pharmacol Ther. 1976;20(3):315–328. — Search PubMed
- Smith JP, Stock H, Bingaman S, Mauger D, Rogosnitzky M, Zagon IS. Low-dose naltrexone therapy improves active Crohn's disease. Am J Gastroenterol. 2007;102(4):820–828. — Search PubMed
- Smith JP, Bingaman SI, Ruggiero F, et al. Therapy with the opioid antagonist naltrexone promotes mucosal healing in active Crohn's disease. Dig Dis Sci. 2011;56(7):2088–2097. PMID 21380937
- Younger J, Noor N, McCue R, Mackey S. Low-dose naltrexone for the treatment of fibromyalgia. Arthritis Rheum. 2013;65(2):529–538. PMID 23359310
- Patten DK, Schultz BG, Berlau DJ. The safety and efficacy of low-dose naltrexone in the management of chronic pain and inflammation. Pharmacotherapy. 2018;38(3):382–389. PMID 29377216
- Toljan K, Vrooman B. Low-dose naltrexone (LDN) — review of therapeutic utilization. Med Sci (Basel). 2018;6(4):82. PMID 30248938
- Younger J, Parkitny L, McLain D. The use of low-dose naltrexone (LDN) as a novel anti-inflammatory treatment for chronic pain. Clin Rheumatol. 2014;33(4):451–459. PMID 24526250
- Trofimovitch D, Baumrucker SJ. Pharmacology update: low-dose naltrexone as a possible non-opioid modality. Am J Hosp Palliat Care. 2019;36(10):907–912. — Search PubMed
- Brown N, Panksepp J. Low-dose naltrexone for disease prevention and quality of life. Med Hypotheses. 2009;72(3):333–337. — Search PubMed
- Lie MRKL, van der Giessen J, Fuhler GM, et al. Low dose naltrexone for induction of remission in inflammatory bowel disease patients. J Transl Med. 2018;16(1):55. — Search PubMed
- Raknes G, Småbrekke L. The effect of low-dose naltrexone on medication in inflammatory bowel disease: a quasi-experimental before-and-after prescription database study. J Crohns Colitis. 2018;12(6):677–686. — Search PubMed
- Bihari B. Bernard Bihari, MD: low-dose naltrexone for normalizing immune system function. Altern Ther Health Med. 2013;19(2):56–65. — Search PubMed
- Krupitsky EM, Zvartau E, Blokhina E, et al. Naltrexone with or without guanfacine for preventing relapse to opiate addiction in St. Petersburg, Russia. Drug Alcohol Depend. 2013;132(3):674–680. — Search PubMed
- Hatfield E, Phillips K, Swidan S, Ashman L. Use of low-dose naltrexone in the management of chronic pain conditions: a systematic review. J Am Dent Assoc. 2020;151(11):891–902. — Search PubMed
Connections
- LDN Benefits Hub
- Low Dose Naltrexone (Main Page)
- LDN for Autoimmune Modulation
- LDN for Pain and Fibromyalgia
- LDN for Mood and Endorphins
- All Remedies
- Crohn's Disease
- Fibromyalgia
- Multiple Sclerosis
- Hashimoto's Thyroiditis
- Lupus (SLE)
- ME/CFS
- Complex Regional Pain Syndrome
- Anti-Inflammatory Remedies
- CRP (Inflammation Marker)
- ANA (Autoimmune Screening)