Menopause and Hormone Replacement Therapy (HRT): The Modern Reassessment
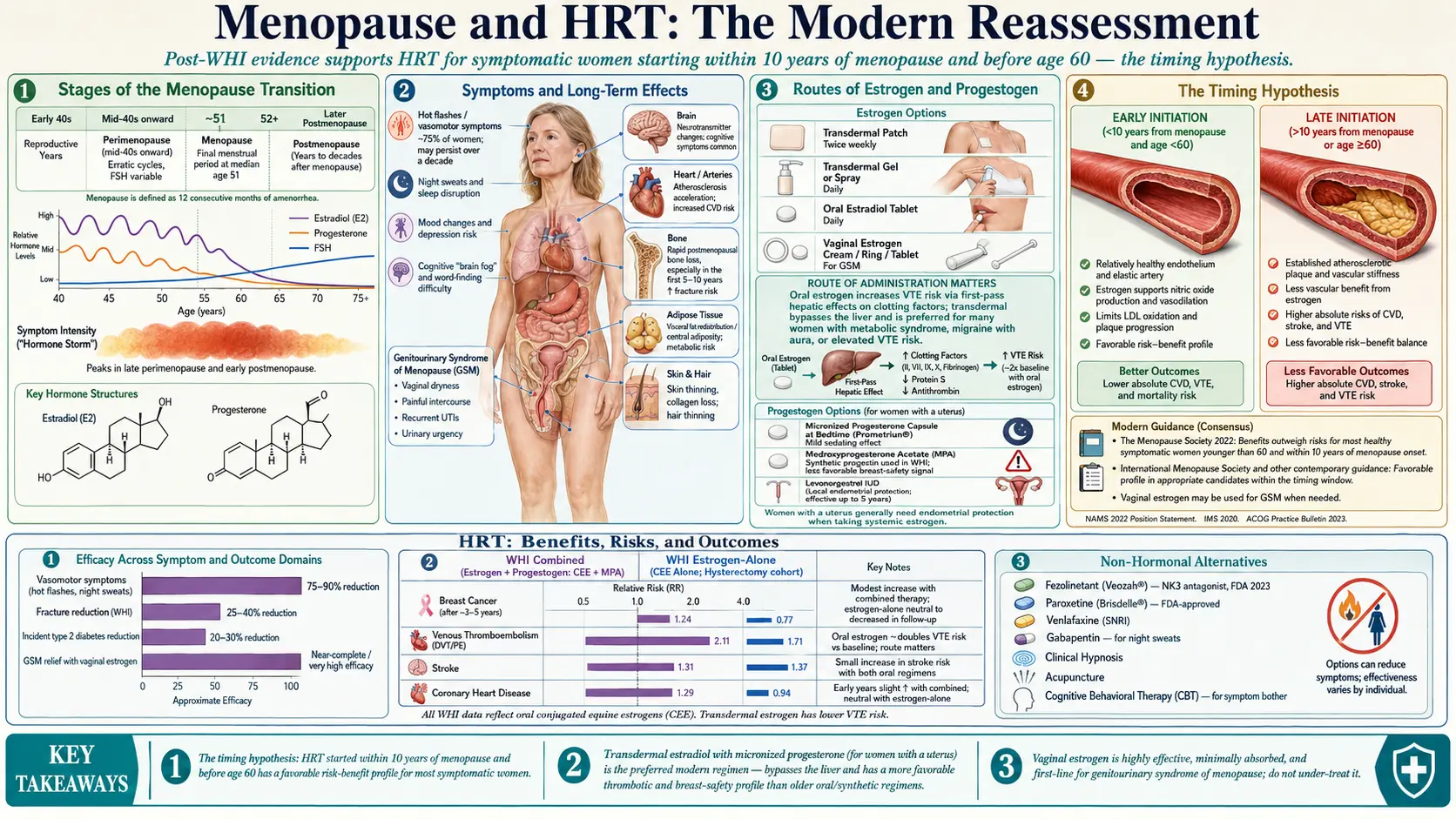
Menopause is the permanent cessation of menstruation that typically occurs between ages 45 and 55, marking the end of reproductive capacity and a substantial drop in ovarian estrogen and progesterone production. The transitional years leading up to menopause (perimenopause) and the decades after (postmenopause) are characterized by a constellation of symptoms and long-term health changes: hot flashes, night sweats, sleep disruption, mood changes, vaginal dryness and genitourinary syndrome, bone loss, cardiovascular risk changes, and metabolic shifts. Menopausal hormone therapy (MHT), still widely called HRT, replaces declining ovarian hormones and is the most effective treatment available for most menopausal symptoms.
After a generation of decline following misinterpretation of the 2002 Women’s Health Initiative (WHI) results, hormone therapy has undergone a thorough reappraisal. Current guidelines from The Menopause Society, the International Menopause Society, and other major bodies now strongly support MHT for appropriately selected women, particularly those who start within 10 years of menopause and before age 60 — the “timing hypothesis.” This article lays out the evidence, risks, modern formulations, and practical considerations.
Deep-Dive Articles
Perimenopause: Symptom Tracker & Hormonal Testing
How to recognize perimenopause, why FSH testing misleads, and what to track instead.
Estradiol Formulations: Patch, Gel, Oral
Comparing delivery routes, bioidentical vs synthetic, dosing, and when to pick each.
Micronized Progesterone vs Synthetic Progestins
Endometrial protection, sleep effects, and why formulation matters for breast cancer risk.
Testosterone Therapy for Women
Low libido, energy, off-label use, compounded pellets vs transdermal, and monitoring.
Hot Flashes & Night Sweats
Why they happen, what actually works, and when to escalate beyond lifestyle changes.
GSM & Vaginal Estrogen
Dryness, painful sex, recurrent UTIs: the most under-treated consequence of menopause.
HRT Risks: Breast Cancer, Clots, Stroke
The honest post-WHI picture: what the data actually show by age, route, and regimen.
Bone Loss Prevention & HRT
How estrogen protects bone, when HRT is first-line for osteoporosis prevention.
Non-Hormonal Options: SSRIs, Gabapentin, Fezolinetant
Veozah (fezolinetant), paroxetine, gabapentin, clonidine, oxybutynin — when HRT isn't an option.
Table of Contents
- Deep-Dive Articles
- Menopause Stages
- Symptoms and Long-Term Effects
- What Menopausal Hormone Therapy Is
- Benefits — The Evidence
- Risks — The Honest Picture
- The Timing Hypothesis
- Oral vs Transdermal
- Types of Progestogen
- Testosterone in Women
- Non-Hormonal Options
- Lifestyle Support
- Connections
- Featured Videos
Menopause Stages
- Perimenopause — The transition, typically starting in the mid-40s, when ovarian hormone production becomes erratic. Cycles shorten, lengthen, or skip. Symptoms often begin here.
- Menopause — Defined as 12 consecutive months without a menstrual period.
- Postmenopause — Every year thereafter. Symptoms may persist for years to decades.
Symptoms and Long-Term Effects
- Vasomotor symptoms (VMS). Hot flashes and night sweats affect roughly 75% of women and can persist for more than a decade on average.
- Sleep disturbance. Often secondary to VMS but also directly hormonal.
- Mood changes. Increased risk of depression, anxiety, irritability.
- Cognitive symptoms. Word-finding difficulty, brain fog, concentration loss — typically transient.
- Genitourinary syndrome of menopause (GSM). Vaginal dryness, painful intercourse, urinary frequency, recurrent UTIs. Often overlooked but highly treatable with local estrogen.
- Bone loss. Rapid loss in the first 5–10 years after menopause, driving osteoporosis risk.
- Cardiovascular changes. Acceleration of atherosclerosis and lipid worsening.
- Weight redistribution. Increased visceral fat.
- Skin and hair changes. Thinning, dryness, reduced elasticity.
What Menopausal Hormone Therapy Is
MHT typically replaces estrogen (most often estradiol) and, in women with a uterus, a progestogen to protect the endometrium from estrogen-induced overgrowth that could otherwise lead to endometrial cancer. Women who have had a hysterectomy can take estrogen alone. Routes of administration include:
- Transdermal patch — applied twice weekly.
- Transdermal gel or spray — daily.
- Oral tablet — daily.
- Vaginal estrogen — cream, ring, or tablet for GSM specifically, with minimal systemic absorption.
- Micronized progesterone — oral bedtime capsule (also has mild sedating/anxiolytic effect).
Benefits — The Evidence
- Vasomotor symptoms. MHT is the most effective treatment, typically reducing hot flashes by 75–90%.
- Sleep and mood. Improvement often follows VMS reduction; some direct benefit.
- Bone health. MHT prevents postmenopausal bone loss and reduces hip, vertebral, and all fractures by roughly 25–40% in WHI data.
- Cardiovascular. When started within 10 years of menopause, MHT is associated with reduced coronary events in re-analyses and in the Danish DOPS trial.
- Diabetes. Reduces incident type-2 diabetes by roughly 20–30%.
- Genitourinary symptoms. Vaginal estrogen is first-line and highly effective.
- Colorectal cancer. Modest reduction in some analyses.
- Quality of life. Consistent improvement.
Risks — The Honest Picture
- Breast cancer. Combined estrogen-progestogen MHT increases breast-cancer risk modestly after 3–5 years of use (an additional ~1 case per 1000 women-years in the WHI). Estrogen-alone MHT in the WHI was associated with reduced breast-cancer incidence. Micronized progesterone appears lower risk than synthetic progestins.
- Venous thromboembolism (VTE). Oral estrogen roughly doubles VTE risk; transdermal estrogen does not raise VTE risk and is preferred in higher-risk women.
- Stroke. Small increase with oral estrogen, particularly in older initiators.
- Gallbladder disease. Increased risk with oral estrogen.
- Endometrial cancer. Prevented by adequate progestogen in women with a uterus.
The Timing Hypothesis
The WHI’s widely publicized harms were driven largely by women who initiated MHT more than 10 years past menopause or after age 60, when arterial plaques may already be established. Pooled evidence strongly supports that initiation within 10 years of menopause and under age 60 carries a favorable risk-benefit profile for most women, particularly when symptomatic. Initiation later is not always harmful but the benefit margin is narrower.
Oral vs Transdermal
Oral estrogen undergoes first-pass liver metabolism, raising clotting factors, triglycerides, sex-hormone-binding globulin, and inflammatory markers. Transdermal estrogen bypasses this and has not been associated with increased VTE or stroke risk. For most women, especially those with metabolic-syndrome features, migraine with aura, or VTE risk factors, transdermal is preferred.
Types of Progestogen
Micronized oral progesterone (Prometrium) is structurally identical to natural progesterone, has a mild sedating effect helpful at bedtime, and appears to have a better breast-cancer safety signal than synthetic progestins in European cohort studies. Synthetic progestins (e.g., medroxyprogesterone acetate) remain effective for endometrial protection but carry the breast-cancer signal seen in WHI. Levonorgestrel IUDs provide effective endometrial protection with minimal systemic exposure.
Testosterone in Women
Low-dose testosterone supplementation is evidence-based for hypoactive sexual desire disorder (HSDD) in postmenopausal women. Benefits for energy, mood, and cognition are claimed clinically but not strongly established in randomized trials. Doses used are roughly one-tenth of male replacement doses, typically delivered as a compounded cream. No testosterone product is FDA-approved for women in the U.S. as of this writing.
Non-Hormonal Options
- Fezolinetant (Veozah) — a neurokinin-3 receptor antagonist approved in 2023 specifically for moderate-to-severe hot flashes.
- SSRIs and SNRIs — paroxetine (Brisdelle) is FDA-approved; venlafaxine and escitalopram also help VMS.
- Gabapentin — helps hot flashes especially at night.
- Cognitive behavioral therapy — reduces the bother of symptoms meaningfully.
- Clinical hypnosis — has good trial evidence for VMS.
- Acupuncture — modest but consistent trial signal.
Lifestyle Support
- Regular aerobic and resistance training — improves bone density, metabolic health, mood, and sleep.
- Adequate dietary protein (1.2 g/kg of goal weight) to preserve muscle mass.
- Weight management — adipose tissue generates estrogen but also drives VMS in a complex way.
- Sleep hygiene and stress management.
- Reduce alcohol — a major VMS and breast-cancer-risk modifier.
- Calcium (1200 mg/day from food), vitamin D adequate, magnesium, and vitamin K2 for bone.
Connections
- Menopause: Why the Hormones Fall and What Changes — interactive animation
- Perimenopause Symptom Tracker and Hormonal Testing
- Micronized Progesterone vs Synthetic Progestins
- Estradiol Formulations: Patch, Gel, Oral Routes
- HRT Risks: Breast Cancer, Clots and Stroke
- Testosterone Therapy for Women
- Vasomotor Symptoms: Hot Flashes and Night Sweats
- Bone Loss Prevention and HRT
- Genitourinary Syndrome of Menopause and Vaginal Estrogen
- Non-Hormonal Options: SSRIs, Gabapentin, Fezolinetant
- Perimenopause
- Calcium
- Depression
- Osteoporosis
- Hormone Panel
- Insomnia
- Cardiovascular Disease
- Vitamin D3
- Vitamin K
- Breast Cancer
- Ovarian Cancer
- Endometrial Cancer
- PMS and PMDD
- Urinary Incontinence
Research Papers
The following PubMed topic searches aggregate the current peer-reviewed literature. Each link opens a live PubMed query — results update as new studies are indexed.
- PubMed — menopause hormone therapy
- PubMed — Women's Health Initiative
- PubMed — transdermal estradiol
- PubMed — micronized progesterone
- PubMed — vasomotor symptoms menopause
- PubMed — genitourinary syndrome of menopause
- PubMed — menopause bone density
- PubMed — menopause cardiovascular risk
- PubMed — menopause cognition
- PubMed — testosterone women menopause
- PubMed — selective estrogen receptor modulator
- PubMed — menopause timing hypothesis