Fracture Prevention and Fall Risk
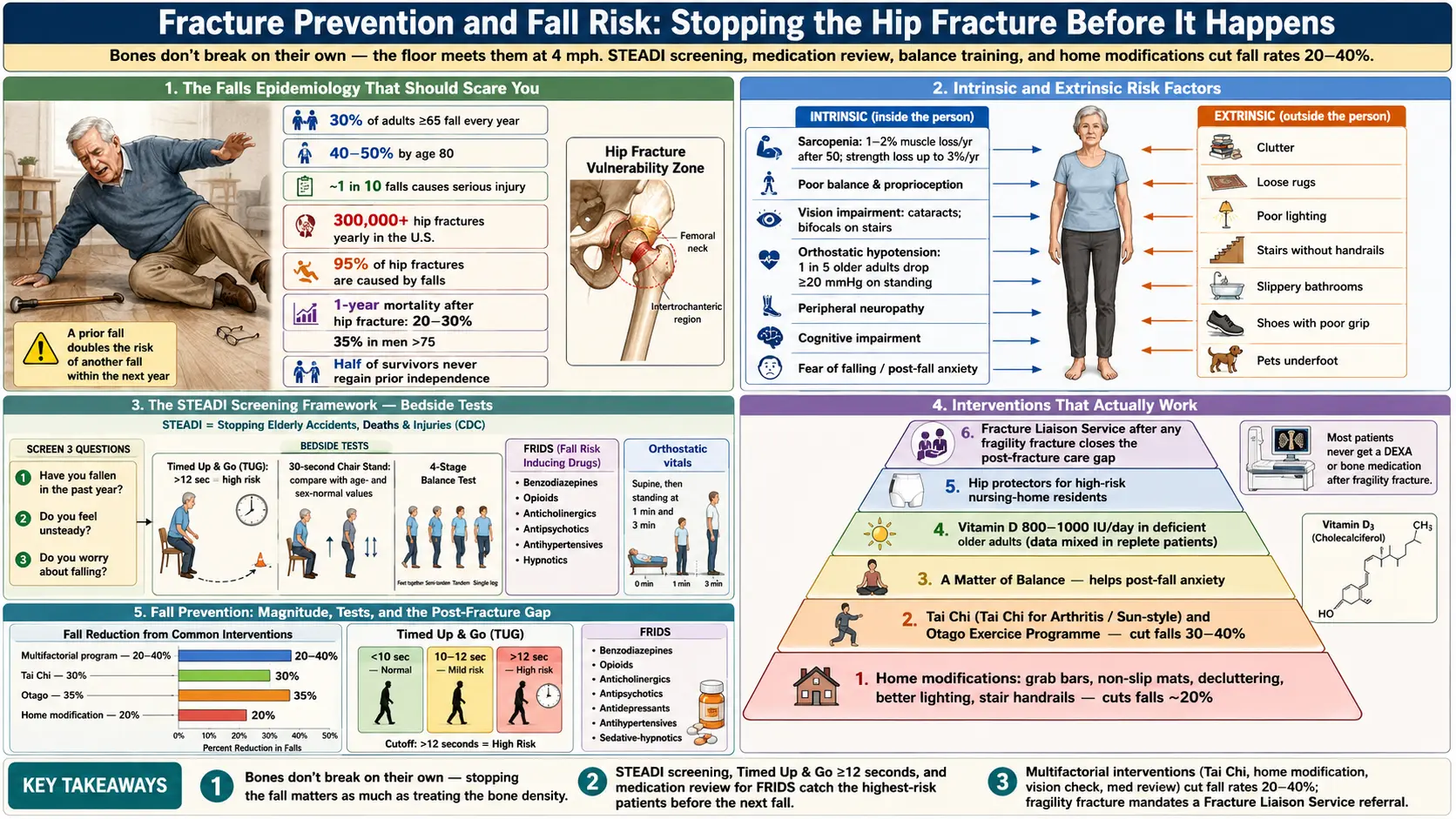
Table of Contents
- Why Falls, Not Bone Density, Break Hips
- The Epidemiology That Should Scare You (a Little)
- Intrinsic Risk Factors — What Is Happening Inside You
- Extrinsic Risk Factors — Your Environment
- The STEADI Screening Framework
- Timed Up & Go, 30-Second Chair Stand, and Other Bedside Tests
- The Medication Review Nobody Does
- Vitamin D for Fall Reduction — What the Evidence Actually Says
- Tai Chi, Otago, and A Matter of Balance
- Home Modifications That Actually Work
- Hip Protectors — The Unloved Intervention
- The Post-Fracture Care Gap and Fracture Liaison Services
- Putting It Together: A Personal Fall-Prevention Plan
- Key Research Papers
- Connections
- Featured Videos
Why Falls, Not Bone Density, Break Hips
Here is the uncomfortable truth that most osteoporosis conversations skip: bones do not break on their own. In the overwhelming majority of hip, wrist, and pelvic fractures, something tipped the person over first. That is why a 70-year-old with osteopenia who never falls rarely fractures, while a 70-year-old with the same T-score who falls twice a year ends up in the operating room.
Treating osteoporosis is not just about bisphosphonates and calcium. It is about making sure the floor never meets your hip at 4 mph. The bone-density work protects you if you fall. The fall-prevention work keeps you from falling in the first place. Both matter, and almost every serious fracture-prevention program does both simultaneously.
This page is the fall-prevention half of that equation. It is written for people who already know they have low bone density, for caregivers worried about an aging parent, and for anyone who has noticed a subtle loss of balance and wants to act before the first fracture — not after.
The Epidemiology That Should Scare You (a Little)
Numbers force clarity. Memorize these:
- About 30% of adults aged 65 and older fall at least once every year. By age 80, the annual figure is closer to 40–50%.
- Roughly 1 fall in 10 causes a serious injury — a fracture, a head injury, or a hospitalization.
- In the United States, more than 300,000 hip fractures occur each year, 95% of them caused by falls.
- One-year mortality after a hip fracture is 20–30%. Among men over 75, it is closer to 35%.
- Of those who survive the first year, roughly half never regain their prior level of independence. Many move permanently to assisted living.
- Having fallen once doubles your risk of falling again within the next year.
These are not numbers to panic over — they are numbers to plan around. Every item in the rest of this page chips away at them. A good fall-prevention program, consistently followed, typically reduces fall rates by 20–40%. Stack several interventions and the reduction compounds.
Intrinsic Risk Factors — What Is Happening Inside You
Intrinsic factors are the ones that travel with you. They are why the same icy sidewalk does not fracture every pedestrian.
Age and Sarcopenia
After age 50, the average adult loses about 1–2% of muscle mass and up to 3% of muscle strength per year. By 80, many people have lost 30–40% of the leg strength they had at 30. Weak quadriceps and hip abductors mean that when your center of mass drifts, you cannot catch it. Sarcopenia is the single most modifiable intrinsic risk factor — see the exercise article.
Balance and Proprioception
Balance is not a single skill. It depends on three inputs: the inner ear (vestibular), vision, and joint-position sense (proprioception). Any one can degrade with age; when two fail at once — cataracts plus peripheral neuropathy, for example — falls become nearly inevitable without training.
Vision
Poor vision roughly doubles fall risk. Uncorrected refractive error, cataracts, macular degeneration, and glaucoma all contribute. Bifocals and progressive lenses are a specific hazard on stairs because the near-reading segment blurs the step edge. Single-distance glasses for walking outdoors meaningfully reduces outdoor fall rates.
Orthostatic Hypotension
Roughly one in five older adults drops 20+ mmHg of systolic blood pressure on standing. The resulting lightheadedness — especially the first steps out of bed or after a meal — is a classic cause of unexplained falls. Check your own: lie flat for five minutes, record BP, stand, record at one and three minutes. A drop of 20 systolic or 10 diastolic is diagnostic.
Peripheral Neuropathy
Diabetic, chemotherapy-induced, alcoholic, or idiopathic neuropathy blunts the feedback from feet to brain. You literally cannot feel the floor. Patients often describe it as "walking on pillows." Neuropathy triples the risk of recurrent falls.
Cognitive Impairment
Mild cognitive impairment and dementia raise fall risk through several mechanisms: slower reaction time, impaired dual-tasking (walking while talking), poor judgment about hazards, and reduced ability to remember safety strategies. Patients with Alzheimer's disease fall at roughly twice the rate of cognitively intact peers.
Fear of Falling
After one fall, many older adults develop a conditioned fear that paradoxically increases risk: they stiffen, take shorter steps, avoid activity, lose more strength, and fall again. The syndrome has a name — post-fall anxiety — and it is specifically addressed by programs like A Matter of Balance (below).
Extrinsic Risk Factors — Your Environment
Most falls among older adults happen at home, on flat ground, in familiar rooms, during routine activities. The environment is rarely exotic. The usual culprits:
- Throw rugs and loose mats. The single most common indoor trip hazard. Especially dangerous on smooth floors or at thresholds.
- Poor lighting. Hallways, stairs, and bathrooms at night. Aging eyes need roughly three times the light that a 20-year-old's eyes need to see the same detail.
- Clutter. Electrical cords, shoes in doorways, pet bowls, magazines stacked on the floor.
- Bathrooms. Wet tile, tub edges, and low toilets without grab bars cause a disproportionate share of hip fractures.
- Stairs. Especially stairs without a sturdy handrail on both sides, without contrast strips on the edges, or carpeted in a pattern that hides step boundaries.
- Footwear. Backless slippers, socks on hardwood, high heels, and shoes with worn-out soles.
- Outdoor hazards. Uneven sidewalks, ice, leaves, curbs, poorly lit parking lots.
- Pets. Dogs and cats underfoot account for 1–2% of fall-related ER visits in older adults.
The STEADI Screening Framework
The CDC's STEADI initiative — Stopping Elderly Accidents, Deaths, and Injuries — is the practical toolkit your primary-care doctor should be using with every patient 65+. It takes about 10 minutes and consists of three steps:
1. Screen. Three yes/no questions:
- Have you fallen in the past year?
- Do you feel unsteady when standing or walking?
- Do you worry about falling?
A "yes" to any one triggers the next step. Alternatively, the 12-item Stay Independent questionnaire gives a numeric fall-risk score.
2. Assess. The clinician performs a structured evaluation: gait and balance testing (below), orthostatic vitals, medication review, visual acuity check, foot exam, and a cognitive screen (Mini-Cog or similar).
3. Intervene. Targeted actions based on what was found: physical therapy referral, medication deprescribing, home safety evaluation by occupational therapy, vitamin D check, cataract referral, and so on.
If your doctor has never run you through STEADI, you can prompt them. Say: "I am worried about falls. Can we do a STEADI assessment at my next visit?" The materials — patient brochures, provider checklists, pocket cards — are all free at the CDC website.
Timed Up & Go, 30-Second Chair Stand, and Other Bedside Tests
You do not need a laboratory to measure fall risk. Two three-minute tests capture most of it. Try them at home with a stopwatch and a sturdy armchair.
Timed Up & Go (TUG)
Sit in a standard chair. On "go," stand up, walk 10 feet (3 meters) at a normal pace, turn around, walk back, and sit down. Time the whole maneuver.
- Under 10 seconds — normal mobility.
- 10–12 seconds — mild impairment; worth addressing.
- 12 seconds or more — significantly elevated fall risk. Physical therapy referral is warranted.
- 14 seconds or more — high risk of recurrent falls.
30-Second Chair Stand
Sit in a standard chair with arms folded across your chest. On "go," stand fully upright and sit back down as many times as possible in 30 seconds. Count completed stands. Age- and sex-stratified thresholds — below the cutoff indicates elevated fall risk:
- Women 60–64: below 12; 65–69: below 11; 70–74: below 10; 75–79: below 10; 80–84: below 9; 85+: below 8.
- Men 60–64: below 14; 65–69: below 12; 70–74: below 12; 75–79: below 11; 80–84: below 10; 85+: below 8.
4-Stage Balance Test
Four progressively harder stances, each held for 10 seconds: feet side-by-side, one foot half in front of the other (semi-tandem), feet in a full tandem line, then single-leg stance. Inability to hold full tandem for 10 seconds predicts a fourfold rise in injurious falls.
These tests are worth doing every six to twelve months after age 65. Trending them over time catches decline early, when it is still reversible with exercise.
The Medication Review Nobody Does
Medications are one of the most under-addressed fall-risk factors. Every additional drug on your list raises risk a little; several classes raise it a lot. Ask your prescriber to run through this list with you. Reference frameworks: the Beers Criteria (American Geriatrics Society) and STOPP/START criteria (European).
Highest-Risk Classes
- Benzodiazepines (alprazolam, lorazepam, diazepam, clonazepam). Increase fall risk roughly 50%, and the risk persists for weeks after starting. Beers-listed for avoidance in adults 65+. If used for sleep, every single night, the case for deprescribing is strong.
- "Z-drugs" / non-benzodiazepine hypnotics (zolpidem, eszopiclone, zaleplon). Once marketed as safer alternatives; real-world data show fall and fracture risk comparable to benzodiazepines.
- Opioids. Sedation, orthostatic hypotension, slowed reflexes. Risk is highest in the first two weeks of a new prescription or after dose escalation.
- Anticholinergics. A surprisingly broad class: diphenhydramine (Benadryl, many PM sleep aids), oxybutynin, tolterodine, amitriptyline, paroxetine, cyclobenzaprine, scopolamine, promethazine. Calculate your "anticholinergic burden" with the ACB Scale; a score of 3+ is associated with substantially higher fall and cognitive risk.
- Tricyclic antidepressants (amitriptyline, nortriptyline, imipramine). Orthostatic hypotension, anticholinergic load.
- Certain SSRIs. Paroxetine in particular; most SSRIs raise fall risk modestly, and many older adults are left on them indefinitely without a fresh indication review.
- Antipsychotics — especially in dementia, where they are frequently inappropriate.
- Antihypertensives in aggressive combinations. Over-treatment of blood pressure in frail older adults is a common cause of orthostatic falls. Target systolic is usually 130–140 in frailer patients, not the 120 used in younger cohorts.
- Alpha-blockers (terazosin, doxazosin, tamsulosin) — orthostatic hypotension on dose initiation.
- Insulin and sulfonylureas (glipizide, glyburide). Hypoglycemia, especially overnight.
- SGLT2 inhibitors (empagliflozin, dapagliflozin, canagliflozin). Though less hypoglycemic than sulfonylureas, they promote volume depletion and orthostatic drops; several registry analyses show modestly increased fall risk in frail elderly.
Proton Pump Inhibitors — The Quiet Contributor
Long-term PPI use (omeprazole, pantoprazole, esomeprazole, and relatives) has been associated with a 10–30% increased risk of hip fracture in observational studies. The proposed mechanism is reduced calcium absorption and accelerated bone turnover. PPIs do not cause falls directly, but they reduce the bone's tolerance for the ones that do happen. If you have been on a PPI for more than a year without a clear ongoing indication (Barrett's esophagus, erosive esophagitis, NSAID gastroprotection), ask about a trial off.
How to Actually Deprescribe
Bring your full medication list — including over-the-counter sleep aids, allergy pills, and supplements — to a dedicated appointment. Ask: "Which of these raises my fall risk? Which can we taper or stop?" Most high-risk drugs require a gradual taper; abrupt discontinuation of benzodiazepines, opioids, or SSRIs can be dangerous in its own right. A pharmacist-led medication review (covered by Medicare's annual wellness visit) is one of the highest-yield hours an older adult can spend.
Vitamin D for Fall Reduction — What the Evidence Actually Says
The vitamin D fall-prevention story has gone in a circle. Early trials in the 2000s suggested that 800 IU daily reduced falls by roughly 20%. This led to broad recommendations to supplement every older adult. More recent, larger trials — including the VITAL substudy and the 2018 USPSTF evidence review — show that in community-dwelling older adults who are not vitamin D deficient, supplementation does not meaningfully reduce falls or fractures. Very high doses (50,000 IU monthly or 60,000 IU monthly) have actually increased falls in some studies.
What survives the scrutiny:
- If you are vitamin D deficient (25-hydroxyvitamin D below 20 ng/mL, or arguably below 30), repletion reduces falls and improves muscle function. The effect is largest in institutionalized older adults, where deficiency is common.
- A reasonable daily dose for most older adults is 800–2000 IU, aiming for a serum 25-OH-D of 30–50 ng/mL. See the dedicated Vitamin D3 page and the calcium, D, and protein article.
- Mega-doses are not better. Avoid 50,000 IU weekly or monthly pulsed regimens unless specifically prescribed for a documented severe deficiency.
Tai Chi, Otago, and A Matter of Balance
Exercise is the single most evidence-backed fall-prevention intervention. The effect sizes are among the largest in geriatrics: well-designed programs cut fall rates by 20–30% and injurious falls by more.
Tai Chi
A 2017 meta-analysis of 18 trials with over 3,800 participants (Huang et al.) found that regular tai chi reduced fall rates by about 20% in community-dwelling older adults. The Tai Ji Quan: Moving for Better Balance program, a simplified eight-form version developed at the Oregon Research Institute, has been adopted by CDC and YMCA chapters nationwide. Typical dose: 60 minutes, twice weekly, for 24 weeks. Effect builds slowly; meaningful balance gains usually appear around week 12.
Otago Exercise Program
Developed in New Zealand, Otago is a set of 17 progressive strength and balance exercises performed at home, three times weekly for 30 minutes, plus a short walk twice weekly. A physical therapist visits to teach and progress the program. In the original trials and multiple replications, Otago reduced falls by roughly 35% in higher-risk older adults (age 80+ or with a history of falling). It is Medicare-covered when prescribed by a physician through home health or outpatient PT.
A Matter of Balance
An eight-session group program designed specifically for people with fear of falling — the post-fall anxiety that keeps people indoors and accelerates deconditioning. Combines cognitive-behavioral techniques, gentle exercise, and problem-solving. Delivered free or low-cost through many Area Agencies on Aging. Trials show reduced falls and, importantly, restored willingness to go outside.
General Dose Guidance
Across programs, three common threads predict success: balance challenge must be genuine (standing on one leg, narrow stances, dual tasks), strength work targets legs and hips, and total dose exceeds 50 hours over at least 12 weeks. Less than that rarely moves the needle.
Home Modifications That Actually Work
An occupational-therapy home assessment, performed once in your own rooms, is worth more than any generic checklist. If that is not available, work through this list yourself. Nearly all of it costs under $500 total and takes a weekend.
Lighting
- Motion-activated nightlights in hallways and bathrooms.
- A bedside lamp you can reach without getting up.
- Brighter bulbs in stairwells — at least 60W equivalent LED, 2700K or higher.
- Light switches at both the top and bottom of every staircase.
Bathrooms
- Grab bars installed into wall studs (not suction cups) next to the toilet and inside the tub or shower.
- A non-slip mat inside the tub and a textured mat outside.
- A shower chair or bench for anyone with leg weakness.
- A raised toilet seat (3-inch elevation) if hip or knee problems make sit-to-stand hard.
- A hand-held shower head.
Floors
- Remove throw rugs, or at minimum secure them with double-sided rug tape.
- Fix raised thresholds between rooms.
- Tape down or reroute electrical cords out of walking paths.
- Declutter high-traffic corridors.
Stairs
- Sturdy handrails on both sides of every staircase, extending slightly past the top and bottom steps.
- Contrast strips on the edge of each step if the carpet or paint hides the transition.
- A secure gate at the top of stairs if cognitive impairment is a concern.
Bedroom and Kitchen
- Frequently used items between waist and shoulder height — no climbing, no deep bending.
- A sturdy step stool with a handle for unavoidable high reaches.
- A phone reachable from the floor in case of a fall (an Apple Watch or a medical alert pendant serves the same purpose).
Footwear
Indoor: closed-heel shoes or slippers with rubber soles. Outdoor: low heels, broad base, good tread, and ideally ties or Velcro rather than slip-ons. In winter, ice cleats that strap over regular shoes (Yaktrax and similar) dramatically reduce outdoor falls.
Hip Protectors — The Unloved Intervention
Hip protectors are padded undergarments with foam or hard-shell pads positioned over the greater trochanter of each hip. A hard-shell protector redirects the force of a sideways fall away from the femoral neck.
The Cochrane systematic review of hip protectors (Santesso 2014) concluded that in the specific setting of institutional care (nursing homes, assisted living), hip protectors produce a modest but real reduction in hip fractures — about 11 fractures prevented per 1000 residents per year. In community-dwelling older adults, the benefit is smaller and often not statistically significant, mostly because adherence collapses: people find them bulky, hot, and uncomfortable in pajamas.
Realistic use case: a high-risk older adult living in assisted living, recently hospitalized for a fall, or with a history of one hip fracture on the other side. Brands like HipSaver and Safehip are sold direct-to-consumer for roughly $70–$100 per pair. Three pairs allow daily rotation through the laundry. Wear them at minimum during waking hours; many falls in frail older adults happen in the evening or overnight bathroom trip.
The Post-Fracture Care Gap and Fracture Liaison Services
Here is the most-broken part of the system, and the easiest to fix if you are the patient or family member advocating for care: after a hip or vertebral fracture, fewer than 25% of patients in the United States are ever started on osteoporosis medication. The orthopedic surgeon fixes the bone; the hospitalist manages the acute stay; the primary care doctor inherits the patient; and somewhere in the handoffs, nobody writes the prescription that could cut the risk of the second fracture in half.
A prior fragility fracture roughly doubles the risk of a future fracture. A hip fracture on one side raises the risk of a hip fracture on the other side by a factor of 2 to 5. This is the population with the most to gain from bisphosphonates, denosumab, or anabolic agents, and simultaneously the population least likely to receive them.
The Fracture Liaison Service (FLS) Model
A Fracture Liaison Service is a nurse-coordinator-driven program embedded in a hospital or orthopedics practice. The FLS nurse systematically identifies every patient admitted with a fragility fracture, orders appropriate workup (DEXA, calcium, 25-OH-D, PTH, sometimes celiac serology or protein electrophoresis), starts therapy or schedules it within 8 weeks of discharge, and hands off to primary care with a written plan.
Where FLS programs exist, secondary fracture rates drop 30–40%. They are standard of care in Australia, the UK, and much of Europe; in the U.S. they are spreading but still spotty. The American Society for Bone and Mineral Research and the National Bone Health Alliance maintain a directory of certified FLS sites (boneallianceinfo.org).
What to Do if Your Hospital Has No FLS
After any fragility fracture — hip, vertebra, wrist, pelvis, humerus — in anyone 50 or older, push for these three actions before leaving the hospital or at the first follow-up:
- A DEXA scan within 3 months (if not done recently).
- A basic workup for secondary causes — see secondary osteoporosis.
- A specific osteoporosis medication prescribed before discharge or at the first outpatient visit. Zoledronic acid (a single annual IV infusion) is particularly suited to the post-fracture setting because adherence with oral bisphosphonates in frail older adults is notoriously poor.
Putting It Together: A Personal Fall-Prevention Plan
If you want one practical sequence to run this month, do these in order:
- Test yourself. Stopwatch, armchair, 30-Second Chair Stand, Timed Up & Go. Write down the numbers.
- Book a medication review. Bring every pill and supplement. Ask specifically about anticholinergics, sleep aids, PPIs, and antihypertensive burden.
- Get a vitamin D level, not a prophylactic megadose. Supplement only if below 30 ng/mL, targeting 30–50.
- Eye exam. Update glasses; consider separate single-distance pairs for walking and reading.
- Walk through your home at dusk with the lights you normally use. Photograph hazards. Fix the top five this weekend.
- Sign up for a structured program. Tai Chi: Moving for Better Balance, Otago, or A Matter of Balance — whichever is available locally. Commit to 12 weeks.
- If you have osteoporosis, confirm you are on appropriate pharmacotherapy. See the osteoporosis overview.
- After any fall, even one without injury, schedule a visit within a week. Do not normalize "I'm fine." Falls cluster.
Done consistently, this combination cuts fall risk by roughly a third to a half. For a person whose bone density puts them on the edge of a fragility fracture, that is frequently the difference between a long independent life and a year in a rehab facility.
Key Research Papers
Foundational randomized trials, Cochrane reviews, and major guidelines underpinning the fall-prevention, exercise, medication-deprescribing, and post-fracture care recommendations on this page.
- Tinetti ME, Baker DI, McAvay G, et al. A Multifactorial Intervention to Reduce the Risk of Falling Among Elderly People Living in the Community. New England Journal of Medicine. 1994;331(13):821–827.
- Lamb SE, Jørstad-Stein EC, Hauer K, Becker C; Prevention of Falls Network Europe. Development of a Common Outcome Data Set for Fall Injury Prevention Trials: The ProFaNE Consensus. Journal of the American Geriatrics Society. 2005;53(9):1618–1622.
- Liu-Ambrose T, Davis JC, Best JR, et al. Effect of a Home-Based Exercise Program on Subsequent Falls Among Community-Dwelling High-Risk Older Adults After a Fall: A Randomized Clinical Trial. JAMA. 2019;321(21):2092–2100.
- Sherrington C, Fairhall NJ, Wallbank GK, et al. Exercise for Preventing Falls in Older People Living in the Community. Cochrane Database of Systematic Reviews. 2019;1(1):CD012424.
- Gillespie LD, Robertson MC, Gillespie WJ, et al. Interventions for Preventing Falls in Older People Living in the Community. Cochrane Database of Systematic Reviews. 2012;9:CD007146.
- Huang ZG, Feng YH, Li YH, Lv CS. Systematic Review and Meta-Analysis: Tai Chi for Preventing Falls in Older Adults. BMJ Open. 2017;7(2):e013661.
- Thomas S, Mackintosh S, Halbert J. Does the Otago Exercise Programme Reduce Mortality and Falls in Older Adults? A Systematic Review and Meta-Analysis. Age and Ageing. 2010;39(6):681–687.
- LeBoff MS, Chou SH, Ratliff KA, et al. Supplemental Vitamin D and Incident Fractures in Midlife and Older Adults (VITAL). New England Journal of Medicine. 2022;387(4):299–309.
- US Preventive Services Task Force; Grossman DC, Curry SJ, et al. Interventions to Prevent Falls in Community-Dwelling Older Adults: USPSTF Recommendation Statement. JAMA. 2018;319(16):1696–1704.
- Santesso N, Carrasco-Labra A, Brignardello-Petersen R. Hip Protectors for Preventing Hip Fractures in Older People. Cochrane Database of Systematic Reviews. 2014;3:CD001255.
- Wu CH, Tu ST, Chang YF, et al. Fracture Liaison Services Improve Outcomes of Patients with Osteoporosis-Related Fractures: A Systematic Literature Review and Meta-Analysis. Bone. 2018;111:92–100.
- 2023 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2023 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults. Journal of the American Geriatrics Society. 2023;71(7):2052–2081.
- Cosman F, de Beur SJ, LeBoff MS, et al. Clinician's Guide to Prevention and Treatment of Osteoporosis. Osteoporosis International. 2014;25(10):2359–2381.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: fall prevention community older adults
- PubMed: STEADI screening
- PubMed: Timed Up & Go fall risk
- PubMed: tai chi fall prevention
- PubMed: Otago exercise program
- PubMed: benzodiazepines falls elderly
- PubMed: anticholinergic burden falls
- PubMed: proton pump inhibitor hip fracture
- PubMed: vitamin D supplementation falls
- PubMed: hip protectors fracture prevention
- PubMed: fracture liaison service
- PubMed: orthostatic hypotension falls
Connections
- Bone Remodeling & Calcium Balance — interactive animation
- Osteoporosis
- Bisphosphonates
- DEXA Scan: T-Score and Z-Score
- Vitamin D3
- Weight-Bearing and Resistance Exercise
- Secondary Osteoporosis Causes
- Denosumab, Romosozumab and Teriparatide
- Calcium, Vitamin D and Protein Intake
- FRAX Risk Assessment
- Postmenopausal Osteoporosis and Hormone Therapy
- Arthritis
- Calcium
- Dementia
- Peripheral Neuropathy
- Cataracts
- Interventional Pain