Weight-Bearing and Resistance Exercise for Bone Density
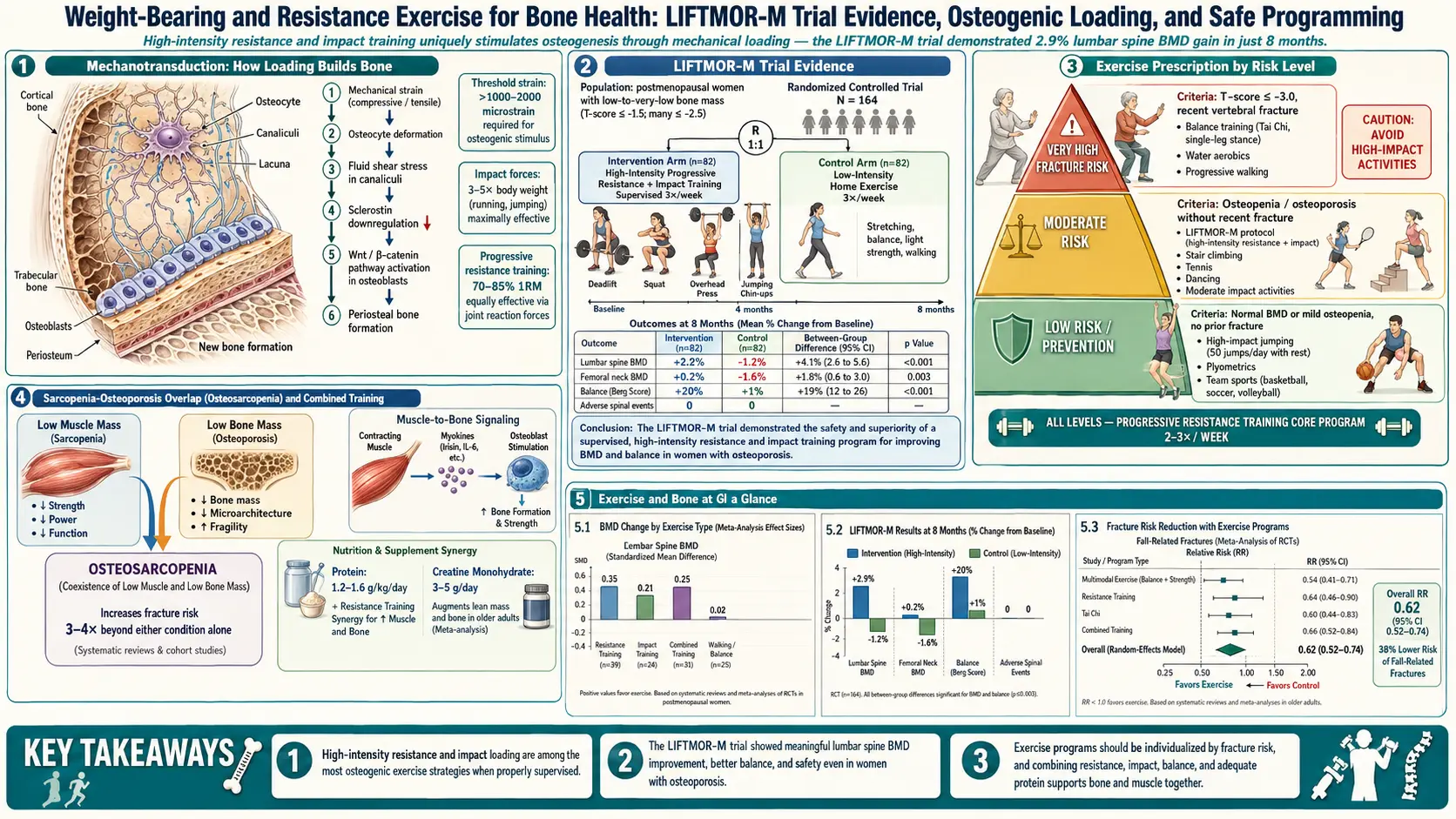
Table of Contents
- Why Exercise Actually Builds Bone
- Wolff's Law and the Osteocyte
- The LIFTMOR Trial — Heavy Lifting Changed the Rules
- LIFTMOR-M — Same Protocol in Older Men
- The Onero Program — LIFTMOR Translated to the Clinic
- Walking, Jogging, Stair Climbing vs Swimming and Cycling
- The Spinal Flexion Danger — Sinaki's Warning
- Balance Training — Tai Chi, Otago, and Why Falls Matter More Than Form
- Whole-Body Vibration Platforms — Limited Evidence
- Your Weekly Exercise Prescription
- Post-Fracture Rehabilitation
- Finding a Qualified Therapist — BoneFit and Beyond
- Getting Started Safely If You're New to Lifting
- Key Research Papers
- Connections
- Featured Videos
Why Exercise Actually Builds Bone
Bone is not an inert scaffold. It is a living tissue that is torn down and rebuilt every day of your life by two cell types working in balance: osteoclasts (demolition) and osteoblasts (construction). In a healthy young adult those two crews work at roughly the same rate. After menopause — or after enough years of low estrogen, low testosterone, chronic inflammation, or sedentary living — the demolition crew runs ahead of the builders, and you lose bone faster than you make it.
Drugs like bisphosphonates, denosumab, and romosozumab shift that balance pharmacologically. Exercise shifts it mechanically. When you load a bone — really load it, with force well above everyday walking — the cells inside the bone interpret that strain as a signal: we need to be stronger here. Over weeks and months, they lay down new mineral along the lines of stress. This is not folklore. It is the most reproducible finding in skeletal biology, going back 150 years.
The practical implication is that the type of exercise matters enormously. Gentle walking is good for your heart and your mood, but it does not reliably build bone density in someone with osteoporosis. Swimming and cycling, while excellent cardio, do nothing measurable for the skeleton. To move the needle on a DEXA scan you need load, impact, or both — and you need enough of it, often enough, for long enough. This article walks through exactly what that looks like in 2026.
Wolff's Law and the Osteocyte
In 1892 the German surgeon Julius Wolff published what became known as Wolff's law: bone remodels in response to the mechanical loads placed upon it. Put force through it and it thickens; take force away and it wastes. Astronauts lose roughly 1–2% of hip bone mineral density per month in microgravity — a natural experiment that confirms the law in its most extreme form.
The cellular machinery behind Wolff's law was identified over the last thirty years. Buried inside the mineralized matrix of your bones are the osteocytes — former osteoblasts that walled themselves into tiny cavities called lacunae. They extend long, spidery processes through microscopic channels (canaliculi) and talk to each other and to the surface cells through these extensions. Osteocytes make up more than 90% of the cells in adult bone, and they are the skeleton's master sensors.
When you load a bone, the fluid in the canaliculi shears past the osteocyte processes. The cells detect that flow and respond chemically. The most important molecule in this response is sclerostin, a protein that osteocytes secrete to suppress bone formation. Mechanical loading turns sclerostin off, which unleashes the Wnt signaling pathway, which tells osteoblasts to start laying down matrix. (The drug romosozumab is an antibody against sclerostin — a pharmacological mimic of what heavy exercise does naturally.)
A second signal comes from the strain rate. Bones respond to how quickly load is applied, not just how much. A slow, steady load — standing still, holding a bag — produces almost no osteogenic response. A fast, dynamic load — a heavy deadlift, a hop, a stomp — produces a large one. This is why researchers chasing bone adaptation consistently land on the same two tools: heavy resistance training (high absolute load, moderate speed) and impact (moderate load, very high speed).
The LIFTMOR Trial — Heavy Lifting Changed the Rules
For decades, postmenopausal women with low bone density were told to avoid heavy lifting. The fear was fracture. The advice was walking, light weights, maybe water aerobics. Density held steady, at best.
In 2018 a research group at Griffith University in Australia, led by Belinda Beck, published results from the LIFTMOR trial (Lifting Intervention For Training Muscle and Osteoporosis Rehabilitation) that reversed the conventional wisdom. They recruited 101 postmenopausal women with osteopenia or osteoporosis and randomized them to either eight months of supervised, high-intensity resistance and impact training (HiRIT) twice a week for 30 minutes, or a home-based low-intensity exercise program that resembled what most guidelines then recommended.
The intervention arm did things women with low BMD were never supposed to do. Deadlifts, overhead presses, and back squats performed at 80–85% of one-rep maximum — genuinely heavy weights — for five sets of five repetitions. Plus jumping chin-ups with drop landings, a high-impact move that delivered 3–5 times body weight through the hips on impact.
The results were striking. After eight months the HiRIT group gained roughly 2.9% in lumbar spine BMD and 0.3% at the femoral neck, while the control group lost bone at both sites. Height and functional performance (timed up-and-go, back extensor strength) improved in the lifting group. And critically, despite the supposedly dangerous movements, there were no fractures or serious adverse events, and compliance was 80% — higher than in most low-intensity trials. See the published results here.
LIFTMOR did not just show that heavy lifting was safe — it showed that in this population it was necessary. The low-intensity program did not maintain bone. Only the heavy program did. The trial has since been replicated in several cohorts and has reshaped osteoporosis exercise guidelines internationally.
LIFTMOR-M — Same Protocol in Older Men
Men get osteoporosis too — about a third of hip fractures globally occur in men, and their one-year mortality after a hip fracture is roughly double that of women. But nearly every exercise-for-bone trial up to 2019 had been in postmenopausal women.
Beck's group followed up with LIFTMOR-M, applying the same eight-month HiRIT protocol to 93 men over 50 with low BMD. They compared it both to a machine-based moderate resistance program and to a non-exercise control. Heavy lifting again won. The HiRIT men gained lumbar spine BMD and femoral neck cortical thickness, with gains significantly larger than the machine-based group. Functional markers (jump height, back extensor strength, stair climb) also improved more. Safety was equivalent: no fractures, low dropout. The published results are here.
The takeaway for men: the advice is the same. Heavy compound lifts, high-impact movement, supervised if you've never lifted, twice a week, for the rest of your life.
The Onero Program — LIFTMOR Translated to the Clinic
LIFTMOR was a research protocol run by exercise scientists. To translate it into something a regular physical therapist or trainer could deliver safely, Beck's group developed Onero — a trademarked, licensed program that certifies clinicians to run LIFTMOR-style classes in community clinics. Onero sessions are typically 30 minutes, twice a week, and follow the same skeletal targets: heavy loaded compound lifts plus impact work, supervised one-on-one or in very small groups.
Real-world data from Onero clinics now show similar results to the original trial. A 2022 implementation study tracked over a hundred participants through 12 months of Onero in Australian community settings and reported BMD gains at the spine and hip consistent with the research-grade protocol — again with no fractures.
In the United States, Onero-trained providers are slowly emerging, and several other brand-name programs (Bone Builders, Strong Bones, OsteoStrong — though OsteoStrong uses static isometric devices rather than free weights and has far weaker evidence) occupy the same niche. What you want, if you can find it, is a supervised program that uses barbells or heavy dumbbells, progresses load aggressively, includes impact drops or hops, and has a physical therapist or exercise physiologist watching your form.
Walking, Jogging, Stair Climbing vs Swimming and Cycling
A perennial patient question: "I walk three miles a day — isn't that enough?" The honest answer is: it's better than nothing, and it helps your cardiovascular system, your mood, and your fall risk. But for bone density in an established osteoporotic skeleton, walking alone is usually insufficient.
Here is the rough hierarchy of aerobic activities ranked by bone-loading intensity:
- Jumping and hopping — ground reaction forces of 3–5+ times body weight. Highly osteogenic.
- Running and jogging — roughly 2–3 times body weight per step. Moderately osteogenic. Trials in premenopausal women consistently show higher hip and spine BMD in runners than in sedentary controls.
- Stair climbing — loads the hip and spine well; the vertical component is particularly useful for the femoral neck. Cheap, accessible, underrated.
- Brisk walking — roughly 1–1.2 times body weight. Helpful for maintaining bone but rarely sufficient to build it in someone already below a T-score of -2.0.
- Swimming — effectively unloaded; the water carries your weight. Zero direct osteogenic stimulus. Excellent for arthritis and cardiac fitness; useless for bone.
- Cycling — also unloaded for most of the gait cycle. Competitive cyclists, despite enormous fitness, consistently show lower BMD than age-matched runners, and sometimes lower than sedentary controls. Endurance cycling is a known secondary risk factor for low BMD in male athletes.
This does not mean you should stop swimming if you love it. It means you should not only swim. Pair it with two resistance sessions and a bit of impact, and you have a complete program.
The Spinal Flexion Danger — Sinaki's Warning
Every osteoporosis exercise article should include this caution, because it is one of the few places the field has a clear "do not do this" recommendation.
In the early 1980s, Mehrsheed Sinaki at the Mayo Clinic followed a cohort of postmenopausal women with osteoporosis who had been prescribed one of three home exercise programs: spinal extension exercises (strengthening the muscles that pull the spine upright), spinal flexion exercises (classic sit-ups, toe-touches, the McKenzie flexion routine common in low back pain care), a combination of both, or no exercise. She tracked them for one to two years and imaged their spines for new vertebral wedge fractures.
The results, published in the Archives of Physical Medicine and Rehabilitation in 1984, were alarming enough that they changed practice: 89% of the flexion-only group developed new vertebral wedge fractures, compared to 16% of the extension-only group and 53% of the combination group. The un-exercised controls fell in between. The published paper is Search PubMed.
The mechanism makes intuitive sense. Vertebrae lose bone asymmetrically in osteoporosis, and the front (anterior) of each vertebral body tends to thin faster than the back. Forward flexion — bending over, touching toes, doing crunches, loading a rounded spine — multiplies the compressive force on that already thinned anterior edge. In a severely osteoporotic spine, a single hard flexion movement can crush the front of a vertebra into a wedge shape, which then cascades into postural kyphosis.
Practical rules:
- No sit-ups, crunches, or toe-touches if your T-score is below -2.0 or you have a known vertebral fracture.
- No loaded spinal flexion — meaning do not pick up grocery bags by bending forward from the waist. Hinge at the hips, keep the spine neutral, bend the knees, and lift with the legs.
- The McKenzie flexion-based program commonly taught for disc-related low back pain is contraindicated in established osteoporosis. The McKenzie extension-based program is usually fine and often helpful.
- Yoga and Pilates are mixed. Many poses (forward folds, rolling spine articulations, deep twists with flexion) are risky. A well-trained instructor who knows your diagnosis can adapt the practice; a general class cannot.
- Do strengthen the back extensors. Prone "cobra" lifts, supermans, bird-dogs, and loaded row variations are your friends. A stronger extensor chain supports the spine and reduces kyphotic drift.
Balance Training — Tai Chi, Otago, and Why Falls Matter More Than Form
Here is a humbling fact: the vast majority of osteoporotic fractures happen because the person fell, not because their bones spontaneously failed. The hip fractures, the wrist fractures, the pelvis fractures, even many of the vertebral fractures — they trace back to a trip, a slip, a stumble. Which means that fall-prevention training is, statistically, as important as bone-building training. Possibly more so in people over 75.
Two evidence-based programs dominate this space:
Tai Chi. Multiple randomized trials have found that 6–12 months of Tai Chi reduces fall rates in older adults by roughly 30–50%. The slow, continuous weight shifts, the single-leg stances, and the trained attention to posture retrain the postural control system. Even community-center Tai Chi (free or low-cost) has measurable benefits. See a representative meta-analysis here.
The Otago Exercise Program. Developed in New Zealand in the 1990s, Otago is a structured home-based program of progressive leg-strengthening exercises plus balance drills, delivered by a physical therapist in 4–5 initial home visits and followed up by phone. In the original trials and subsequent meta-analyses, Otago reduces falls in adults 80 and over by about 35% and reduces fall-related injuries by a similar amount. Many Medicare Advantage plans in the U.S. now cover Otago-certified physical therapists.
Practical balance training you can start today, no class required: stand on one leg for 30 seconds while brushing your teeth (switch legs after rinsing). Walk heel-to-toe along a line for 10 steps. Stand up from a chair without using your hands, 10 times. Do these every day. If any of them feels scary, start near a countertop you can grab.
Whole-Body Vibration Platforms — Limited Evidence
Whole-body vibration (WBV) platforms — you stand on a plate that oscillates vertically at 20–50 Hz — have been marketed as a passive bone-building tool, particularly for frail older adults who cannot tolerate lifting or impact.
The evidence is genuinely mixed. Some trials in postmenopausal women show modest hip BMD gains over 6–12 months; others show nothing. A 2019 Cochrane-style review of over a dozen trials concluded that any effect is small, inconsistent, and smaller than what heavy resistance training delivers. The vibration frequency, amplitude, duration, and posture on the platform all influence results and have not been standardized across studies.
Honest bottom line: WBV is probably better than nothing if you truly cannot lift or jump — for example, severe osteoarthritis, recent fracture, cognitive impairment limiting gym use. It is not a substitute for loading if you are capable of loading. The $3,000–$8,000 consumer platforms are poorly regulated and often deliver less force than the research-grade machines used in positive trials. Save your money; spend it on a barbell, dumbbells, or a few months of supervised training.
Your Weekly Exercise Prescription
Synthesizing everything above, here is a defensible weekly template for a reader with osteopenia or osteoporosis, assuming no acute fractures and medical clearance to exercise:
Resistance training: 2–3 sessions per week. 30–45 minutes each. The core movements are compound, multi-joint, and loaded with enough weight that the last one or two reps of a set are genuinely hard. Target 3–5 sets of 5–8 repetitions once you are past a beginner phase. Build toward deadlifts, back squats (or goblet squats), overhead press, and bent-over rows. A trap-bar deadlift is a safer starting point than a conventional barbell deadlift because it keeps the load closer to the body's center of mass.
Impact work: 2 sessions per week. This can be appended to your resistance sessions. Start with low-amplitude hops — 10 small jumps, both feet, landing softly. Progress to drop landings (step off a 10–20 cm platform, land absorbing), multi-directional hops, and eventually short sprints or skipping if joints tolerate it. The target is roughly 50–100 impacts per session at forces above 3× body weight. Concentrate the impact on the hips — that is where fractures kill people.
Balance training: daily or near-daily. 5–10 minutes. Tai Chi class once or twice a week is a bonus. Daily single-leg stands, tandem walks, and chair stands are the minimum.
Aerobic / walking: most days. 30–45 minutes of brisk walking or similar. Not a bone builder on its own, but it supports weight control, cardiovascular health, mood, and the enjoyment factor that keeps you doing everything else.
Avoid: unsupervised spinal flexion, heavy loaded twists, deep forward folds, sit-ups and crunches, full yoga forward folds, and sudden unaccustomed high-impact activity. Avoid exercising through sharp back pain — a new vertebral fracture often presents exactly this way.
Consistency beats intensity. Two real sessions per week, sustained for a decade, will do more for your skeleton than a six-week boot-camp that leaves you injured and demoralized.
Post-Fracture Rehabilitation
If you are reading this shortly after a vertebral, hip, wrist, or pelvic fracture, the rules are different for the first several months. Tissue has to heal. Load has to be reintroduced gradually. But — and this is critical — the answer is not prolonged bed rest or indefinite exercise avoidance. Prolonged immobilization accelerates bone loss and dramatically raises your risk of the next fracture.
Typical timeline after a low-trauma vertebral compression fracture:
- Weeks 0–2. Pain control with short-course analgesics (acetaminophen, cautious NSAID use, sometimes calcitonin nasal spray). Gentle movement, walking as tolerated, avoiding forward bending and twisting. Vertebroplasty or kyphoplasty is considered only for severe, persistent pain — most fractures settle without it.
- Weeks 2–6. Physical therapy begins with extension-based spine stabilization (prone press-ups, small bird-dogs), hip-hinge retraining, and isometric core work. No flexion, no loaded lifting above body weight.
- Weeks 6–12. Gradual reintroduction of light resistance training. Bodyweight squats, wall push-ups, resistance band rows. Walking volume progresses.
- Months 3–6. Progressive loading restarts, ideally under supervision. A skilled physical therapist transitions you back toward the heavy compound lifts that your spine actually needs. Impact work is reintroduced last and carefully.
- Month 6 and beyond. You are back on a full program — heavy resistance, impact, balance — usually with pharmacological backup from a bisphosphonate, denosumab, or anabolic agent.
After a hip fracture the timeline is longer and surgical; after a wrist fracture it is shorter and largely limb-specific. In every case the principle is the same: return to loading as soon as tissue tolerates it, because the alternative — doing nothing — guarantees the next fracture.
Finding a Qualified Therapist — BoneFit and Beyond
Most physical therapists and personal trainers have almost no training specific to osteoporosis. Many will still tell a patient with a T-score of -3.0 not to lift anything heavier than a soup can. Others will happily demonstrate a sit-up. You need to screen your provider.
BoneFit (bonefit.ca) is a training program run by Osteoporosis Canada that certifies physical therapists, kinesiologists, and exercise physiologists in evidence-based osteoporosis exercise prescription. A BoneFit-trained clinician will know the LIFTMOR and Sinaki literature, will screen you for vertebral fractures before loading your spine, and will progress you toward heavy compound lifts rather than away from them. BoneFit providers are listed on the program's website; the directory is dominated by Canadian providers but is expanding.
Onero-certified providers (onero.com.au and spreading internationally) deliver the LIFTMOR protocol directly, most commonly in Australia and increasingly in the U.S.
In the U.S., the American Physical Therapy Association's Academy of Geriatric Physical Therapy offers a Certified Exercise Expert for Aging Adults (CEEAA) credential that is a reasonable proxy. Also ask any prospective provider these three questions:
- "How do you adapt resistance training for osteoporosis?" If they say "lighter weights and more reps," find someone else. The correct answer mentions progressive loading toward heavy compound lifts, with avoidance of spinal flexion.
- "Are you familiar with the LIFTMOR trial?" A provider who keeps up with the literature will say yes.
- "Do you screen for vertebral fractures before starting a loading program?" The right answer involves reviewing imaging, asking about sudden height loss, and doing a physical exam for kyphotic posture.
Expect to pay $80–$200 per session in the U.S. for a specialized provider. Many insurance plans cover 8–30 sessions per year when prescribed by a physician; group programs are cheaper per session and often equally effective.
Getting Started Safely If You're New to Lifting
If you have never lifted a barbell and the prospect is intimidating, here is the path most safely taken:
- Get imaging first. A recent DEXA scan and, ideally, a spine X-ray or vertebral fracture assessment (VFA) to rule out existing silent vertebral fractures. You cannot plan a loading program around a spine you have not looked at.
- Get medical clearance. Especially if you have cardiac disease, uncontrolled blood pressure, or recent fractures.
- Hire a qualified trainer for 4–8 sessions. Learn the hip hinge, the squat pattern, the overhead press, and the row with light loads. This is the single highest-return investment you can make in your skeleton.
- Progress slowly. Add 2.5–5 pounds per session for the first few months, then slow down as weights get heavier. The LIFTMOR protocol built up to 80–85% of one-rep max gradually, over weeks, not on day one.
- Track your lifts. Write down the weight and reps. Bone adapts to progressive overload; the log tells you whether you are progressing.
- Re-scan at 18–24 months. DEXA changes slowly. Do not panic if your 6-month scan shows little change; statistical noise dominates at that timescale.
If you combine protein and calcium intake adequate for bone turnover, vitamin D sufficiency, fall-prevention training, and heavy progressive resistance plus impact — with pharmacological support layered on when indicated — you have assembled the most effective osteoporosis program currently possible. Exercise is the piece nobody can prescribe for you. Only you can do the sets.
Key Research Papers
Randomized exercise trials and systematic reviews establishing that heavy progressive resistance plus impact loading improves BMD in postmenopausal women and older men, plus the spinal-mechanics literature defining safe versus risky movement patterns after vertebral fracture.
- Watson SL, Weeks BK, Weis LJ, Harding AT, Horan SA, Beck BR. High-Intensity Resistance and Impact Training Improves Bone Mineral Density and Physical Function in Postmenopausal Women with Osteopenia and Osteoporosis: The LIFTMOR Randomized Controlled Trial. Journal of Bone and Mineral Research. 2018;33(2):211–220.
- Harding AT, Weeks BK, Lambert C, Watson SL, Weis LJ, Beck BR. A Comparison of Bone-Targeted Exercise Strategies to Reduce Fracture Risk in Middle-Aged and Older Men with Osteopenia and Osteoporosis: LIFTMOR-M Semi-Randomized Controlled Trial. Journal of Bone and Mineral Research. 2020;35(8):1404–1414.
- Beck BR, Daly RM, Singh MA, Taaffe DR. Exercise and Sports Science Australia (ESSA) Position Statement on Exercise Prescription for the Prevention and Management of Osteoporosis. Journal of Science and Medicine in Sport. 2017;20(5):438–445.
- Howe TE, Shea B, Dawson LJ, et al. Exercise for Preventing and Treating Osteoporosis in Postmenopausal Women. Cochrane Database of Systematic Reviews. 2011;7:CD000333.
- Sinaki M, Mikkelsen BA. Postmenopausal Spinal Osteoporosis: Flexion versus Extension Exercises. Archives of Physical Medicine and Rehabilitation. Search PubMed
- Sinaki M, Itoi E, Wahner HW, et al. Stronger Back Muscles Reduce the Incidence of Vertebral Fractures: A Prospective 10 Year Follow-Up of Postmenopausal Women. Bone. 2002;30(6):836–841.
- Kemmler W, Shöjaa M, Kohl M, von Stengel S. Effects of Different Types of Exercise on Bone Mineral Density in Postmenopausal Women: A Systematic Review and Meta-Analysis. Calcified Tissue International. 2020;107(5):409–439.
- Sherrington C, Fairhall NJ, Wallbank GK, et al. Exercise for Preventing Falls in Older People Living in the Community. Cochrane Database of Systematic Reviews. 2019;1(1):CD012424.
- Liu-Ambrose T, Davis JC, Best JR, et al. Effect of a Home-Based Exercise Program on Subsequent Falls Among Community-Dwelling High-Risk Older Adults: A Randomized Clinical Trial. JAMA. 2019;321(21):2092–2100.
- Robling AG, Castillo AB, Turner CH. Biomechanical and Molecular Regulation of Bone Remodeling. Annual Review of Biomedical Engineering. 2006;8:455–498.
- Robling AG, Niziolek PJ, Baldridge LA, et al. Mechanical Stimulation of Bone in vivo Reduces Osteocyte Expression of Sost/Sclerostin. Journal of Biological Chemistry. 2008;283(9):5866–5875.
- Cosman F, de Beur SJ, LeBoff MS, et al. Clinician's Guide to Prevention and Treatment of Osteoporosis. Osteoporosis International. 2014;25(10):2359–2381.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: LIFTMOR resistance training
- PubMed: Wolff's law and osteocytes
- PubMed: postmenopausal exercise trials
- PubMed: spinal flexion and vertebral fracture
- PubMed: Tai Chi falls prevention
- PubMed: Otago exercise program
- PubMed: whole-body vibration and BMD
- PubMed: impact exercise and hip BMD
- PubMed: vertebral fracture rehabilitation
- PubMed: cycling athletes and BMD
Connections
- Bone Remodeling & Calcium Balance — interactive animation
- Osteoporosis
- Bisphosphonates
- Denosumab, Romosozumab and Teriparatide
- DEXA Scan: T-Score and Z-Score
- FRAX Risk Assessment
- Secondary Osteoporosis Causes
- Fracture Prevention and Fall Risk
- Postmenopausal Osteoporosis and Hormone Therapy
- Calcium, Vitamin D and Protein Intake
- Arthritis
- Fibromyalgia
- Calcium
- Vitamin D3
- Magnesium
- Full Body MRI