Bisphosphonates — Alendronate, Risedronate, Zoledronate
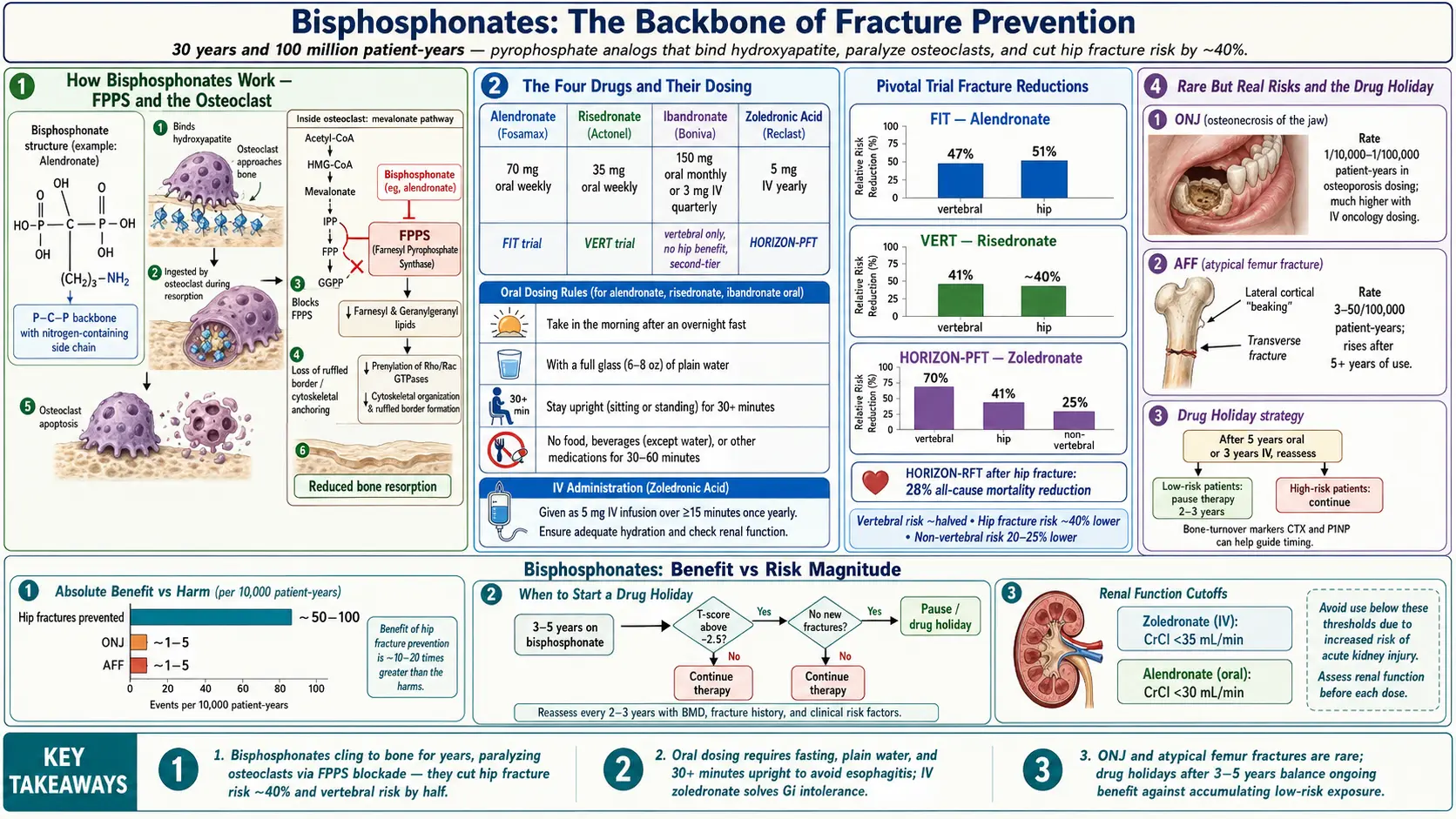
Table of Contents
- The Short Version
- How Bisphosphonates Work
- The Drugs in the Class
- The Pivotal Trials — What the Evidence Actually Shows
- Who Should Take a Bisphosphonate
- Oral Dosing Rules — Why They Matter
- IV Zoledronic Acid — What to Expect
- GI Side Effects — Alendronate and Risedronate
- Acute-Phase Reaction with IV Dosing
- Osteonecrosis of the Jaw (ONJ)
- Atypical Femur Fracture (AFF)
- The Drug Holiday — When to Stop and Restart
- Renal Dosing and Hypocalcemia
- Cost, Coverage, and Practical Logistics
- Questions Worth Asking Your Doctor
- Key Research Papers
- Connections
- Featured Videos
The Short Version
Bisphosphonates are the most prescribed, most studied, and cheapest class of osteoporosis drugs in the world. They have been on the market since 1995 (alendronate was the first), and more than a hundred million patient-years of follow-up now sit behind them. Used correctly, they cut the risk of a spine fracture roughly in half and the risk of a hip fracture by about 40%. They cost pennies a day as generics. They are the backbone of fracture prevention for most postmenopausal women and older men with osteoporosis.
They are also the drug class patients are most afraid of — because of two rare but real complications (jaw osteonecrosis, atypical femur fracture) that get splashed across news headlines whenever a lawsuit is filed. The goal of this page is to put the numbers side by side: the fractures these drugs prevent versus the complications they can cause, the dosing rules that separate patients who tolerate them from patients who hate them, and the strategy — called a "drug holiday" — that modern specialists use to capture the benefit without stacking up the long-term risk.
How Bisphosphonates Work
Your skeleton is not static. Specialized cells called osteoclasts chew away old bone. Other cells called osteoblasts lay down new bone in the crater behind them. In a healthy adult, the two crews are roughly balanced. After menopause (when estrogen drops) or with aging, the osteoclasts get louder and the osteoblasts fall behind. Bone mass drops roughly 1–2% a year. Given enough time, a spine vertebra or a hip neck becomes thin enough that a modest fall — or just bending to pick up a grocery bag — cracks it.
Bisphosphonates interrupt the osteoclast side of that equation. Structurally they are chemical cousins of pyrophosphate, a naturally occurring molecule that latches onto the hydroxyapatite mineral crystals that form bone. Because of that affinity, a bisphosphonate swallowed or infused today will cling to the inside surface of your bones for years. When an osteoclast arrives to dissolve that patch of bone, it swallows the drug along with the mineral.
Inside the osteoclast, the nitrogen-containing bisphosphonates (alendronate, risedronate, ibandronate, zoledronate) block an enzyme called farnesyl pyrophosphate synthase (FPPS). FPPS sits in the mevalonate pathway — the same pathway that statins interrupt higher up. Blocking it starves the osteoclast of the geranylgeranyl and farnesyl lipids it needs to anchor its cell-internal scaffolding (the "ruffled border" that dissolves bone, and small GTPase signaling proteins like Rho and Rac). Without those anchors, the osteoclast cannot do its job. It becomes functionally paralyzed and eventually dies by apoptosis.
The net effect: bone resorption slows dramatically, formation catches up, and measured bone density rises 4–8% over three years at the spine. More importantly, the fracture risk falls within the first 6–12 months of treatment — faster than you might expect given how slowly density changes — because the drug also seems to repair the microarchitecture and reduce the kind of microscopic stress cracks that precede a full fracture.
The Drugs in the Class
Four bisphosphonates are FDA-approved for osteoporosis. A fifth (pamidronate) is used for Paget's disease and cancer-related bone problems but not first-line osteoporosis.
- Alendronate (Fosamax). Oral tablet, 70 mg once weekly. The most prescribed osteoporosis drug in the world. Generic, usually $4–$15 a month. Pivotal trial: FIT.
- Risedronate (Actonel, Atelvia). Oral tablet, 35 mg once weekly (also 150 mg monthly, and a delayed-release "Atelvia" version that can be taken with food). Generic. Slightly easier on the stomach than alendronate for some patients. Pivotal trial: VERT.
- Ibandronate (Boniva). Oral 150 mg monthly or IV 3 mg every 3 months. Convenient dosing, but the evidence base is weaker: ibandronate clearly reduces vertebral fractures but has never convincingly shown a hip-fracture benefit. Many specialists consider it a second-tier choice.
- Zoledronic acid (Reclast; Zometa in oncology dosing). IV infusion, 5 mg once yearly over 15–30 minutes. The most potent of the four, and the only option if you cannot tolerate oral dosing or have chronic GI disease. Pivotal trial: HORIZON-PFT.
For most new patients, the practical choice is between oral alendronate or risedronate (cheap, self-administered) and IV zoledronate (annual infusion, supervised). There is no good head-to-head evidence that one is meaningfully more effective than the others at preventing fractures — the choice comes down to tolerance, convenience, and cost.
The Pivotal Trials — What the Evidence Actually Shows
Three randomized controlled trials established the modern fracture-prevention numbers that every later guideline is built on.
FIT — Alendronate
The Fracture Intervention Trial (Black et al., 1996 and Cummings et al., 1998) randomized about 6,500 postmenopausal women with low femoral-neck bone density to alendronate or placebo for three to four years. In the arm with established vertebral fractures at baseline, alendronate cut the risk of a new vertebral fracture by 47% and cut hip fractures by 51%. In the arm without prior vertebral fractures, vertebral fractures fell by about 44% but the absolute numbers were small.
VERT — Risedronate
The Vertebral Efficacy with Risedronate Therapy trials (Harris et al., 1999; Reginster et al., 2000) randomized roughly 2,500 women with at least one prior vertebral fracture. Over three years, risedronate reduced new vertebral fractures by 41% and non-vertebral fractures by about 39%. A separate hip-fracture trial (HIP, McClung 2001) showed about a 40% hip-fracture reduction in women selected for low hip bone density.
HORIZON-PFT — Zoledronic Acid
The Health Outcomes and Reduced Incidence with Zoledronic Acid Once Yearly Pivotal Fracture Trial (Black et al., N Engl J Med, 2007) randomized 7,765 postmenopausal women with osteoporosis to a single 5 mg annual infusion versus placebo for three years. Vertebral fractures fell by 70%, hip fractures by 41%, and all non-vertebral fractures by 25%. A companion trial (HORIZON-RFT, Lyles et al., 2007) in patients who had just had a hip fracture repaired showed a 35% reduction in new clinical fractures and a 28% reduction in all-cause mortality — the only osteoporosis trial to show a clear survival benefit.
The headline numbers to keep in mind: bisphosphonates cut vertebral fracture risk roughly in half, hip fracture risk by about 40%, and non-vertebral fracture risk by about 20–25%. That is a big effect size for a cheap generic medicine.
Who Should Take a Bisphosphonate
Current U.S. guidelines (American College of Physicians, Endocrine Society, Bone Health & Osteoporosis Foundation) recommend starting a bisphosphonate in any of the following:
- A DEXA T-score of −2.5 or lower at the spine, total hip, or femoral neck.
- A history of a fragility fracture (hip or vertebra) regardless of T-score.
- A T-score between −1.0 and −2.5 (osteopenia) plus a FRAX 10-year major-fracture risk of 20% or higher, or a 10-year hip-fracture risk of 3% or higher. See the FRAX article for how to run your own numbers.
- Certain high-risk situations regardless of baseline T-score: long-term glucocorticoid therapy (prednisone 7.5 mg/day or more for three months or longer), aromatase-inhibitor treatment for breast cancer, androgen-deprivation therapy for prostate cancer.
Before starting, your clinician should check calcium, 25-OH vitamin D, creatinine (kidney function), and ideally TSH and a celiac screen to catch common secondary causes of bone loss. A baseline DEXA scan is required for tracking.
Oral Dosing Rules — Why They Matter
Oral bisphosphonates are notoriously poorly absorbed. Less than 1% of a swallowed dose ever makes it into the bloodstream, and any food, coffee, tea, mineral water, calcium, iron, or juice taken nearby will knock absorption to essentially zero. The standard rules exist for exactly that reason:
- First thing in the morning, on an empty stomach. No food, no coffee, no vitamin, no other pill for at least an hour beforehand.
- Swallow the tablet whole with a full 6–8 oz glass of plain tap water. Not bottled mineral water (the dissolved calcium and magnesium bind the drug). Not coffee, tea, or juice.
- Stay fully upright — sitting, standing, or walking — for at least 30 minutes. Do not lie down. Do not stretch out on the couch.
- Wait 30 minutes (60 for ibandronate) before eating, drinking anything else, or taking other medicines.
Why so strict? Bisphosphonates are caustic to the lining of the esophagus. If a tablet sticks on the way down — which happens disturbingly often when people take it with a sip of water and lie back in bed — it can cause a chemical burn, an ulcer, or in rare cases an esophageal stricture. The 30-minute upright rule gives the tablet time to clear into the stomach, where the acidic environment neutralizes the contact risk.
Practical trick: pick a fixed weekly day and tie it to a ritual you already do. Saturday morning, drink your water, set a kitchen timer for 30 minutes, then go make coffee. Patients who skip the rules almost always end up with either bad heartburn (and quit the drug) or no benefit (because they took it with coffee and never absorbed it).
IV Zoledronic Acid — What to Expect
Zoledronate bypasses the stomach entirely. The infusion is a once-a-year event, usually done in a rheumatologist's or oncologist's office, a hospital infusion suite, or — increasingly — the Medicare-covered "Reclast in the primary care office" workflow. Total chair time is about 45 minutes: IV line placement, 15–30 minutes of drip, a brief observation period, and out.
Before the first infusion, you should:
- Drink an extra 2–3 glasses of water the day before and the day of the infusion (prevents kidney stress).
- Have normal calcium and vitamin D levels. A 25-OH vitamin D below 30 ng/mL should be corrected first.
- Take 1,000 mg of acetaminophen (Tylenol) 60 minutes before the infusion — this cuts the acute-phase reaction (see below) by about half.
- Complete any planned dental work, especially extractions or implants, before starting.
Zoledronate is the go-to if you cannot tolerate oral dosing, have severe reflux or a history of esophageal disease, have problems with adherence (skipping doses), or simply prefer "once a year and done." Efficacy is at least as good as oral alendronate — arguably better for vertebral fracture reduction.
GI Side Effects — Alendronate and Risedronate
The most common reason people abandon oral bisphosphonates is upper-GI irritation: heartburn, acid regurgitation, mid-chest burning after swallowing the pill, nausea, or a vague dull discomfort behind the breastbone. Real population-based studies put the incidence of meaningful GI symptoms around 10–20% in the first year, though in randomized trials the rate is much closer to placebo because enrollees were pre-screened for pill tolerance.
Strategies that help:
- Double-check that you are following all four dosing rules.
- Try delayed-release risedronate (Atelvia), which is designed to bypass the esophagus and release in the small intestine; it can be taken immediately after breakfast.
- Switch from alendronate to regular risedronate — some patients tolerate one and not the other despite identical mechanism.
- If symptoms persist, switch to IV zoledronate.
Serious esophagitis, esophageal ulcer, or stricture happens in fewer than 1 in 1,000 treated patients, almost always in people who did not follow the dosing rules or who had pre-existing reflux or esophageal motility problems. A history of Barrett's esophagus or achalasia is a contraindication to oral bisphosphonates.
Acute-Phase Reaction with IV Dosing
About one in three first-time zoledronate recipients develops what feels like a 24-to-72-hour flu: low-grade fever, muscle aches, bone aches (sometimes quite severe), headache, fatigue. This is the acute-phase reaction and it is a real pharmacological effect, not an allergy. Nitrogen-containing bisphosphonates trigger a burst of interleukin-6 and gamma-delta T-cell activation — the same inflammatory signaling that makes a flu infection feel terrible.
The reaction is much milder on second and subsequent annual infusions, usually resolves on its own within three days, and can be blunted by:
- Pre-infusion acetaminophen (1,000 mg) an hour before, then every 6 hours for 48–72 hours as needed.
- Plenty of fluids.
- Planning the infusion for a Thursday or Friday so the flu-like days fall on the weekend.
A handful of patients have an acute-phase reaction bad enough that they refuse a second infusion. For those patients, switching to oral alendronate or to denosumab (see the denosumab article) is reasonable.
Osteonecrosis of the Jaw (ONJ)
ONJ is the complication patients fear most because of the lawsuit advertising. Here are the honest numbers.
ONJ is a patch of exposed jaw bone that will not heal, usually in the lower jaw, usually after a tooth extraction or implant placement. In cancer patients receiving high-dose monthly IV bisphosphonates (zometa, zoledronate at 4 mg every 3–4 weeks for bone metastases), the incidence is roughly 1–10%. In osteoporosis patients on standard doses (weekly oral or yearly IV), the incidence is orders of magnitude lower: most studies put it between 1 in 10,000 and 1 in 100,000 patient-years.
To put that in context: your lifetime risk of a hip fracture after age 65 without treatment is roughly 1 in 6 for a woman and 1 in 20 for a man. Hip fractures kill about 20% of people who sustain them within a year. The math almost always favors taking the drug.
Sensible precautions:
- See your dentist before starting a bisphosphonate. Get any extractions, implants, periodontal surgery, or deep cleaning done first.
- Maintain excellent oral hygiene — brushing twice daily, flossing, twice-yearly cleanings.
- If you need a tooth extraction while on therapy, tell the dentist and oral surgeon. Most will proceed — routine extractions on osteoporosis-dose bisphosphonate patients almost always heal normally. Some will ask for a short drug hold around the procedure, though the evidence that this helps is thin.
- Report any exposed bone, non-healing socket, or unexplained jaw pain to your dentist and prescribing clinician.
Atypical Femur Fracture (AFF)
AFF is a transverse or short-oblique fracture of the femoral shaft (the middle of the thighbone), not the usual hip-neck spot. It is distinct from ordinary hip fractures: it is almost always preceded by weeks or months of a dull, aching pain in the thigh or groin, often bilateral, worse with weight-bearing. On X-ray there is a characteristic thickening of the lateral femoral cortex (the outside edge of the bone) called "beaking."
Baseline risk without any treatment is roughly 1 per 100,000 per year. With bisphosphonate treatment the risk climbs with duration of exposure: about 1.8 per 100,000 at 2 years, rising to 113 per 100,000 after 8–10 years of continuous treatment. The absolute risk is still small, but the curve bends sharply upward after roughly the 5-year mark. That single fact is what drives the modern "drug holiday" strategy.
If you develop new thigh or groin pain while on a bisphosphonate, take it seriously. Ask for a femur X-ray (or, for better sensitivity, a bilateral femur MRI). Catching a stress reaction before it propagates into a completed fracture is the whole point of surveillance.
The Drug Holiday — When to Stop and Restart
Because bisphosphonate molecules persist in bone for years after the last dose, the anti-fracture effect does not simply vanish when you stop the drug. Modern practice takes advantage of that residual effect to cap total exposure and reduce the long-term AFF and ONJ risk.
The rough algorithm (based on ASBMR 2016 guidance and American College of Physicians 2023 update):
- Reassess at 5 years for oral bisphosphonates (alendronate, risedronate), or at 3 years for IV zoledronate.
- At that point, check DEXA, run FRAX, and review fracture history.
- Low to moderate risk (T-score above −2.5, no new fractures on treatment, FRAX below intervention thresholds): stop for 2–5 years, rescan every 1–2 years, and restart if bone density drops or a fracture occurs.
- High risk (T-score still −2.5 or lower, prior hip or vertebral fracture, ongoing glucocorticoids, or new fractures on therapy): continue for up to 10 years oral or 6 years IV, then reassess. Some of these patients will be switched to a different class (denosumab, teriparatide, or romosozumab) rather than held on bisphosphonates indefinitely.
A drug holiday is not permanent. The AFF risk falls back toward baseline within about a year of stopping, but fracture-prevention benefit also fades over 2–5 years. Your clinician is balancing those two curves. The worst outcome is patients who "just stop" on their own and never get rescanned, then show up five years later with a new vertebral fracture.
Renal Dosing and Hypocalcemia
Bisphosphonates are cleared by the kidneys. When kidney function falls, the drug sticks around longer and its effect on bone and on blood calcium intensifies. Standard cutoffs:
- eGFR above 35 mL/min/1.73m²: full dose of any bisphosphonate.
- eGFR 30–35: zoledronate is generally avoided; oral bisphosphonates can still be used but with caution.
- eGFR below 30: avoid bisphosphonates. Denosumab is the usual alternative since it is cleared by the reticuloendothelial system rather than the kidney — but it carries its own hypocalcemia risk in advanced CKD and should be supervised by a nephrologist.
Before any bisphosphonate dose, your serum calcium and 25-OH vitamin D must be in range. Treating a hypocalcemic patient with a bisphosphonate can drop the calcium further into a symptomatic range (tingling, cramps, tetany, seizures). The standard pre-treatment baseline is calcium 8.5–10.2 mg/dL and 25-OH vitamin D of at least 30 ng/mL. While on therapy, aim for 1,200 mg of calcium and 800–1,000 IU of vitamin D daily, mostly through food when possible. See the calcium and vitamin D article for food sources and supplement strategy, or the calcium mineral page for background.
Cost, Coverage, and Practical Logistics
Generic alendronate and risedronate are on every major $4-a-month big-box pharmacy list (Walmart, Costco, Kroger). With GoodRx or similar discount cards, they are frequently under $10 for a 90-day supply even without insurance.
Zoledronate infusion is covered under Medicare Part B (not Part D) as a physician-administered drug. Total charge to the patient after Medicare is typically $0–$150 depending on supplemental coverage. Commercial insurance usually covers it with prior authorization, which your prescriber's office handles.
Two logistic traps to avoid: (1) Make sure your lab work (calcium, vitamin D, creatinine) is recent — within 3 months for IV dosing — before the infusion is scheduled, or the infusion center will cancel you at the door. (2) Schedule your yearly zoledronate at the same time each year (e.g., every November) and put it on the calendar; missed-infusion lapses are a common reason for breakthrough fractures.
Questions Worth Asking Your Doctor
- What is my 10-year FRAX-estimated fracture risk, and what would it be on treatment?
- Have we checked for secondary causes of osteoporosis (celiac, hyperparathyroidism, low testosterone, multiple myeloma) before committing to long-term bisphosphonate therapy?
- Is my vitamin D level at least 30 ng/mL?
- Oral versus IV — given my GI history and ability to follow the dosing rules, which makes more sense?
- When should we plan a drug holiday, and what will trigger restarting?
- Do I need a pre-treatment dental visit, and do I have any planned oral surgery that should happen first?
- If I develop new thigh or groin pain, what is the plan to check for a stress reaction?
Key Research Papers
Pivotal randomized fracture trials (FIT, VERT, HORIZON-PFT, HORIZON-RFT), the FLEX long-term extension that informs drug-holiday decisions, and ASBMR / ACP / Endocrine Society task-force statements on atypical femur fractures, osteonecrosis of the jaw, and treatment duration.
- Black DM, Cummings SR, Karpf DB, et al. Randomised Trial of Effect of Alendronate on Risk of Fracture in Women with Existing Vertebral Fractures (Fracture Intervention Trial). Lancet. 1996;348(9041):1535–1541.
- Cummings SR, Black DM, Thompson DE, et al. Effect of Alendronate on Risk of Fracture in Women with Low Bone Density but without Vertebral Fractures (FIT II). JAMA. 1998;280(24):2077–2082.
- Harris ST, Watts NB, Genant HK, et al. Effects of Risedronate Treatment on Vertebral and Nonvertebral Fractures in Women with Postmenopausal Osteoporosis (VERT-NA). JAMA. 1999;282(14):1344–1352.
- Black DM, Delmas PD, Eastell R, et al. Once-Yearly Zoledronic Acid for Treatment of Postmenopausal Osteoporosis (HORIZON-PFT). New England Journal of Medicine. 2007;356(18):1809–1822.
- Lyles KW, Colón-Emeric CS, Magaziner JS, et al. Zoledronic Acid and Clinical Fractures and Mortality After Hip Fracture (HORIZON-RFT). New England Journal of Medicine. 2007;357(18):1799–1809.
- Black DM, Schwartz AV, Ensrud KE, et al. Effects of Continuing or Stopping Alendronate After 5 Years of Treatment: The Fracture Intervention Trial Long-term Extension (FLEX). JAMA. 2006;296(24):2927–2938.
- Black DM, Reid IR, Boonen S, et al. The Effect of 3 Versus 6 Years of Zoledronic Acid Treatment of Osteoporosis: A Randomized Extension to the HORIZON-Pivotal Fracture Trial. Journal of Bone and Mineral Research. 2012;27(2):243–254.
- Adler RA, El-Hajj Fuleihan G, Bauer DC, et al. Managing Osteoporosis in Patients on Long-Term Bisphosphonate Treatment: Report of a Task Force of the American Society for Bone and Mineral Research. Journal of Bone and Mineral Research. 2016;31(1):16–35.
- Shane E, Burr D, Abrahamsen B, et al. Atypical Subtrochanteric and Diaphyseal Femoral Fractures: Second Report of a Task Force of the American Society for Bone and Mineral Research. Journal of Bone and Mineral Research. 2014;29(1):1–23.
- Khan AA, Morrison A, Hanley DA, et al. Diagnosis and Management of Osteonecrosis of the Jaw: A Systematic Review and International Consensus. Journal of Bone and Mineral Research. 2015;30(1):3–23.
- Qaseem A, Hicks LA, Etxeandia-Ikobaltzeta I, et al. Pharmacologic Treatment of Primary Osteoporosis or Low Bone Mass to Prevent Fractures in Adults: A Living Clinical Guideline From the American College of Physicians. Annals of Internal Medicine. 2023;176(2):224–238.
- Eastell R, Rosen CJ, Black DM, Cheung AM, Murad MH, Shoback D. Pharmacological Management of Osteoporosis in Postmenopausal Women: An Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology & Metabolism. 2019;104(5):1595–1622.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: alendronate fracture prevention
- PubMed: risedronate VERT trials
- PubMed: zoledronic acid HORIZON
- PubMed: bisphosphonates and ONJ
- PubMed: atypical femur fractures
- PubMed: bisphosphonate drug holiday
- PubMed: bisphosphonates and renal function
- PubMed: FPP synthase and osteoclasts
Connections
- Bone Remodeling & Calcium Balance — interactive animation
- Calcium
- Osteoporosis
- DEXA Scan: T-Score and Z-Score
- Denosumab, Romosozumab and Teriparatide
- Calcium, Vitamin D and Protein Intake
- FRAX Risk Assessment
- Secondary Osteoporosis Causes
- Weight-Bearing and Resistance Exercise
- Fracture Prevention and Fall Risk
- Postmenopausal Osteoporosis and Hormone Therapy
- Vitamin D3
- Vitamin K
- Magnesium
- Arthritis
- eGFR
- Hyperparathyroidism
- Bone Loss Prevention and HRT
- Vitamin K2 and Bone Health