Calcium, Vitamin D, and Protein Intake for Bone Health
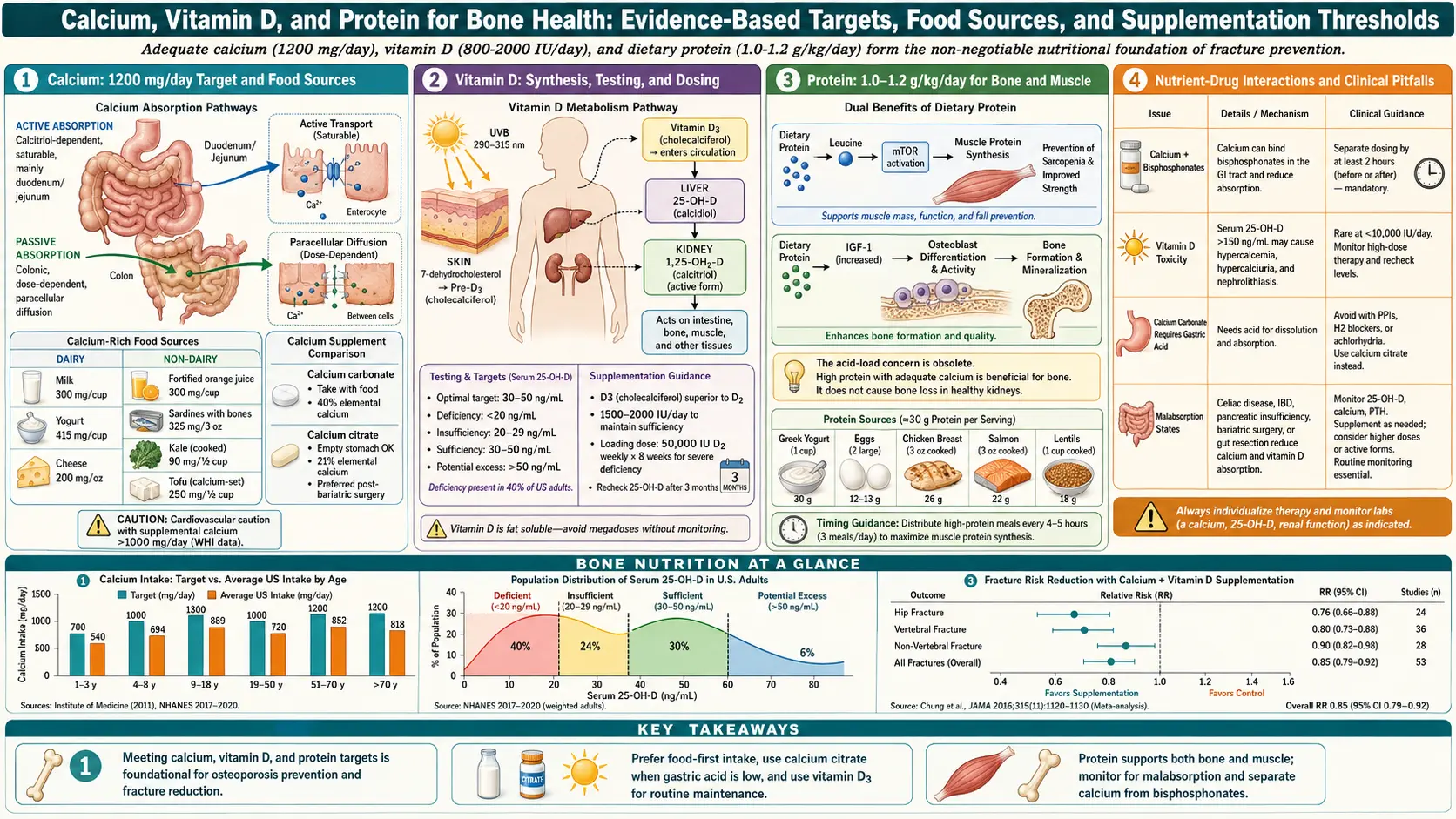
Table of Contents
- Why These Three Nutrients Matter Together
- Calcium — Daily Targets and Why the Number Changes With Age
- Food-First Calcium: Where It Actually Lives
- Calcium Supplements: Carbonate vs. Citrate
- The Calcium Supplement Cardiovascular Debate
- Vitamin D — The 25(OH)D Target
- D3 vs. D2, Dosing, and Loading Protocols
- VITAL and D-Health — What the Mega-Trials Actually Showed
- Protein — Older Adults Need More Than the RDA
- Leucine, Meal Distribution, and Anabolic Resistance
- Supporting Cofactors: Magnesium, K2, Boron, Zinc
- Timing Around Bisphosphonates and Other Medications
- A Sample Bone-Friendly Day
- Common Mistakes
- Key Research Papers
- Connections
- Featured Videos
Why These Three Nutrients Matter Together
Your skeleton is not inert. It is a living organ that rebuilds itself constantly — roughly 10% of your bone mass is replaced every year. Old bone is dissolved by osteoclasts, and new bone is laid down by osteoblasts. For that turnover to keep pace (and, before age 30, to build a peak bone mass that will carry you for the rest of your life), three nutrients must all be available at the same time:
- Calcium is the mineral that gets deposited into the protein scaffold of bone. Without it, the scaffold is just soft tissue.
- Vitamin D is the hormone that tells your gut to absorb calcium in the first place. Without adequate vitamin D, you can eat 1,500 mg of calcium a day and still run a deficit.
- Protein provides the amino-acid raw material (primarily type I collagen) that forms 90% of bone matrix by volume. Calcium is the plaster; protein is the rebar.
Focus on any one of these in isolation and you miss the point. A postmenopausal woman chugging calcium chews with a 25(OH)D of 18 ng/mL and a 0.7 g/kg protein intake is doing almost nothing for her skeleton. Get all three dialed in, layer in weight-bearing exercise (see the exercise page), and you create the conditions under which bone can actually remodel in your favor — or, if you are on a drug like alendronate or denosumab, under which that drug can do its job (see bisphosphonates and denosumab/romosozumab/teriparatide).
Calcium — Daily Targets and Why the Number Changes With Age
The U.S. National Academies (formerly the Institute of Medicine) set the Recommended Dietary Allowances (RDAs) for calcium based on the intake needed to maintain calcium balance and support bone health. The targets are not one-size-fits-all:
- Adults 19–50: 1,000 mg/day (both sexes).
- Women 51 and older: 1,200 mg/day.
- Men 51–70: 1,000 mg/day.
- Men 71 and older: 1,200 mg/day.
- Pregnant or lactating adults: 1,000 mg/day (1,300 mg for teenagers).
- Tolerable Upper Intake Level (UL): 2,500 mg/day for adults 19–50, and 2,000 mg/day for adults 51+.
The jump for women at 51 reflects the sharp drop in estrogen at menopause, which accelerates bone resorption and reduces the efficiency of intestinal calcium absorption. Men hit the same absorption-efficiency cliff later, around 70. In both cases, the body needs more dietary calcium to replace what the gut can no longer grab as efficiently.
One number that trips patients up: total intake means food plus supplements. If your diet already provides 900 mg of calcium, adding a 1,200 mg chewable on top is not a gentle extra — it pushes you past 2,000 mg and into the zone where cardiovascular and kidney-stone signals start to appear (more on that below).
Food-First Calcium: Where It Actually Lives
Every major bone-health guideline — from the National Osteoporosis Foundation (now Bone Health & Osteoporosis Foundation), to Endocrine Society, to the European Society for Clinical and Economic Aspects of Osteoporosis (ESCEO) — now recommends meeting calcium needs from food first, with supplements used only to close a gap. Food-derived calcium comes packaged with the protein, magnesium, and phosphorus the skeleton needs anyway, and it does not produce the sharp blood-calcium spikes that some researchers have linked to arterial calcification.
Reliable calcium sources by typical serving:
- Plain low-fat yogurt, 1 cup — 415 mg.
- Milk (cow, 1%), 1 cup — 305 mg.
- Fortified soy or almond milk, 1 cup — 300–450 mg (check the label; unfortified plant milks have almost none).
- Canned sardines with bones, 3 oz — 325 mg.
- Canned salmon with bones, 3 oz — 180 mg.
- Firm tofu set with calcium sulfate, ½ cup — 250–400 mg.
- Cheddar cheese, 1.5 oz — 305 mg.
- Cottage cheese, 1 cup — 140 mg.
- Collard greens, cooked, 1 cup — 270 mg.
- Kale, cooked, 1 cup — 180 mg.
- Bok choy, cooked, 1 cup — 160 mg.
- Calcium-fortified orange juice, 1 cup — 350 mg.
- White beans, cooked, 1 cup — 160 mg.
- Almonds, 1 oz (about 23) — 75 mg.
Spinach, rhubarb, and Swiss chard technically contain calcium but are heavy in oxalates that bind the mineral in the gut — absorption drops to about 5%, compared with roughly 30% for dairy and 50% for bok choy or kale. Don't count them.
The practical target for a patient doing food-first: three calcium-rich servings a day. A yogurt at breakfast (400 mg), a cup of fortified soy milk with lunch (300 mg), and a serving of sardines on toast or a tofu-and-greens stir-fry at dinner (400 mg) puts you at 1,100 mg without a single pill. See the Calcium mineral page for a full food-source reference.
Calcium Supplements: Carbonate vs. Citrate
If food alone can't close the gap, a supplement is reasonable — but the form and timing matter more than most patients realize.
Calcium carbonate is the cheapest and most concentrated form (40% elemental calcium by weight), which is why it dominates drugstore shelves as Tums, Caltrate, and Os-Cal. It requires stomach acid to dissolve, so it must be taken with food. Patients on proton-pump inhibitors (omeprazole, esomeprazole, pantoprazole) or H2 blockers absorb carbonate poorly and should switch forms.
Calcium citrate (Citracal) is 21% elemental calcium — you need bigger or more pills to match a carbonate dose — but it does not require acid and can be taken on an empty stomach. It is the right choice for anyone on acid-suppressing drugs, anyone with a history of kidney stones (citrate itself is a stone inhibitor), and anyone who simply finds carbonate constipating.
Practical rules regardless of form:
- Split doses. The gut absorbs calcium efficiently only up to about 500–600 mg at a time. A single 1,000 mg pill is largely wasted. Take 500 mg with breakfast and 500 mg with dinner.
- Read the label for elemental calcium. A "1,250 mg calcium carbonate" tablet provides 500 mg of elemental calcium. The elemental number is what counts toward your daily target.
- Don't overshoot. If your diet already gives you 700–900 mg, a single 500 mg supplement gets you to target. A second pill pushes you into the zone where cardiovascular signals have been raised.
- Calcium plus iron don't mix. Calcium blocks iron absorption. If you take an iron supplement, separate them by at least two hours.
The Calcium Supplement Cardiovascular Debate
Starting with a 2010 meta-analysis by Bolland and colleagues in BMJ, several observational datasets suggested that calcium supplements (but not dietary calcium) might increase the risk of myocardial infarction by around 25–30%. The signal has been controversial ever since — some subsequent analyses confirmed it, others did not, and the 2016 joint guideline from the National Osteoporosis Foundation and the American Society for Preventive Cardiology concluded that calcium intake from food or supplements up to the UL is likely safe for the cardiovascular system in generally healthy adults.
The most defensible patient-facing interpretation today:
- Food-source calcium appears cardiovascular-neutral or protective in every major analysis. Eat calcium-rich foods without worry.
- Supplements are safe when used to close a real dietary gap and kept at 500–600 mg/day or less.
- Doses of 1,000–1,500 mg/day from supplements alone, on top of a diet that already meets the RDA, are the real concern. That is the dose range where signals appear. Don't stack supplements on a calcium-rich diet "for insurance."
Vitamin D — The 25(OH)D Target
Vitamin D is the gatekeeper. Without adequate stores, your gut absorbs only 10–15% of dietary calcium; with adequate stores, it absorbs 30–40%. The lab test that actually matters is 25-hydroxyvitamin D, abbreviated 25(OH)D — the storage form, measured in ng/mL in the U.S. or nmol/L elsewhere (multiply ng/mL by 2.5 for nmol/L).
Target ranges remain debated, but the ranges most bone-health specialists use:
- <20 ng/mL: frank deficiency. Associated with rickets in children, osteomalacia in adults, and accelerated bone loss. Treatment required.
- 20–29 ng/mL: insufficiency for bone health in most older adults. Many endocrinologists treat this range aggressively in osteoporosis patients.
- 30–50 ng/mL: the practical target range for patients with osteoporosis or on antiresorptive therapy. This is where calcium absorption is maximized and PTH is fully suppressed.
- >50–60 ng/mL: no added bone benefit, possible cardiovascular signal in some cohorts. No reason to push higher.
- >100 ng/mL: toxicity risk (hypercalcemia, kidney stones). Stop supplementation and retest.
The Endocrine Society's 2011 clinical practice guideline set a goal of >30 ng/mL for at-risk patients and remains the most widely cited reference. The 2024 update loosened some of the broad-population recommendations but kept the 30 ng/mL target for patients with osteoporosis.
D3 vs. D2, Dosing, and Loading Protocols
D3 (cholecalciferol) and D2 (ergocalciferol) both raise 25(OH)D, but D3 raises it further per IU and sustains the level longer. D3 is made by your skin in sunlight and found in animal-source foods (fatty fish, egg yolks). D2 is made by yeast and mushrooms exposed to UV, and it is the form most commonly written on prescription pads in the U.S. (the old 50,000 IU weekly capsules). For most patients, an over-the-counter D3 capsule or softgel is both cheaper and more effective than prescription D2. See the Vitamin D3 page for form details.
Typical dosing:
- Maintenance for adults with adequate baseline (25(OH)D >30): 1,000–2,000 IU/day of D3.
- Repletion for deficiency (25(OH)D <20): 50,000 IU D3 weekly for 6–8 weeks, then drop to a 2,000–4,000 IU/day maintenance dose. Recheck 25(OH)D 3 months after starting maintenance.
- Patients with malabsorption (celiac, Crohn's, post-bariatric surgery): often need 5,000–10,000 IU/day to maintain a target level. Dose is individualized by retesting.
- Obese patients (BMI >30): vitamin D sequesters in fat tissue. Expect to need roughly 1.5× the dose of a lean person to achieve the same serum level.
- Tolerable Upper Intake Level: 4,000 IU/day for adults, per the National Academies. Higher doses are safe under physician supervision with monitoring, but self-dosing above 4,000 IU/day without lab checks is not advised.
Take vitamin D with the largest fat-containing meal of the day — absorption roughly doubles compared with fasting or a low-fat meal.
VITAL and D-Health — What the Mega-Trials Actually Showed
Two enormous randomized trials reshaped how bone specialists talk about vitamin D in the last five years, and their results are often mis-summarized in the lay press.
VITAL (2018–2022) randomized 25,871 U.S. adults to 2,000 IU/day of vitamin D3 (with or without omega-3s) versus placebo for a median of 5.3 years. The headline: vitamin D did not reduce total fractures, hip fractures, or non-vertebral fractures in the overall, generally-healthy population. Critics noted that most participants entered the trial already vitamin-D-replete (mean baseline 25(OH)D ~31 ng/mL), so the study was underpowered to detect a benefit in deficient patients. VITAL did not test vitamin D plus calcium in osteoporosis patients; it tested vitamin D alone in a generally healthy cohort.
D-Health (2023) randomized 21,315 Australian adults aged 60–84 to 60,000 IU/month of vitamin D3 versus placebo for 5 years. Again, no reduction in total fractures. Again, most participants started with adequate vitamin D levels.
What this actually means for the patient in front of you:
- Vitamin D alone, without calcium, probably does little for fracture risk in already-replete adults. That is what the trials tested, and that is what they found.
- Vitamin D plus calcium, together, does reduce hip and non-vertebral fractures in institutionalized older adults and in people who are actually deficient — Weaver 2016 (NOF-sponsored meta-analysis) and Chapuy's landmark 1992 French nursing-home trial remain the foundations of that recommendation.
- Pairing is the point. Treating an osteoporosis patient with calcium without vitamin D, or vitamin D without checking that calcium intake is adequate, misses the mechanism.
Protein — Older Adults Need More Than the RDA
The U.S. RDA for protein is 0.8 g per kilogram of body weight per day, set in 1989 and anchored on nitrogen-balance studies in young adults. That number is almost certainly wrong for older adults, and it is the most underappreciated lever in bone health.
The PROT-AGE consensus (Bauer 2013, JAMDA), jointly issued by the European Union Geriatric Medicine Society, the International Association of Gerontology and Geriatrics, and the European Society for Clinical Nutrition and Metabolism, recommends:
- Healthy adults over 65: 1.0–1.2 g/kg/day of protein.
- Older adults with acute or chronic illness: 1.2–1.5 g/kg/day.
- Older adults with severe illness, injury, or malnutrition: up to 2.0 g/kg/day.
For a 70-kg (154-lb) older woman, that is 70–84 g of protein a day, minimum — roughly double what many actually eat. For a 90-kg (198-lb) older man, it is 90–108 g.
Why this matters for bone specifically: protein provides the collagen matrix itself, it raises circulating IGF-1 (a key anabolic signal for osteoblasts), it is required for muscle maintenance (and a stronger muscle pulls harder on bone, stimulating remodeling), and it reduces fall risk by preserving lean mass and grip strength. The old fear that "high protein leaches calcium from bone" has been thoroughly debunked — the modest acid load from dietary protein is buffered by kidney excretion, not bone dissolution, and higher-protein diets consistently associate with better bone density and lower hip-fracture risk in older adults, provided calcium intake is adequate.
Leucine, Meal Distribution, and Anabolic Resistance
Older muscle is less responsive to a given dose of protein — a phenomenon called anabolic resistance. To trigger maximal muscle protein synthesis, an older adult needs roughly 25–30 g of high-quality protein per meal, containing about 2.5–3 g of the amino acid leucine. Smaller doses simply do not cross the threshold.
The practical implication is counter to the typical Western eating pattern, which is protein-light at breakfast (toast and coffee), protein-light at lunch (salad or sandwich), and protein-heavy at dinner (a large steak or chicken breast). That one big dinner hits the anabolic threshold once; the rest of the day wastes the opportunity.
Distribute protein across three or four meals, hitting 25–30 g each time:
- Breakfast (30 g): 1 cup Greek yogurt (17 g) + 2 eggs (12 g).
- Lunch (30 g): 4 oz canned tuna or salmon (28 g) on whole-grain bread, or a lentil-and-bean bowl with feta.
- Dinner (30 g): 4 oz chicken, fish, tofu, or lean beef with a calcium-rich vegetable side.
- Snack/evening (15–20 g): cottage cheese, a whey shake, or a hard-boiled egg with cheese.
Leucine-dense sources include whey protein (the highest leucine density of any natural food), milk, yogurt, eggs, fish, and poultry. Plant eaters can hit the same target with soy (tofu, tempeh, edamame), pea protein isolate, and combinations of legumes and grains — just expect to eat a somewhat larger volume to match the leucine dose.
Supporting Cofactors: Magnesium, K2, Boron, Zinc
Calcium, vitamin D, and protein are the big three. A smaller set of minerals and vitamins matter around the edges:
Magnesium is required for the enzymatic conversion of vitamin D into its active form (1,25-dihydroxyvitamin D) and for healthy parathyroid hormone signaling. About half of U.S. adults fall short of the RDA (420 mg/day for men, 320 mg/day for women). Food sources include pumpkin seeds, almonds, spinach, black beans, dark chocolate, and whole grains. If you supplement, magnesium glycinate or citrate is better tolerated than magnesium oxide (which mostly acts as a laxative). See the Magnesium page.
Vitamin K2 (menaquinone) activates osteocalcin, the protein that binds calcium into bone matrix, and activates matrix-Gla protein, which keeps calcium out of arteries. Two forms matter: MK-4 (short half-life, used in Japan at high doses — 45 mg/day — for osteoporosis with modest fracture-reduction data) and MK-7 (long half-life, typical supplement dose 100–200 mcg/day). Food sources of K2 include natto (by far the densest), hard cheeses, egg yolks, and fermented dairy. K2 is not universally recommended by guidelines, but the biology is coherent and the safety profile at typical supplement doses is reassuring — with one important caveat: anyone on warfarin must keep vitamin K intake consistent and discuss changes with their prescriber, because K antagonizes the drug. K2 does not interact with DOACs (apixaban, rivaroxaban, dabigatran). See the Vitamin K page.
Boron (3 mg/day from diet or supplement) appears to reduce urinary calcium and magnesium loss and to extend the half-life of circulating vitamin D. Food sources: prunes, raisins, almonds, avocados. The evidence base is modest, but the dose is cheap and non-toxic.
Zinc is a cofactor for alkaline phosphatase, a key osteoblast enzyme, and for collagen cross-linking. The RDA is 11 mg/day (men), 8 mg/day (women). Oysters, beef, pumpkin seeds, lentils, and cashews are good sources. See the Zinc page. High-dose zinc supplements (>40 mg/day long-term) can induce copper deficiency; don't megadose without a reason.
Timing Around Bisphosphonates and Other Medications
If you are on an oral bisphosphonate (alendronate, risedronate, ibandronate), timing of calcium becomes a sharper issue. Oral bisphosphonates are notorious for poor absorption — less than 1% of the dose gets into circulation under ideal conditions, and any calcium, magnesium, iron, or coffee in the stomach essentially zeroes that out.
The standard protocol:
- Take the bisphosphonate first thing in the morning, with a full glass of plain water — not coffee, not juice, not mineral water.
- Remain upright (sitting or standing) and do not eat, drink anything other than plain water, or take other medications for 30 minutes (60 minutes for ibandronate).
- Then eat breakfast and take calcium, vitamin D, and other supplements.
- IV bisphosphonates (zoledronate, the annual infusion) bypass this issue entirely — you can take calcium normally on infusion day, though you should confirm 25(OH)D is >20 ng/mL before the infusion to avoid post-infusion hypocalcemia.
For full treatment details, see the bisphosphonates page. Denosumab (Prolia) requires adequate calcium and vitamin D before every injection to prevent severe hypocalcemia — see the denosumab page for that protocol.
Other timing notes:
- Thyroid hormone (levothyroxine): calcium binds it. Separate by at least 4 hours.
- Fluoroquinolone and tetracycline antibiotics: calcium dramatically reduces absorption. Separate by 2–4 hours.
- Iron supplements: separate from calcium by 2 hours.
- Proton-pump inhibitors: switch to calcium citrate (no stomach acid required).
A Sample Bone-Friendly Day
For a 70-kg postmenopausal woman targeting 1,200 mg calcium, 2,000 IU vitamin D, and 84 g protein:
- Breakfast: 1 cup plain Greek yogurt (17 g protein, 200 mg calcium) with 2 tbsp chopped almonds (40 mg calcium) and berries. 2 scrambled eggs (12 g protein). 2,000 IU vitamin D3 softgel with the meal. Running total: 29 g protein, 240 mg calcium.
- Mid-morning: 1 cup fortified soy milk latte (7 g protein, 300 mg calcium). 36 g, 540 mg.
- Lunch: Canned sardines on whole-grain toast, 3 oz (22 g protein, 325 mg calcium) with a side salad including kale massaged with olive oil. 58 g, 865 mg.
- Afternoon snack: 1 oz cheddar + an apple (10 g protein, 200 mg calcium). 68 g, 1065 mg.
- Dinner: 4 oz baked salmon (25 g protein) with a cup of braised collard greens (270 mg calcium) and a sweet potato. Optional 500 mg calcium citrate if the day ran low. 93 g protein, 1335 mg calcium.
No supplements needed beyond the single D3 softgel and an optional calcium citrate on low-dairy days. This is the food-first pattern guidelines recommend, and it is both cheaper and more sustainable than pill-stacking.
Common Mistakes
- Taking all your calcium in one big dose. Absorption caps around 500–600 mg. Split it.
- Supplementing calcium without checking diet first. Many patients are already at target from food and add a supplement "for insurance," overshooting.
- Ignoring vitamin D while taking bisphosphonates or denosumab. Low 25(OH)D plus these drugs can trigger hypocalcemia and stall bone rebuilding.
- Eating 0.8 g/kg protein because that's the RDA. Older adults need 1.0–1.2 g/kg minimum.
- Loading all protein at dinner. You trigger the anabolic response once, then waste breakfast and lunch.
- Taking calcium carbonate while on a PPI. Switch to citrate.
- Relying on spinach for calcium. Oxalates block most of it. Kale, collards, bok choy absorb far better.
- Not rechecking 25(OH)D after starting supplementation. Retest at 3 months and adjust the dose.
Key Research Papers
The Chapuy/Dawson-Hughes nursing-home calcium+D fracture trials, the recent VITAL and D-Health large-scale supplementation studies, the Bischoff-Ferrari and Bolland calcium-controversy meta-analyses, the PROT-AGE and ESCEO/IOF protein consensus statements, and the Endocrine Society and IOM intake guidelines.
- Chapuy MC, Arlot ME, Duboeuf F, et al. Vitamin D3 and Calcium to Prevent Hip Fractures in Elderly Women. New England Journal of Medicine. 1992;327(23):1637–1642.
- Dawson-Hughes B, Harris SS, Krall EA, Dallal GE. Effect of Calcium and Vitamin D Supplementation on Bone Density in Men and Women 65 Years of Age or Older. New England Journal of Medicine. 1997;337(10):670–676.
- Tang BM, Eslick GD, Nowson C, Smith C, Bensoussan A. Use of Calcium or Calcium in Combination with Vitamin D Supplementation to Prevent Fractures and Bone Loss in People Aged 50 Years and Older: A Meta-Analysis. Lancet. 2007;370(9588):657–666.
- Bischoff-Ferrari HA, Willett WC, Wong JB, et al. Prevention of Nonvertebral Fractures with Oral Vitamin D and Dose Dependency: A Meta-Analysis of Randomized Controlled Trials. Archives of Internal Medicine. 2009;169(6):551–561.
- LeBoff MS, Chou SH, Ratliff KA, et al. Supplemental Vitamin D and Incident Fractures in Midlife and Older Adults (VITAL). New England Journal of Medicine. 2022;387(4):299–309.
- Manson JE, Cook NR, Lee IM, et al. Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease (VITAL). New England Journal of Medicine. 2019;380(1):33–44.
- Waterhouse M, Sanguineti E, Baxter C, et al. The Effect of Monthly Vitamin D Supplementation on Fractures: A Tertiary Outcome from the Population-Based, Double-Blind, Randomised, Placebo-Controlled D-Health Trial. Lancet Diabetes & Endocrinology. 2023;11(5):324–332.
- Bolland MJ, Avenell A, Baron JA, et al. Effect of Calcium Supplements on Risk of Myocardial Infarction and Cardiovascular Events: Meta-Analysis. BMJ. 2010;341:c3691.
- Kopecky SL, Bauer DC, Gulati M, et al. Lack of Evidence Linking Calcium With or Without Vitamin D Supplementation to Cardiovascular Disease in Generally Healthy Adults: A Clinical Guideline from the National Osteoporosis Foundation and the American Society for Preventive Cardiology. Annals of Internal Medicine. 2016;165(12):867–868.
- Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology & Metabolism. 2011;96(7):1911–1930.
- Bauer J, Biolo G, Cederholm T, et al. Evidence-Based Recommendations for Optimal Dietary Protein Intake in Older People: A Position Paper from the PROT-AGE Study Group. Journal of the American Medical Directors Association. 2013;14(8):542–559.
- Rizzoli R, Biver E, Bonjour JP, et al. Benefits and Safety of Dietary Protein for Bone Health — An Expert Consensus Paper Endorsed by the European Society for Clinical and Economical Aspects of Osteoporosis, Osteoarthritis, and Musculoskeletal Diseases and by the International Osteoporosis Foundation. Osteoporosis International. 2018;29(9):1933–1948.
- Ross AC, Manson JE, Abrams SA, et al. The 2011 Report on Dietary Reference Intakes for Calcium and Vitamin D from the Institute of Medicine: What Clinicians Need to Know. Journal of Clinical Endocrinology & Metabolism. 2011;96(1):53–58.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: calcium intake and BMD
- PubMed: calcium citrate vs carbonate
- PubMed: calcium and cardiovascular risk
- PubMed: 25(OH)D and fracture risk
- PubMed: vitamin D3 vs D2
- PubMed: VITAL trial fractures
- PubMed: protein intake and hip fracture
- PubMed: leucine and muscle synthesis
- PubMed: vitamin K2 MK-7 BMD
- PubMed: magnesium and bone health
Connections
- Bone Remodeling & Calcium Balance — interactive animation
- Calcium
- Vitamin D3
- Magnesium
- Vitamin K
- Zinc
- Osteoporosis
- Bisphosphonates
- Weight-Bearing and Resistance Exercise
- Denosumab, Romosozumab and Teriparatide
- FRAX Risk Assessment
- Secondary Osteoporosis Causes
- Fracture Prevention and Fall Risk
- Postmenopausal Osteoporosis and Hormone Therapy
- DEXA Scan: T-Score and Z-Score
- Leucine
- Collagen
- Milk
- Sardines