Non-Hormonal Options: SSRIs, Gabapentin, Fezolinetant
You may have very good reasons not to take hormone therapy. A personal or strong family history of breast cancer. A prior blood clot, stroke, or known thrombophilia. Active liver disease. Unexplained vaginal bleeding. Or simply — after reading the risks and talking to your clinician — the decision that estrogen is not the right tool for you. None of that means you have to white-knuckle your way through hot flashes, 3 a.m. drenching sweats, and the brain fog that rides along with them.
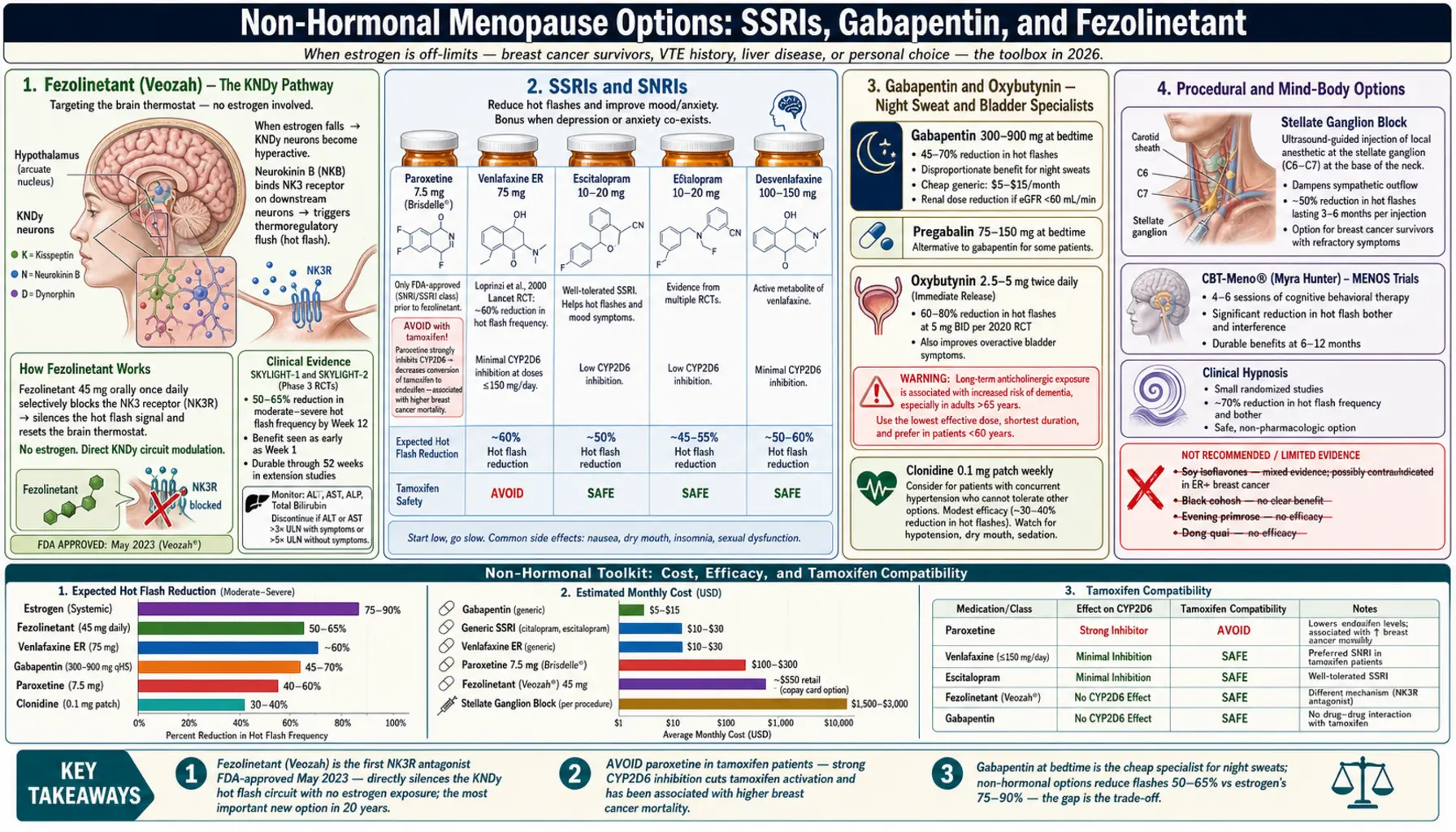
The good news: the non-hormonal toolbox has expanded dramatically, including a first-in-class drug (fezolinetant) approved in 2023 that targets the brain circuit driving hot flashes directly. The not-so-good news: most non-hormonal options deliver roughly a 50–65% reduction in vasomotor symptoms, compared with the 75–90% reduction estrogen typically provides. That gap matters, and it is the main reason non-hormonal therapy sometimes leads back to a second conversation about HRT.
This article walks through every evidence-backed non-hormonal option currently used in 2026, with realistic expectations, dosing, side effects, and costs.
Interactive Visualization Menopause — run the hormones down and set off a hot flash Empty the ovarian follicle pool and watch estradiol swing, then flatten, while FSH climbs — then trigger a hot flash and see the narrowed thermoneutral zone behind it. Launch →Table of Contents
- Who This Article Is For
- Fezolinetant (Veozah) — The New NK3R Antagonist
- SSRIs and SNRIs — Paroxetine, Venlafaxine, and Cousins
- Gabapentin and Pregabalin — Night-Sweat Specialists
- Clonidine and Oxybutynin
- Stellate Ganglion Block
- CBT, Mindfulness, and Hypnosis
- Herbs, Soy, and Supplements
- Acupuncture, Cooling Devices, and Weighted Blankets
- When to Reopen the HRT Conversation
- Key Research Papers
- PubMed Topic Searches
- Connections
- Featured Videos
Who This Article Is For
Non-hormonal therapy is standard of care if you fall into any of these groups:
- Personal history of hormone-sensitive breast cancer (ER-positive), and especially if you are on tamoxifen or an aromatase inhibitor.
- Prior deep vein thrombosis, pulmonary embolism, or stroke, or a known thrombophilia (Factor V Leiden, prothrombin mutation, antiphospholipid syndrome).
- Active liver disease or recent unexplained elevated liver enzymes.
- Unexplained vaginal bleeding that has not yet been worked up.
- Coronary artery disease or recent heart attack, particularly if you are more than 10 years past menopause.
- Personal preference — you read about HRT and decided it is not for you. That is a valid reason, and a good clinician will work with it.
For everyone else, non-hormonal options are still reasonable either as first-line (if you prefer) or as add-ons to HRT when estrogen alone is not fully controlling symptoms.
Fezolinetant (Veozah) — The New NK3R Antagonist
Fezolinetant, sold as Veozah, is the first drug designed specifically to silence the brain circuit that causes hot flashes. It was FDA-approved in May 2023 for moderate-to-severe vasomotor symptoms of menopause. For women who cannot take estrogen, this is the most important new tool in 20 years.
How it works. When ovarian estrogen falls, a cluster of neurons in the hypothalamus called KNDy neurons (kisspeptin, neurokinin B, dynorphin) become hyperactive. These neurons release neurokinin B, which binds the NK3 receptor and triggers the thermoregulatory flush — the cascade you feel as a hot flash. Fezolinetant blocks the NK3 receptor. No estrogen involved. The brain thermostat resets without touching breast, uterine, or clotting tissue.
Dose. 45 mg orally once daily, any time of day, with or without food.
What to expect. In the SKYLIGHT-1 and SKYLIGHT-2 phase 3 trials, women taking fezolinetant had roughly a 50–65% reduction in the frequency of moderate-to-severe hot flashes by week 12, with significant improvement as early as week 1. Severity scores also dropped. Benefit maintained through 52 weeks of open-label extension.
Liver monitoring is required. The FDA requires baseline liver function tests (ALT, AST, alkaline phosphatase, total bilirubin) before starting, then at months 3, 6, and 9. A small but real fraction of patients develop asymptomatic liver enzyme elevations; almost all reverse on stopping the drug. Do not take fezolinetant if you have cirrhosis or severe liver impairment.
Side effects. Abdominal pain, diarrhea, insomnia, back pain, and hot flash (paradoxically, as the body adjusts). Most are mild.
Drug interactions. Fezolinetant is primarily metabolized by CYP1A2. Strong or moderate CYP1A2 inhibitors (ciprofloxacin, fluvoxamine, mexiletine) are contraindicated or require caution — they can raise fezolinetant levels significantly.
Cost reality. List price is approximately $550 per month in the U.S. (about $6,600/year). Coverage is improving but still inconsistent — many commercial plans require step therapy (trial of an SSRI or gabapentin first) before approving Veozah. The manufacturer (Astellas) runs a patient assistance program and a copay card for commercially insured patients that can bring out-of-pocket cost to as low as $5–$30/month; call 1-844-VEOZAH-1 or ask your prescribing clinician's office to help enroll. Without insurance or assistance, cost is a real barrier. A second NK3R antagonist, elinzanetant, is in late-stage trials and may broaden options when approved.
Bottom line. For a woman with breast cancer history who is miserable on tamoxifen with uncontrolled flashes, fezolinetant is often the single best option. Ask specifically for it by name; some clinicians are still unfamiliar with it.
SSRIs and SNRIs — Paroxetine, Venlafaxine, and Cousins
Antidepressants in the SSRI and SNRI families reduce hot flashes through serotonin and norepinephrine pathways in the hypothalamus. The effect appears within 1–2 weeks — much faster than their antidepressant effect, which takes 4–6 weeks.
Paroxetine 7.5 mg (Brisdelle)
The only FDA-approved non-hormonal treatment for hot flashes before fezolinetant. Brisdelle is a low-dose paroxetine formulation (7.5 mg) specifically dosed below the antidepressant range to minimize side effects while retaining hot flash benefit.
- Dose: 7.5 mg at bedtime.
- Expected benefit: 40–60% reduction in hot flash frequency.
- Big warning: Avoid in women taking tamoxifen. Paroxetine is a strong inhibitor of CYP2D6, the enzyme that converts tamoxifen into its active metabolite endoxifen. Co-administration can cut tamoxifen's effectiveness and has been associated with higher breast cancer mortality in retrospective studies. If you are on tamoxifen, choose venlafaxine, desvenlafaxine, escitalopram, or citalopram instead.
- Side effects: Nausea (usually transient), headache, drowsiness. Less sexual side effects at 7.5 mg than at antidepressant doses.
- Discontinuation: Taper slowly — paroxetine has the worst discontinuation syndrome of any SSRI. Do not stop cold.
Venlafaxine (Effexor XR) — Off-Label but Widely Used
Venlafaxine is an SNRI that became the de facto standard for non-hormonal hot flash treatment after Charles Loprinzi's landmark 2000 Lancet trial in breast cancer survivors.
- Dose: Start 37.5 mg extended-release for 1 week, then increase to 75 mg daily. Higher doses (150 mg) add modest benefit but significantly more side effects.
- Expected benefit: About 60% reduction in hot flash frequency at 75 mg.
- Safe with tamoxifen — minimal CYP2D6 inhibition.
- Side effects: Nausea (first 1–2 weeks), dry mouth, decreased appetite, mild blood pressure elevation at doses >150 mg, sexual dysfunction.
- Discontinuation syndrome: Taper over 2–4 weeks. Venlafaxine has a short half-life and missed doses feel unpleasant quickly ("brain zaps").
Escitalopram, Citalopram, and Desvenlafaxine
- Escitalopram (Lexapro) 10–20 mg — roughly 50% hot flash reduction; tamoxifen-safe; generally well tolerated.
- Citalopram (Celexa) 10–20 mg — similar efficacy to escitalopram; watch QT interval at doses above 20 mg in older women.
- Desvenlafaxine (Pristiq) 100–150 mg — active metabolite of venlafaxine; FDA-studied specifically for vasomotor symptoms though not FDA-labeled for them; reasonable alternative for women who had GI side effects on venlafaxine.
If you already have co-existing depression or anxiety, choosing an SSRI/SNRI that treats both at once is elegant — two birds, one daily pill. See the depression article for a broader overview of these drugs.
Gabapentin and Pregabalin — Night-Sweat Specialists
Gabapentin (Neurontin) is an anticonvulsant originally developed for seizures and nerve pain. It turns out to blunt hot flashes too, and its sedating side effect is a feature, not a bug, if you take it at bedtime: it simultaneously quiets night sweats and helps you sleep through what is left.
- Dose: Start 300 mg at bedtime for 3 nights. Increase to 600 mg at bedtime if tolerated. Can go up to 900 mg at bedtime or split as 300 mg three times daily (total 900 mg) if daytime flashes remain.
- Expected benefit: 45–70% reduction in hot flash frequency, with disproportionate benefit for night sweats because of the timing and sedation.
- Best candidates: Women whose dominant complaint is drenching 2 a.m. sweats that wreck sleep. The sleep benefit is often the biggest quality-of-life win.
- Side effects: Drowsiness (usually wears off in 1–2 weeks), dizziness on standing, mild weight gain, rarely ankle swelling. In older women, watch for fall risk.
- Renal dosing: Gabapentin is cleared by the kidneys. Reduce the dose if eGFR is below 60 mL/min.
- Cheap and generic. Typical U.S. cost with GoodRx: $5–$15/month.
Pregabalin (Lyrica) 75–150 mg at bedtime is similar in mechanism and effect. Slightly better bioavailability than gabapentin, but more expensive (though now generic) and controlled schedule V in the U.S. Reasonable second choice if gabapentin is not tolerated.
Clonidine and Oxybutynin
Clonidine 0.1 mg Patch
Clonidine is a central alpha-2 adrenergic agonist originally used for high blood pressure. It reduces hot flashes modestly — about 30–40% reduction — and has fallen out of first-line use since better options appeared. Still reasonable if you have concurrent mild hypertension and want to knock out two issues with one drug.
- Form: 0.1 mg/24-hour transdermal patch, changed weekly. Oral dosing (0.05–0.1 mg twice daily) also works but causes more dry mouth and rebound hypertension if missed.
- Side effects: Dry mouth, dizziness, drowsiness, rebound hypertension on sudden withdrawal.
Oxybutynin 2.5–5 mg
Oxybutynin is an anticholinergic normally used for overactive bladder. In a 2020 randomized trial it cut hot flashes by about 60–80% at 5 mg twice daily — a striking result. But there is a serious caveat.
The dementia concern. Chronic anticholinergic exposure has been associated with higher dementia risk in long-term observational studies, particularly in women over 65. The effect seems dose- and duration-dependent. For that reason, oxybutynin is best used:
- At the lowest dose that works (try 2.5 mg twice daily first).
- For the shortest duration you can tolerate (bridge therapy, a few months to a couple of years, not a 20-year plan).
- In women under 60 rather than women 70+.
- If overactive bladder is also a problem, this is an elegant two-for-one.
Other side effects: dry mouth, constipation, blurred vision, urinary retention. Avoid if you have narrow-angle glaucoma.
Stellate Ganglion Block
A stellate ganglion block is an ultrasound-guided injection of local anesthetic into the stellate ganglion — a cluster of sympathetic nerves at the base of the neck. It is a procedural option, not a drug, and it is performed by pain-medicine or anesthesia specialists.
- What it does: Temporarily silences sympathetic nervous system output above the neck. For reasons that are still being worked out, this dampens the thermoregulatory misfiring that drives hot flashes.
- Expected benefit: In small randomized trials, roughly 50% reduction in moderate-to-severe hot flashes lasting 3–6 months per injection. Some women get 9–12 months.
- Who might consider it: Breast cancer survivors with severe refractory hot flashes who cannot or will not take medication daily, or who have failed multiple oral options.
- Risks: Temporary Horner's syndrome (droopy eyelid, small pupil, flushed face on one side) is common and expected; resolves in hours. Rare serious risks: hoarseness from recurrent laryngeal nerve block, bleeding, nerve injury, pneumothorax, intravascular injection.
- Cost and access: $1,500–$3,000 per procedure; insurance coverage is inconsistent and often requires specific documentation (failed medical therapy, breast cancer context). Not widely available outside academic pain centers.
CBT, Mindfulness, and Hypnosis
Cognitive Behavioral Therapy for Menopausal Symptoms (CBT-Meno)
This is not generic CBT. Myra Hunter's group in the UK developed a structured 4–6 session protocol that specifically targets the cognitive and behavioral components of hot flashes, night sweats, and mood around menopause. The MENOS trials (MENOS-1, MENOS-2, MENOS-4) consistently show clinically meaningful reductions in hot flash bother — the subjective impact — even when the frequency of flashes changes less.
- Format: Four to six weekly sessions, either individual or group, in-person or via telehealth. Self-help workbooks and apps (such as the NHS-used "Women's Health CBT" program) work nearly as well as face-to-face in randomized data.
- What it teaches: Recognizing and reframing catastrophic thoughts during a flash ("everyone is staring, I'm going to faint"), paced breathing at the onset of a flash, sleep hygiene, and behavioral activation for mood.
- Best for: Women who tell their clinician "the flashes aren't even that frequent but they are ruining my life." CBT closes the gap between physiology and suffering.
- Combinable: Works alongside every other option on this page and alongside HRT.
Mindfulness and Hypnosis
Mindfulness-based stress reduction (MBSR, 8-week group format) and clinical hypnosis (Gary Elkins' protocols) have modest but real evidence for hot flash reduction — around 30–50% reduction in bother, less in frequency. Hypnosis in particular had good results in a 2013 randomized trial in breast cancer survivors. Both are safe, have no drug interactions, and layer well with other therapies.
Herbs, Soy, and Supplements
Most over-the-counter menopause supplements have weaker evidence than the pharmaceutical options above, but several are popular and some women respond well. Here is a grounded look.
Black Cohosh (Cimicifuga racemosa)
Black cohosh is the most-studied herb for menopause. Trials are mixed — some show modest benefit, others show no difference from placebo. The German Commission E monograph endorsed it for menopausal symptoms, and it remains widely used in Europe under brand names like Remifemin.
- Typical dose: 40–80 mg of standardized extract daily.
- Expected benefit: Small, around 20–30% reduction in hot flash frequency in responders; no effect in many.
- Liver concern: Rare case reports of hepatotoxicity, probably idiosyncratic. Stop and get liver enzymes checked if you develop fatigue, dark urine, or right-upper-quadrant pain. Avoid if you have existing liver disease.
- Mechanism: Not estrogenic in most studies, so theoretically acceptable in breast cancer survivors, but data are thin and guidelines vary. Talk to your oncologist before starting.
Soy Isoflavones and S-Equol
Soy isoflavones (genistein, daidzein) are phytoestrogens that bind estrogen receptor beta preferentially. Whole-soy-food diets (tofu, tempeh, edamame, soy milk) appear safer and possibly more effective than concentrated supplements.
- S-equol is a bacterial metabolite of daidzein. Only about 30% of Western women (vs 50–60% of Japanese women) have the gut bacteria to produce it. Direct S-equol supplements (10 mg twice daily) bypass that genetic lottery and have shown modest benefit (around 30% flash reduction) in small trials.
- Breast cancer survivors: Evidence now suggests dietary soy is not harmful and may be modestly protective, but high-dose isolated isoflavone supplements remain a gray area. Whole-food soy is the safer choice.
Options with Weak or No Evidence
- Evening primrose oil — randomized trials show no benefit for hot flashes. Skip it.
- Red clover — trials are inconsistent; meta-analyses show either no effect or very modest effect. Contains isoflavones similar to soy.
- Vitamin E 400 IU — a classic Loprinzi trial showed about 1 fewer hot flash per day than placebo. Minimal benefit; at 400 IU the dose is safe for most women but higher doses have been linked to increased all-cause mortality in meta-analyses.
- Dong quai, wild yam cream, maca, ginseng — limited or negative evidence.
See the ashwagandha page for an adaptogen that has better evidence for perimenopausal anxiety and sleep than for hot flashes specifically.
Acupuncture, Cooling Devices, and Weighted Blankets
Acupuncture
Meta-analyses are mixed. The most rigorous sham-controlled trials (including the 2016 Acupuncture in Menopause / AIM trial) show modest benefit over usual care but comparable to sham acupuncture — meaning the treatment works largely through nonspecific effects. That said, the treatment is safe, many women enjoy it, and the regular ritual itself can reduce menopause-related stress. If you have access and budget, it is reasonable to try 8–12 weekly sessions and judge the response.
Cooling Pillows, Mattress Pads, and Fans
- Chillow and gel-core pillows: Cheap (~$30), no downside, meaningfully improve the night-sweat wake-up experience.
- Ooler / BedJet / ChiliPad active-cooling mattress pads (~$500–$1,500) — circulate cool water or air under you and drop core temperature during the flash. Many women describe these as life-changing for sleep and worth every dollar.
- Bedside fan: cheap, effective, and the sound doubles as a sleep aid.
- Moisture-wicking pajamas (bamboo, merino, technical fabrics) — spare your partner and the mattress.
Weighted Blankets
A paradox — they are warm but also calming. Small sleep studies show modest improvement in insomnia, particularly in women with co-existing anxiety. If your sweats are night-dominant, a weighted blanket may make flashes worse; a cooling pad plus a lighter blanket is a better combination. If your problem is anxiety-driven insomnia more than temperature, a weighted blanket can help.
When to Reopen the HRT Conversation
Many women start non-hormonal therapy convinced that HRT is off the table, then rediscover — after a fair trial — that the symptom relief is not enough to live a full life. That is not a failure; it is data. A reasonable trigger list for revisiting HRT with a clinician:
- Two or more non-hormonal options tried for at least 8–12 weeks each at adequate dose, without acceptable symptom control.
- Sleep is still destroyed — waking more than 3 times per night from sweats after gabapentin and cooling measures.
- Work performance or relationships are suffering.
- Your original reason for avoiding HRT has changed — for example, your breast cancer history is now 5+ years out with no recurrence and your oncologist has softened on vaginal estrogen or even on low-dose systemic therapy.
- Vaginal and urinary symptoms persist. Low-dose vaginal estrogen has minimal systemic absorption and is generally considered safe even in most breast cancer survivors after a conversation with their oncologist.
Non-hormonal therapy and HRT are not mutually exclusive. Some women do best on a low-dose estradiol patch plus gabapentin at night, or on fezolinetant plus vaginal estrogen, or on CBT plus an SSRI. The goal is the minimum intervention that lets you sleep through the night and get through the day feeling like yourself.
Key Research Papers
- Johnson KA, Martin N, Nappi RE, et al. Efficacy and safety of fezolinetant in moderate-to-severe vasomotor symptoms associated with menopause: the SKYLIGHT 1 randomised trial. Lancet. 2023.
- Stearns V, Beebe KL, Iyengar M, Dube E. Paroxetine controlled release in the treatment of menopausal hot flashes: a randomized controlled trial. JAMA. 2003.
- Loprinzi CL, Kugler JW, Sloan JA, et al. Venlafaxine in management of hot flashes in survivors of breast cancer: a randomised controlled trial. Lancet. 2000.
- The 2023 Nonhormone Therapy Position Statement of The North American Menopause Society. Menopause. 2023.
- Search PubMed
- Search PubMed
PubMed Topic Searches
For current peer-reviewed literature on each option, these PubMed searches return the most relevant recent work:
- Fezolinetant and vasomotor symptoms
- Paroxetine and menopausal hot flashes
- Venlafaxine for hot flashes in breast cancer survivors
- Gabapentin for menopausal night sweats
- Oxybutynin for hot flashes
- Stellate ganglion block for hot flashes
- CBT for menopausal hot flashes (MENOS trials)
- Black cohosh randomized trials in menopause
- Soy isoflavones and S-equol for hot flashes
- Nonhormonal therapy position statements
Connections
- Menopause: Why the Hormones Fall and What Changes — interactive animation
- Depression
- Ashwagandha
- Genitourinary Syndrome of Menopause and Vaginal Estrogen
- Insomnia
- Micronized Progesterone vs Synthetic Progestins
- Estradiol Formulations: Patch, Gel, Oral Routes
- HRT Risks: Breast Cancer, Clots and Stroke
- Testosterone Therapy for Women
- Vasomotor Symptoms: Hot Flashes and Night Sweats
- Perimenopause Symptom Tracker and Hormonal Testing
- Bone Loss Prevention and HRT
- Perimenopause
- Menopause and HRT
- Black Cohosh
- Anxiety
- Hypertension
- Sleep Hygiene
- Dementia
- Breast Cancer
- Dong Quai (Angelica sinensis) — the “limited or negative evidence” entry above, spelled out: a negative 24-week randomized trial for hot flushes, plus a documented warfarin bleeding interaction