Micronized Progesterone vs Synthetic Progestins
If you have a uterus and you take estrogen for menopause, you also need a progestogen. The reason is simple and non-negotiable: estrogen alone thickens the lining of the uterus (the endometrium), and after a few years of unopposed stimulation, that thickening can progress to endometrial hyperplasia and, in a minority of women, to endometrial cancer. A progestogen opposes estrogen's effect on the uterine lining and keeps it thin and safe. That is the single job progestogen must do in menopausal HRT.
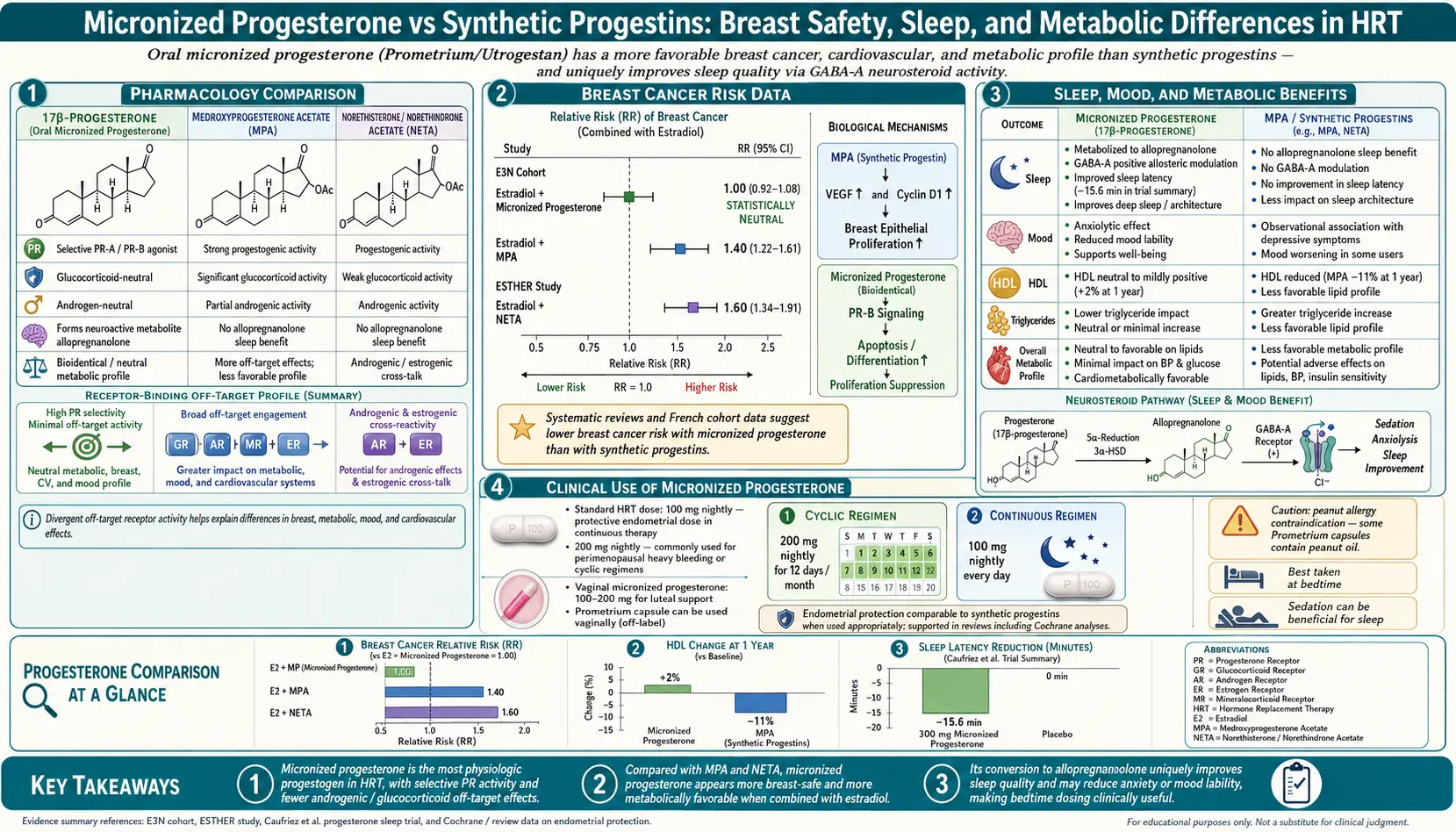
What kind of progestogen you take is not a cosmetic choice. There are two broad families: micronized progesterone (Prometrium, Utrogestan) — a bioidentical molecule structurally identical to the progesterone your ovaries made before menopause — and the synthetic progestins, a family of lab-made molecules (medroxyprogesterone acetate/MPA, norethisterone, levonorgestrel, drospirenone, and others) that mimic some of progesterone's actions but behave differently in the breast, the brain, and the cardiovascular system. The largest safety signals in the history of menopausal hormone therapy — the breast cancer signal in the WHI combined arm, the mood effects, and much of the anxiety women feel about HRT — trace back to the synthetic progestin in that trial, not to estrogen and not to bioidentical progesterone.
This article walks you through the actual differences: molecule by molecule, dose by dose, side effect by side effect. By the end you should know which form is likely right for you, how to dose it, what to expect at bedtime, what bleeding pattern is normal, and when you can skip progestogen entirely.
Interactive Visualization Menopause — run the hormones down and set off a hot flash Empty the ovarian follicle pool and watch estradiol swing, then flatten, while FSH climbs — then trigger a hot flash and see the narrowed thermoneutral zone behind it. Launch →Table of Contents
- Why Progestogen Is Needed With Estrogen
- The Two Families — Bioidentical vs Synthetic
- Micronized Progesterone — How It Works
- Synthetic Progestins — MPA, Norethisterone, Levonorgestrel
- The Breast Cancer Signal — WHI vs E3N
- Dosing Schedules — Continuous vs Cyclical
- Bleeding Patterns — What Is Normal
- Mood, Sleep, and Other Side Effects
- Vaginal Progesterone and the Mirena IUD
- When You Can Skip Progestogen
- Key Research Papers
- PubMed Topic Searches
- Connections
- Featured Videos
Why Progestogen Is Needed With Estrogen
Estrogen is a growth signal for the endometrium. Every month before menopause, rising estradiol in the first half of the cycle builds up the uterine lining; then progesterone surges after ovulation, converts the lining to a secretory state, and — if no pregnancy occurs — allows it to shed as a period. That monthly progesterone pulse is the body's natural brake on estrogen's growth effect.
In menopausal HRT you are typically giving estrogen every day with no cycle to create the natural brake. Without a progestogen, the endometrium keeps thickening. After two to three years of unopposed systemic estrogen, the relative risk of endometrial cancer rises roughly two- to eight-fold, depending on dose. Adding any adequate progestogen brings that risk back down to — and often below — the risk of an untreated postmenopausal woman.
This is why every reputable menopause guideline (NAMS/Menopause Society, IMS, NICE, British Menopause Society) says the same thing: if you have a uterus and you take systemic estrogen, you take a progestogen. The choice is which one.
The Two Families — Bioidentical vs Synthetic
The word "progesterone" is often used loosely. Clinically and chemically, these are distinct molecules:
- Micronized progesterone (Prometrium in the U.S., Utrogestan in Europe/UK, sold generically as well). The molecule is structurally identical to the progesterone your ovaries produced. "Micronized" refers only to the manufacturing process — the drug is milled into very small particles and suspended in oil so it can be absorbed from the gut. Bioidentical does not mean natural-source; it is synthesized in a lab from plant sterols, but the end product is the same molecule as human progesterone.
- Synthetic progestins. A family of lab-designed molecules. They activate the progesterone receptor but differ in structure, and most also activate other steroid receptors (androgen, glucocorticoid, mineralocorticoid) to varying degrees. That off-target receptor activity is why different progestins have very different side-effect profiles. Important members:
- Medroxyprogesterone acetate (MPA) — sold as Provera, and the progestin component of Prempro. This is the drug used in the Women's Health Initiative combined arm.
- Norethisterone / norethindrone — a 19-nortestosterone derivative (descended from testosterone, not progesterone), so it has some androgenic activity.
- Levonorgestrel — also 19-nortestosterone-derived; the hormone released by the Mirena IUD.
- Drospirenone — a spironolactone derivative with mild antimineralocorticoid and anti-androgenic activity; used in some combined HRT products.
- Dydrogesterone — a close structural cousin of progesterone, more selective than MPA; widely used in Europe, not in the U.S.
The practical point: progestin is not progesterone. Most of the published concern about progestogen safety in HRT comes from studies of synthetic progestins, especially MPA.
Micronized Progesterone — How It Works
Oral micronized progesterone is taken at bedtime, and the bedtime timing is not a stylistic preference — it is a pharmacology-driven instruction. When you swallow a progesterone capsule, the liver metabolizes a large fraction of it into neurosteroid metabolites, most importantly allopregnanolone and pregnanolone. These metabolites are potent positive allosteric modulators of the GABA-A receptor — the same receptor hit by alcohol, benzodiazepines, and Z-drugs — but at a far milder, non-addictive intensity.
The result is a gentle sedating, anxiolytic effect that peaks about one to three hours after the dose. Many women report deeper, less-broken sleep on oral micronized progesterone, and some describe a calmer baseline during the day as well. The same mechanism is why a daytime dose makes most people feel foggy or sleepy — take it at night and you convert that side effect into a benefit.
Standard menopausal doses:
- 100 mg at bedtime, every night — the continuous-combined regimen. Used when you want no bleeding.
- 200 mg at bedtime for 12–14 days per month — the cyclical regimen. Produces a predictable monthly withdrawal bleed.
Product availability: Prometrium 100 mg and 200 mg capsules in the U.S.; Utrogestan 100 mg in the UK and Europe (often dosed as two capsules for 200 mg). The capsules contain peanut oil in some formulations — relevant for peanut-allergic patients, who should request the newer sunflower-oil generic.
Synthetic Progestins — MPA, Norethisterone, Levonorgestrel
Medroxyprogesterone acetate (MPA). The classic North American HRT progestin. Usually dosed as 2.5 mg daily (continuous) or 5–10 mg for 12–14 days per month (cyclical). MPA is reliable at protecting the endometrium and it is cheap. What makes it controversial is everything else: in the WHI combined arm it was the progestogen paired with conjugated equine estrogens (Prempro), and that arm — not the estrogen-alone arm — carried the excess breast cancer signal, the excess cardiovascular events, and much of the mood and weight complaints that drove women off HRT in the 2000s.
Norethisterone / norethindrone. Structurally a modified testosterone molecule. Can cause mild androgenic side effects (oily skin, acne in susceptible women) and is sometimes associated with less favorable lipid effects than progesterone. Common in European HRT patches (e.g., combined transdermal estradiol + norethisterone).
Levonorgestrel. Also 19-nortestosterone-derived. When given systemically in HRT it carries a similar profile to norethisterone. When delivered locally from the Mirena IUD, the picture changes dramatically — the dose in the bloodstream is tiny and the effect is overwhelmingly on the endometrium (see alternatives section below).
Drospirenone. The progestin in Angeliq (combined with estradiol). Mildly diuretic and anti-androgenic, which some women find tolerable. Slightly raises venous-clot risk in younger contraceptive use; in postmenopausal doses the signal is smaller but present.
Dydrogesterone. Behaves most like progesterone of the synthetic family. The large French E3N cohort suggested its breast profile looks more like micronized progesterone than like MPA — encouraging, but it is not available in the U.S.
The Breast Cancer Signal — WHI vs E3N
This is the single most important data point for most women choosing a progestogen, so it is worth walking through carefully.
The Women's Health Initiative (WHI), combined arm, 2002. Postmenopausal women took conjugated equine estrogens 0.625 mg + MPA 2.5 mg daily versus placebo. After about 5.6 years the trial was stopped early. The combined arm showed a small absolute increase in invasive breast cancer — roughly 8 additional cases per 10,000 women per year. The estrogen-alone arm (women without a uterus, given conjugated estrogens with no progestin) showed no increase in breast cancer, and over longer follow-up actually trended toward a reduction. The difference between the two arms is almost entirely attributable to MPA.
The French E3N cohort. A large prospective study of roughly 80,000 French women followed for more than a decade. E3N separately tracked women on estrogen + micronized progesterone, estrogen + dydrogesterone, and estrogen + various synthetic progestins. The result was striking: women using estrogen + micronized progesterone (or dydrogesterone) showed little to no increase in breast cancer risk at the typical five-year mark, while women using estrogen + synthetic progestins showed a clear increase similar to WHI. The key 2008 paper is Fournier et al., Breast Cancer Research and Treatment.
Caveats worth stating plainly. E3N is observational, not randomized, so it is vulnerable to residual confounding. The micronized-progesterone arm showed some signal at longer durations (beyond five to eight years). And we still do not have a randomized trial the size of WHI testing bioidentical progesterone head-to-head against a synthetic progestin. But the consistent finding across E3N and several smaller cohorts — that micronized progesterone has a more favorable breast profile than MPA — is the basis for the current preference among menopause specialists for transdermal estradiol plus oral micronized progesterone as the default modern regimen.
Dosing Schedules — Continuous vs Cyclical
Two main schedules exist. Either is acceptable for endometrial protection; the choice turns on whether you want bleeding or not, and how close you are to your final menstrual period.
Continuous combined. Estrogen every day plus progesterone (or progestin) every day. For micronized progesterone this is 100 mg at bedtime nightly. For MPA it is 2.5 mg daily. This regimen is the standard once a woman is clearly postmenopausal (usually at least one full year after her last period, or age 54+). Goal: no bleeding.
Cyclical / sequential. Estrogen every day plus a pulse of progesterone/progestin for 12–14 days each calendar month, followed by a progesterone-free interval during which the endometrium sheds as a predictable withdrawal bleed. For micronized progesterone the typical schedule is 200 mg at bedtime, days 1–12 or 1–14 of the month. For MPA, 5–10 mg for the same window. This is preferred in perimenopause or within the first 12 months of menopause, when a continuous regimen often produces nuisance breakthrough bleeding.
A reasonable rule: start cyclical if you are still having any periods or your last period was under a year ago; switch to continuous combined once bleeding has stopped for a year or two, or once you are around age 54 and have been on cyclical for a while.
Bleeding Patterns — What Is Normal
Bleeding is the single most common reason women quit HRT early, often unnecessarily. What to expect:
- On cyclical dosing, a predictable bleed in the week after the progestogen stops is expected and reassuring — it means the endometrium is behaving normally.
- On continuous combined dosing, irregular light spotting in the first 3–6 months is common and does not mean something is wrong. It usually settles as the endometrium atrophies under daily progestogen.
- Bleeding that should prompt evaluation: any bleeding that starts after six months of amenorrhea on continuous combined; heavy bleeding; bleeding that returns after it had stopped; any bleeding in a woman who is clearly postmenopausal and not on HRT. The standard workup is a transvaginal ultrasound (looking at endometrial thickness) and, if indicated, endometrial biopsy.
A useful tactic if continuous combined is producing unwanted spotting: switch temporarily to cyclical for six to twelve months, then try continuous combined again. Many women tolerate it second time around once the endometrium has been reset.
Mood, Sleep, and Other Side Effects
The two families diverge most visibly in how they make women feel.
Micronized progesterone. The dominant effects are sedation (use at bedtime), sometimes vivid dreams in the first few weeks, and in a minority of women a paradoxical low mood or irritability. Most women find the sleep benefit is a feature rather than a bug. GI side effects (nausea, mild bloating) can occur with oral dosing — the vaginal route avoids them.
Synthetic progestins. A broader and less predictable side-effect profile. Common complaints include low mood, irritability, anxiety, weight gain, breast tenderness, and bloating. MPA in particular has been reported to trigger or worsen depressive symptoms in women with a history of PMS/PMDD. Androgenic progestins (norethisterone, levonorgestrel) can cause acne, oily skin, and sometimes unfavorable cholesterol changes.
A clinically important pattern: women who felt terrible on Provera often feel dramatically better when switched to micronized progesterone at the same stage of HRT. If a progestogen is making your mood worse, the first-line move is to change the progestogen, not to stop hormone therapy.
Vaginal Progesterone and the Mirena IUD
Two useful alternatives when oral progesterone is not working:
Vaginal micronized progesterone. The same Prometrium/Utrogestan capsules can be inserted vaginally at bedtime. This bypasses the liver, sharply reduces the systemic sedating effect (some women like this, some miss it), eliminates oral GI side effects, and still delivers enough progesterone locally to the uterus to protect the endometrium. Useful for women who cannot tolerate oral dosing or who need daytime alertness. It is technically off-label for endometrial protection in several countries but widely used and supported by endometrial-biopsy studies.
Mirena levonorgestrel IUD. The Mirena releases about 20 micrograms of levonorgestrel per day directly into the uterus. Local endometrial levels are very high, so endometrial suppression is excellent; systemic blood levels are very low, so systemic progestin side effects are minimized. Formally, Mirena is approved as a contraceptive and, in some countries, as treatment for heavy menstrual bleeding; its use as the progestogen component of HRT is technically off-label in the United States but on-label in the UK and much of Europe, and it is widely used for this purpose by menopause specialists. The device lasts 5–8 years and can be a good fit for women who hated oral progestogens, who still need contraception in perimenopause, or who want to avoid the bedtime pill routine.
When You Can Skip Progestogen
The one clear scenario: women who have had a hysterectomy and no longer have a uterus. With no endometrium to protect, there is no reason to take a progestogen, and adding one only exposes you to side effects and, in the case of synthetic progestins, a probable breast cancer signal. Post-hysterectomy women on HRT should generally be on estrogen alone.
Two edge cases deserve a conversation with a menopause-literate clinician rather than a blanket rule:
- History of endometriosis with hysterectomy. Rare residual endometriotic tissue can still respond to estrogen. Some specialists add a small dose of progestogen for a year or two as a precaution; others do not. Individual decision.
- Supracervical hysterectomy (cervix left in place but uterus removed). Small amounts of endometrial tissue may remain at the stump. Most specialists still treat these women as estrogen-only unless there is a specific reason not to.
If you have a uterus and a clinician suggests you take estrogen without any progestogen, get a second opinion. That is not modern practice.
Key Research Papers
- Fournier A, et al. Unequal risks for breast cancer associated with different hormone replacement therapies: results from the E3N cohort study. Breast Cancer Res Treat. 2008;107(1):103–11.
- Writing Group for the Women's Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the WHI randomized controlled trial. JAMA. 2002;288(3):321–333.
- Search PubMed
- PubMed review: micronized progesterone and endometrial protection in HRT
- PubMed review: allopregnanolone, GABA-A modulation, and sleep
- PubMed review: levonorgestrel IUD for endometrial protection in menopausal HRT
PubMed Topic Searches
For further reading, these PubMed topic searches return current peer-reviewed work on progestogen choice in menopausal HRT:
- Micronized progesterone versus MPA and breast cancer risk
- E3N cohort, progestogen type, and breast cancer
- Oral progesterone, sleep, and menopause
- Vaginal progesterone for endometrial protection
- Mirena IUD in menopausal hormone therapy
- Continuous combined HRT bleeding patterns
- Cyclical sequential HRT and endometrial hyperplasia
- Progestin effects on mood and depression in HRT
- Dydrogesterone and breast cancer risk in HRT
- Post-hysterectomy estrogen-only HRT outcomes
Connections
- Menopause: Why the Hormones Fall and What Changes — interactive animation
- Perimenopause Symptom Tracker and Hormonal Testing
- Perimenopause
- Depression
- Estradiol Formulations: Patch, Gel, Oral Routes
- HRT Risks: Breast Cancer, Clots and Stroke
- Testosterone Therapy for Women
- Vasomotor Symptoms: Hot Flashes and Night Sweats
- Genitourinary Syndrome of Menopause and Vaginal Estrogen
- Non-Hormonal Options: SSRIs, Gabapentin, Fezolinetant
- Bone Loss Prevention and HRT
- Insomnia
- Menopause and HRT
- Cardiovascular Disease
- Hormone Panel
- Anxiety
- Testosterone
- Osteoporosis
- Endometriosis