Estradiol Formulations: Patch, Gel, and Oral Routes
Not all estrogen is the same, and the route of delivery matters as much as the dose. The same molecule — estradiol — behaves very differently in your body depending on whether it goes through your skin, your mouth, or your bloodstream directly. If you only remember one thing from this page, remember this: transdermal estradiol (patch, gel, or spray) does not raise your clot risk the way oral estrogen does. That single fact has reshaped menopause medicine over the past fifteen years.
This article walks through every common estradiol product on the U.S. market, what a typical starting dose looks like, how to titrate up or down, how to switch between routes without losing symptom control, and why the North American Menopause Society (NAMS, now simply "The Menopause Society") and most modern prescribers now favor the skin over the stomach for most women. We will also cover three formulations you may see mentioned — conjugated equine estrogens (Premarin), ethinyl estradiol (the estrogen in birth control pills), and compounded "bioidentical" pellets — and explain where each fits, or does not fit, into modern practice.
This is a patient-facing explainer. None of it replaces a conversation with a clinician who knows your history, but it should leave you able to ask better questions and understand the answers.
Interactive Visualization Menopause — run the hormones down and set off a hot flash Empty the ovarian follicle pool and watch estradiol swing, then flatten, while FSH climbs — then trigger a hot flash and see the narrowed thermoneutral zone behind it. Launch →Table of Contents
- The Three Estrogens You Might Be Offered
- Why Transdermal Wins: The First-Pass Liver Effect
- The Patch: Vivelle-Dot, Climara, Estradot, Minivelle
- Gels and Sprays: Divigel, EstroGel, Elestrin, Evamist
- Oral Estradiol: Estrace and Generic 17-Beta-Estradiol
- Starting Dose and How to Titrate
- Switching Routes Without Losing Ground
- Absorption in Overweight and Obese Patients
- Cost, Insurance, and Why Not Pellets
- What NAMS and Major Societies Actually Say
- Key Research Papers
- PubMed Topic Searches
- Connections
- Featured Videos
The Three Estrogens You Might Be Offered
When a prescription label says "estrogen," it can mean one of three very different things. Knowing which one you are getting is the first step.
- 17-beta-estradiol. This is the exact molecule your ovaries made in your reproductive years — chemically identical, atom for atom. It is the "bioidentical" estrogen. It is FDA-approved, sold under dozens of generic and brand names (Estrace, Vivelle-Dot, Climara, Divigel, EstroGel, and more), and is the default modern choice.
- Conjugated equine estrogens (CEE, brand name Premarin). A mixture of about ten different estrogen compounds extracted from the urine of pregnant mares. It contains some estradiol metabolites plus equine-specific estrogens like equilin and equilenin that human bodies do not make and cannot perfectly clear. Premarin was the dominant menopause drug for fifty years, which is why it appears in almost every major older trial (including the Women's Health Initiative). It still works, but modern prescribing has largely moved on from it.
- Ethinyl estradiol. A synthetic estrogen engineered to survive digestion, used in oral contraceptives. It is roughly 100 times more potent per milligram than natural estradiol and has a much stronger effect on liver proteins, clotting factors, and blood pressure. It is not used for menopausal hormone therapy — the risk profile is wrong for an older population. If you are still on a low-dose birth control pill in your late 40s for cycle control, that is ethinyl estradiol; most clinicians transition you to estradiol-based HRT once periods stop.
For the rest of this article, "estradiol" means 17-beta-estradiol, the bioidentical form, unless we say otherwise.
Why Transdermal Wins: The First-Pass Liver Effect
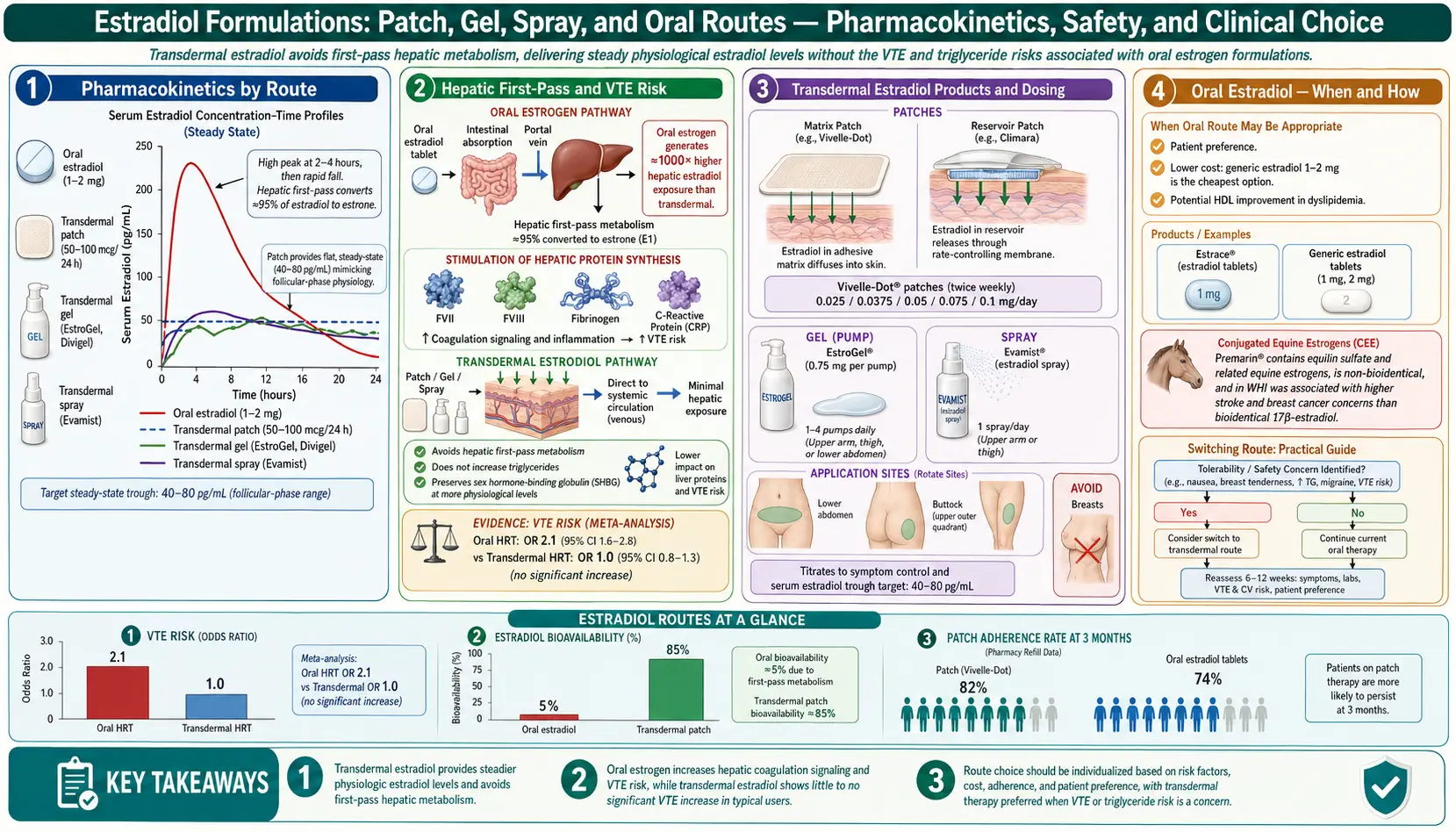
When you swallow an estradiol tablet, it is absorbed through your gut wall and carried by the portal vein directly into your liver before it reaches the rest of your body. The liver processes (and largely destroys) most of that first dose — this is the "first-pass effect." To deliver a useful amount of estradiol to your bloodstream, the oral dose has to be high enough that what survives is still meaningful. While the liver is doing all this work on a flood of estrogen, it changes how it makes several proteins:
- Clotting factors go up. Factors II, VII, IX, X, and fibrinogen all rise. This is the mechanism behind the increased venous thromboembolism (VTE) risk seen with oral estrogen. The landmark Canonico 2007 ESTHER study showed roughly four times the clot risk with oral estrogen compared to non-users, while transdermal users had no detectable increase over baseline.
- Triglycerides go up. Oral estrogen can push triglycerides 20–40% higher, occasionally enough to matter in women who already have high triglycerides or metabolic syndrome.
- Sex hormone binding globulin (SHBG) goes up sharply. SHBG is the protein that binds testosterone in your blood and keeps it inactive. An oral estrogen dose can double or triple SHBG, which drops your free testosterone and can worsen libido, energy, and mood. This is a common reason women feel "off" on oral HRT despite otherwise good symptom control.
- C-reactive protein goes up. Oral estrogen raises CRP independent of actual inflammation — another liver-protein quirk.
Estradiol absorbed through the skin skips all of this. It goes straight into your general circulation at low, steady concentrations, reaches the brain, bones, and blood vessels, and does not flood the liver. Clotting factors, triglycerides, and SHBG stay roughly where they were. That is the single biggest reason transdermal is the preferred route for most women today, and the specific reason it is strongly preferred if you have a history of clots, migraine with aura, obesity, high triglycerides, gallbladder disease, or a strong family clot history.
The Patch: Vivelle-Dot, Climara, Estradot, Minivelle
The estradiol patch is a small, clear or flesh-colored adhesive square that slowly releases 17-beta-estradiol through your skin over several days.
Common products and schedules:
- Vivelle-Dot and Minivelle — changed twice weekly (every 3–4 days). Small (roughly the size of a nickel or quarter). Doses: 0.025, 0.0375, 0.05, 0.075, 0.1 mg per day.
- Climara — changed once weekly. Larger patch. Same dose range.
- Estradot (Canada, UK, Europe) — very small twice-weekly patch, chemically similar to Vivelle-Dot.
- Alora — twice-weekly, similar profile.
- Combipatch — a twice-weekly patch combining estradiol with the progestin norethindrone; used in women with a uterus who want one-stop delivery. Note: this pairs transdermal estradiol with a synthetic progestin rather than micronized progesterone — see the progesterone vs progestins article for the trade-off.
Typical dose range: 0.025 to 0.1 mg per day. Most women land somewhere between 0.05 and 0.075 mg. A 0.025 mg patch is often enough for bone protection and mild symptoms; 0.05 mg is a common "full" starting dose for moderate hot flashes; 0.075 and 0.1 mg are reserved for women who are younger (surgical menopause, premature ovarian insufficiency) or who do not respond to standard doses.
Where to apply: Lower abdomen or upper buttock/hip, on clean, dry, hairless skin. Not on the breasts. Rotate sites with each change — do not put a new patch on the exact spot the old one was, or you will get skin irritation. Avoid the waistband area where clothing rubs the patch off. After a shower, pat the patch dry; it is designed to stay on through bathing, swimming, and exercise. If one falls off early, stick it back down or replace it and keep the same change-day schedule.
Skin reactions are the main downside — redness, itching at the site, occasional rash. Rotating sites aggressively usually solves this. A few women cannot tolerate any adhesive and need to move to gel or spray.
Gels and Sprays: Divigel, EstroGel, Elestrin, Evamist
If you hate patches or react to the adhesive, transdermal gels and sprays deliver the same estradiol through the skin in a different vehicle.
- Divigel — single-use foil packets (0.25, 0.5, 0.75, 1.0, 1.25 mg of estradiol per packet). Applied once daily to a 5-by-7-inch area on one upper thigh. Alternate thighs day to day.
- EstroGel — metered pump, 0.75 mg estradiol per pump. One or two pumps daily, applied to one arm from wrist to shoulder. Alternate arms.
- Elestrin — metered pump, 0.52 mg per pump. Applied to the upper arm.
- Evamist — a metered spray, 1.53 mg estradiol per spray. One to three sprays on the inner forearm once daily.
Typical dose range: Roughly 0.5 to 1.5 mg of estradiol per day transdermally via gel. Bloodstream levels achieved are comparable to a 0.025–0.075 mg patch.
Application rules that matter:
- Let the gel dry completely (a few minutes) before dressing or applying sunscreen.
- Wash hands thoroughly after applying.
- Do not let anyone else — especially children, pregnant partners, or pets — touch the application area until it has dried and you have covered it with clothing. Small but real transfer cases have been documented.
- Do not shower or swim for at least an hour after applying.
- Avoid sunscreen directly on the application site; some sunscreens increase estradiol absorption unpredictably.
Gels offer slightly more dose flexibility than patches (you can use half a packet, or one pump instead of two), which some women prefer for titration. The main drawbacks are price (see cost section below) and the daily ritual.
Oral Estradiol: Estrace and Generic 17-Beta-Estradiol
Oral 17-beta-estradiol is still a legitimate option — it is cheap, simple, and effective for symptom control. It just carries the first-pass liver effects described above.
- Estrace and generic estradiol tablets — 0.5, 1.0, and 2.0 mg. Typical doses: 1 mg daily for most women, 2 mg for stronger symptom control, 0.5 mg for low-dose maintenance.
- Premarin (conjugated equine estrogens) — 0.3, 0.45, 0.625, 0.9, and 1.25 mg. Typical dose 0.3–0.625 mg daily. Still covered by most insurance plans but decreasingly prescribed.
Oral may be a reasonable choice if: you have no personal or family history of clots; you are not obese; your triglycerides are normal; you do not have migraine with aura; you have tried transdermal and it did not give you symptom relief; or cost is the deciding factor (generic oral estradiol is pennies a day). Oral estrogen can also be slightly better at raising HDL cholesterol, though the clinical importance of this is debated.
Oral is a poor choice if: personal VTE history, strong family VTE history, known thrombophilia (Factor V Leiden, prothrombin mutation), migraine with aura, BMI over 30, high triglycerides, active gallbladder disease, or you rely on testosterone for libido/energy and cannot afford the SHBG bump.
Starting Dose and How to Titrate
There is no single "right" dose — the goal is the lowest dose that controls your symptoms and protects your bones. A typical titration plan for a newly menopausal woman starting transdermal estradiol:
- Weeks 1–4: Start at 0.05 mg/day patch (Vivelle-Dot or Climara) or equivalent gel (EstroGel one pump, Divigel 0.5–1.0 mg packet). If you have only mild symptoms or are over age 60 starting for the first time, begin at 0.025 mg.
- Weeks 4–8: Reassess. Track hot flash frequency, night sweats, sleep quality, mood, vaginal dryness, brain fog. A simple daily 1–5 rating works. See the symptom tracker article for a template.
- Weeks 8–12: If still symptomatic, step up one increment — 0.05 to 0.075, or 0.075 to 0.1. If symptoms are controlled but you feel over-estrogenized (breast tenderness, bloating, headaches, spotting), step down.
- Months 3–6: Most women find a stable dose. Reassess annually with your clinician.
Add progesterone if you still have a uterus. Unopposed estrogen thickens the uterine lining and raises endometrial cancer risk. Micronized progesterone (Prometrium) 100 mg nightly continuous or 200 mg nightly for 12 days per month is the preferred partner — see the progesterone comparison.
Blood level testing is usually unnecessary. Estradiol serum levels on transdermal therapy do loosely correspond to symptom relief (typically 40–100 pg/mL on a 0.05–0.1 mg patch), but they fluctuate. Treat the patient, not the number. Testing is useful when symptoms are not responding at an apparently adequate dose — it can catch a poor absorber. See the hormone panel lab test page.
Switching Routes Without Losing Ground
Women switch routes for lots of reasons — insurance changes, skin reactions, new clot-risk information, travel convenience, or just curiosity about whether one will feel better than the other. Rough equivalencies your prescriber will use:
- Oral estradiol 1 mg/day ≈ 0.05 mg/day patch ≈ 0.5–1.0 mg/day gel ≈ Premarin 0.625 mg/day.
- Oral estradiol 2 mg/day ≈ 0.1 mg/day patch ≈ 1.5 mg/day gel ≈ Premarin 1.25 mg/day.
How to do the switch: Stop the old route on day 1 and start the new route on day 1 — no taper overlap needed. If switching from patch to gel, apply the first gel dose on the morning you would have changed your patch. If switching from oral to patch, apply the first patch the morning after the last pill. Expect a brief 1–2 week adjustment where symptoms may flare slightly as steady-state shifts. Recheck at 4–6 weeks and titrate if needed.
One note on the oral-to-transdermal switch: your SHBG will fall back toward baseline over 4–8 weeks, which raises free testosterone. If you were on oral HRT and felt flat or low-libido, you may feel the switch within a month. Conversely, switching from transdermal to oral can unmask a testosterone drop you did not realize was coming — something to watch for.
Absorption in Overweight and Obese Patients
Transdermal estradiol absorption varies with body fat and skin characteristics. A few real-world points:
- Patches may underdeliver in women with higher BMI — thicker subcutaneous fat under the adhesion site can slow movement of estradiol into capillary circulation. Some women with BMI over 30 need 0.075 or 0.1 mg patches to get the symptom control a leaner woman gets from 0.05 mg.
- Gel tends to be more consistent across body sizes because it is applied over a wider, thinner-skin area (arm or thigh) where vascularity is predictable.
- Abdomen vs hip placement matters. In women with abdominal obesity, a lower abdominal patch may absorb less reliably than an upper hip or buttock placement. If you are not getting relief, try rotating the patch site to the hip for a cycle.
- Oral is NOT the answer for absorption problems in obese patients. Obesity itself is a VTE risk factor, and adding oral estrogen stacks risk on risk. The correct fix is a higher transdermal dose or a switch to gel.
Cost, Insurance, and Why Not Pellets
Costs vary dramatically by product. Ballpark U.S. retail with GoodRx or similar discount programs (2025–2026 range):
- Generic oral estradiol 1 mg — $5–$15 per month. Cheapest option by far.
- Generic estradiol patch (twice weekly) — $15–$45 per month. Widely covered by insurance, often $0–$20 copay.
- Brand-name patch (Vivelle-Dot, Climara, Minivelle) — $80–$200 per month without insurance. Usually a $30–$60 copay with coverage.
- Divigel / EstroGel / Elestrin — $80–$250 per month retail. Insurance coverage varies; prior authorization is common.
- Evamist spray — similar to gels, often $150–$300 per month retail.
- Premarin — $150–$300 per month retail, though many plans cover it with a modest copay.
If cost is the deciding factor, generic oral estradiol or a generic patch is almost always the answer. Many compounding pharmacies offer "custom" transdermal creams at comparable prices to branded gels, but these are not FDA-approved and deliver unpredictable doses.
Why compounded pellets are NOT recommended. Estradiol and testosterone pellets — small drug implants inserted under the skin of the hip every 3–4 months — are heavily marketed by some clinics as "bioidentical hormone replacement." The estradiol in pellets is the same 17-beta-estradiol as in a patch, so "bioidentical" is technically true; that is not the problem. The problems are:
- Pellets deliver supraphysiologic doses — often estradiol levels 2–5x higher than a premenopausal woman's own ovaries produced. These high levels are associated with more breast tenderness, spotting, and unknown long-term breast and endometrial safety.
- You cannot stop a pellet. If you have a side effect, you ride it out for months until the pellet dissolves.
- They are not FDA-approved for menopause. The Menopause Society, the Endocrine Society, and the American College of Obstetricians and Gynecologists all explicitly advise against them.
- Cost is high — typically $300–$800 every 3–4 months, rarely covered by insurance, on top of the procedure fee.
If a clinic is selling you pellets as "safer" or "more natural" than a patch, they are selling you something that is neither. A cheap generic patch plus micronized progesterone is the modern standard for a reason.
What NAMS and Major Societies Actually Say
The North American Menopause Society 2022 Hormone Therapy Position Statement (and its 2023 update) is the most widely cited guideline document in the English-speaking world. Its core points on route selection:
- For most women under 60 or within 10 years of menopause, the benefits of HRT outweigh the risks.
- Transdermal estradiol is preferred over oral in women with elevated VTE risk (obesity, personal or family clot history, thrombophilia, migraine with aura, active gallbladder disease, hypertriglyceridemia).
- Transdermal is "reasonable first-line" even in women without these risk factors, reflecting the cleaner liver profile.
- There is no required maximum duration of HRT. Decisions to continue past age 65 are individualized, not automatic.
- Compounded hormone therapy — including pellets and custom creams — is not recommended over FDA-approved products for routine use.
The Endocrine Society, ACOG, and the International Menopause Society all publish parallel guidance that says essentially the same thing. The 2002 Women's Health Initiative scare — which used oral conjugated equine estrogens plus medroxyprogesterone acetate in women averaging 63 years old — is no longer considered representative of modern transdermal regimens in appropriately selected women. See the HRT risks article for a full discussion of what the WHI does and does not tell us in 2026.
Key Research Papers
- Canonico M, et al. Hormone therapy and venous thromboembolism among postmenopausal women: impact of the route of administration and progestogens: the ESTHER study. Circulation. 2007. The landmark paper showing oral HRT raises VTE risk roughly 4-fold while transdermal HRT does not.
- The 2022 Hormone Therapy Position Statement of The North American Menopause Society. Menopause. 2022. Current U.S. guidance on HRT including explicit preference for transdermal in higher-risk patients.
- Search PubMed Meta-analysis confirming the route-specific VTE and stroke difference.
- PubMed search: transdermal estradiol, first-pass metabolism, and SHBG. Background on why oral estrogen doubles SHBG and lowers free testosterone.
- PubMed search: compounded bioidentical hormone pellets, safety review. Literature supporting why major societies advise against pellet therapy.
- PubMed search: conjugated equine estrogens vs 17-beta-estradiol comparative outcomes.
PubMed Topic Searches
- Transdermal estradiol and venous thromboembolism
- Oral vs transdermal estrogen in menopause
- Estradiol patch dose titration for vasomotor symptoms
- Estradiol gel pharmacokinetics (Divigel, EstroGel)
- Transdermal estradiol absorption in obesity
- Conjugated equine estrogens and cardiovascular outcomes
- Estradiol route, SHBG, and free testosterone
- Compounded hormone pellets in menopause
- NAMS/Menopause Society hormone therapy position statements
- Oral estradiol, triglycerides, and first-pass hepatic metabolism
Connections
- Menopause: Why the Hormones Fall and What Changes — interactive animation
- HRT Risks: Breast Cancer, Clots and Stroke
- Hormone Panel
- Perimenopause Symptom Tracker and Hormonal Testing
- Micronized Progesterone vs Synthetic Progestins
- Testosterone Therapy for Women
- Vasomotor Symptoms: Hot Flashes and Night Sweats
- Genitourinary Syndrome of Menopause and Vaginal Estrogen
- Non-Hormonal Options: SSRIs, Gabapentin, Fezolinetant
- Bone Loss Prevention and HRT
- Perimenopause
- Menopause
- Cardiovascular Disease
- Menopause and HRT
- Testosterone
- Gallbladder Disease
- Migraine
- Vitamin D3
- Vitamin K
- Osteoporosis