Bone Loss Prevention & HRT
Estrogen is the single most important hormone regulating your skeleton. When it falls at menopause, bone loss accelerates quickly — and for many women, that accelerated loss is the first event that will eventually cause a fracture in their seventies or eighties. This page walks through why that happens, what hormone therapy (HRT) does to stop it, how HRT compares to the drugs osteoporosis specialists usually reach for (bisphosphonates and denosumab), and how to decide whether HRT should be your bone strategy, part of your strategy, or not the right fit.
This is a patient-facing guide. It is rigorous about numbers and studies, but written for you, not a rheumatology fellow.
Interactive Visualization Menopause — run the hormones down and set off a hot flash Empty the ovarian follicle pool and watch estradiol swing, then flatten, while FSH climbs — then trigger a hot flash and see the narrowed thermoneutral zone behind it. Launch →Table of Contents
- Why Menopause Accelerates Bone Loss
- What the WHI Actually Showed for Bone
- The FDA Indication People Forget About
- Who Is a Candidate for HRT-First Bone Strategy
- Effective Doses — Low-Dose Transdermal Works
- HRT vs Bisphosphonates vs Denosumab
- What Happens When You Stop HRT
- Calcium, Vitamin D, K2, and Protein
- Resistance Training and Impact Exercise
- DEXA Intervals and the FRAX Score
- Key Research Papers
- PubMed Topic Searches
- Connections
- Featured Videos
Why Menopause Accelerates Bone Loss
Bone is living tissue. All through adulthood, small crews of cells called osteoclasts chew away old bone while osteoblasts lay down new bone behind them. As long as the two crews are balanced, your bones stay the same density. Estrogen is one of the referees that keeps them balanced.
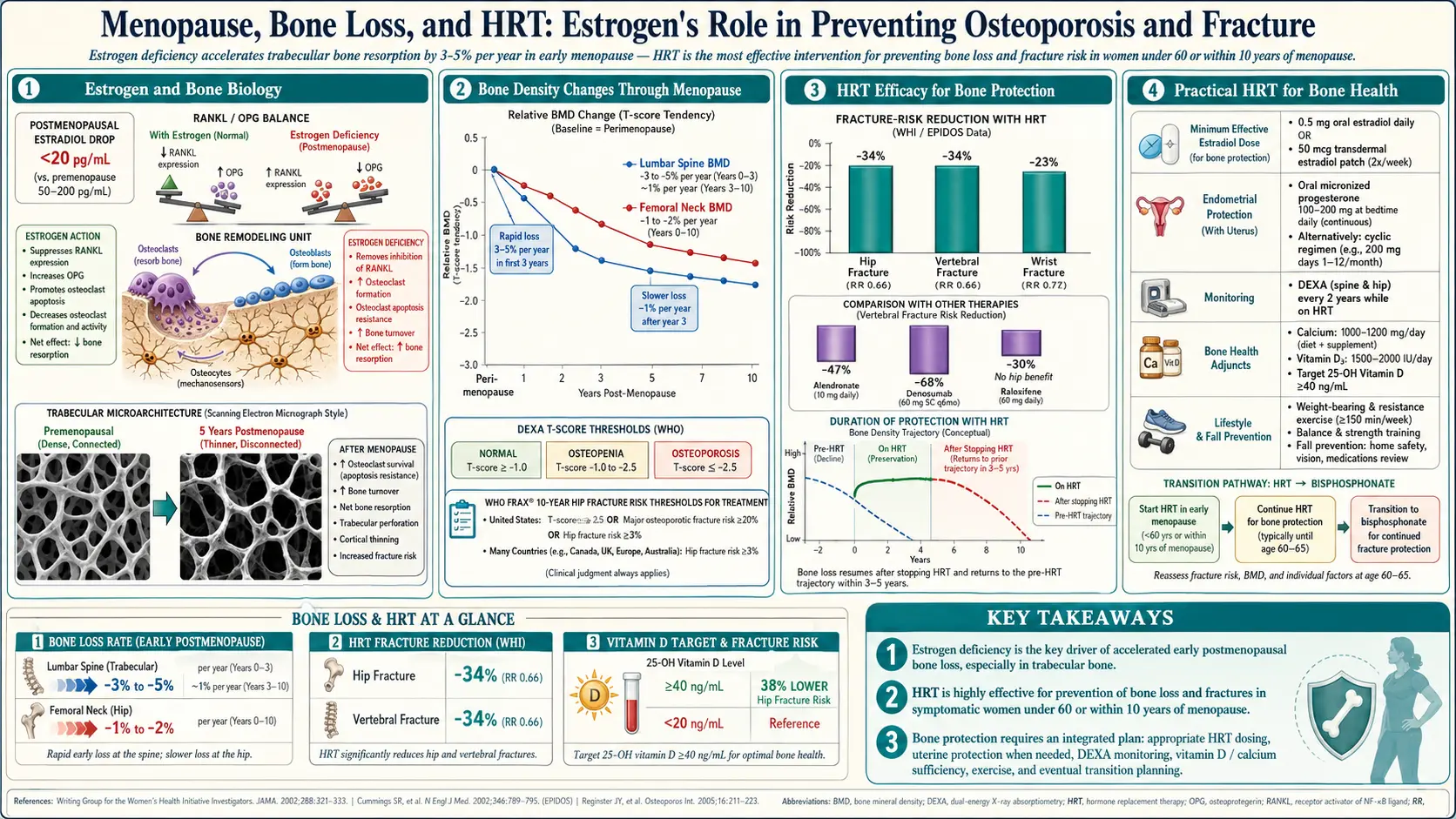
Estrogen works largely through a pair of signalling molecules called RANKL (which tells osteoclasts to form and start dissolving bone) and OPG (which blocks RANKL and protects bone). When estrogen is high, OPG is high and osteoclast activity is restrained. When estrogen falls at menopause, RANKL shoots up relative to OPG, osteoclasts become over-active, and bone is dissolved faster than it can be rebuilt.
The practical result: during the first 5–10 years after your final period, most women lose bone mineral density (BMD) at roughly 1–3% per year at the spine and 1–2% per year at the hip. In the first 1–2 years after menopause, trabecular (spongy) bone in the spine can lose as much as 5% in a single year. By age 70, a woman who never used HRT has typically lost 25–30% of her peak bone mass. That is the trajectory that turns into hip fractures at 80.
What the WHI Actually Showed for Bone
The Women's Health Initiative (WHI) is famous for bad news about HRT. Its bone results were almost the opposite — and are often under-reported to the women who could most benefit.
In the estrogen-plus-progestin arm (Rossouw 2002 and Cauley 2003), HRT produced:
- 34% reduction in hip fracture (hazard ratio 0.66).
- 34% reduction in clinical vertebral fracture (HR 0.66).
- 24% reduction in total fractures (HR 0.76).
These were not post-hoc fishing-expedition results. They were prespecified endpoints, statistically significant, and consistent with decades of observational data. Importantly, the fracture benefit appeared in average-risk postmenopausal women — not just women already diagnosed with osteoporosis. No other medication class has shown a hip-fracture reduction in healthy postmenopausal women with normal baseline BMD.
The estrogen-alone arm (for women without a uterus) showed similar fracture reductions with a cleaner safety profile — no increase in breast cancer during the trial, and a reduction in breast cancer that has persisted in long-term follow-up.
The FDA Indication People Forget About
One of the official FDA-approved indications for systemic estrogen in the United States is prevention of postmenopausal osteoporosis. That label has been in place since the 1980s and has never been withdrawn. It sits right alongside the indication for vasomotor symptoms.
Yet if you walk into a primary care office and ask for estrogen specifically to protect your bones, many clinicians still react as if you are asking for something off-label or risky. The North American Menopause Society (NAMS) 2022 position statement explicitly supports HRT for osteoporosis prevention in appropriate candidates, and both the Endocrine Society and the International Menopause Society agree. If your doctor pushes back, the NAMS statement is the document to cite.
Who Is a Candidate for HRT-First Bone Strategy
HRT is the preferred bone drug for women who meet all of the following:
- Under age 60 at the time of initiation, and
- Within 10 years of their final menstrual period (the "timing hypothesis" window), and
- Also experiencing vasomotor symptoms (hot flashes, night sweats), genitourinary symptoms (vaginal dryness, urinary urgency), sleep disruption, mood changes, or joint aches — so HRT is doing multiple jobs at once, and
- No contraindications (see the HRT risks page): no active or prior estrogen-sensitive breast cancer, no prior unprovoked blood clot or stroke, no active liver disease, no undiagnosed vaginal bleeding.
If you fit that profile, HRT does five or six useful things at once. Starting a bisphosphonate in a 52-year-old woman with hot flashes and early bone loss is a strangely narrow choice when estrogen would treat the bone and the flashes and the vaginal symptoms and possibly reduce cardiovascular risk.
Women who are 60 or older, more than 10 years past menopause, have established osteoporosis (T-score ≤ –2.5), or have already had a fragility fracture are usually better served starting with a bisphosphonate or denosumab — those drugs have the direct fracture-reduction RCT data in that population, and HRT is no longer recommended for initiation in women past the 10-year window.
Effective Doses — Low-Dose Transdermal Works
You do not need high-dose estrogen to protect bone. The bone-sparing dose is lower than the dose many women used in the 1990s for symptom control.
- Transdermal estradiol patch 0.025–0.05 mg/day changed twice weekly — the best-studied and generally preferred route. Gambacciani and colleagues (2008) and multiple follow-on trials showed that even the 0.025 mg patch produces meaningful BMD gains at the spine and hip over 1–2 years.
- Estradiol gel 0.5–1.0 mg/day or spray — comparable bone effect to the patch.
- Oral estradiol 1 mg/day — effective, but first-pass liver metabolism raises clotting factors; transdermal routes are preferred for most women, especially with any cardiovascular risk (see the estradiol formulations page).
If you still have a uterus, you must pair estrogen with a progestogen to protect the endometrium. For most women that means micronized progesterone 100 mg nightly (continuous) or 200 mg nightly for 12 days/month (cyclic). Micronized progesterone has a better safety profile than older synthetic progestins — detail on the progesterone vs progestins page.
Typical BMD response on a 0.05 mg patch plus adequate calcium and vitamin D: +2 to +5% at the spine and +1 to +3% at the hip over 2 years, compared with a 2–6% loss on placebo over the same interval. That is a 4–11 percentage-point swing — clinically equivalent to what a bisphosphonate achieves over the same period.
HRT vs Bisphosphonates vs Denosumab
Head-to-head, the drug classes look more similar than marketing suggests.
BMD effect (prevention of bone loss in healthy early-postmenopausal women): HRT and bisphosphonates (alendronate 5–10 mg/day or 70 mg/week, risedronate, zoledronic acid) produce roughly comparable spine and hip BMD gains over 1–3 years. Studies that have randomized women directly between the two (EPIC trial and others) show either similar gains or a slight edge to HRT at the spine.
Fracture reduction (treatment of established osteoporosis): Bisphosphonates have the larger and more recent RCT database in women with T-score ≤ –2.5 or prior vertebral fracture — alendronate, risedronate, and zoledronic acid all reduce vertebral fractures by roughly 40–70% and hip fractures by 30–50%. Denosumab (60 mg subcutaneously every 6 months) produces even larger BMD gains and similar fracture reductions, but it has a dangerous rebound: if you miss a dose or stop without transitioning to a bisphosphonate, vertebral fractures can cluster within 6–18 months.
The practical choice matrix:
- Age 50–59, recently menopausal, T-score –1.0 to –2.4, plus hot flashes: HRT first.
- Age 50–59, recently menopausal, no symptoms, T-score borderline: HRT or bisphosphonate — reasonable either way.
- Age 65+, T-score ≤ –2.5, or prior fragility fracture: bisphosphonate (oral alendronate or yearly zoledronic acid IV) first-line. Denosumab if bisphosphonate-intolerant, but plan an exit strategy.
- Very high risk (T-score ≤ –3.0, recent vertebral fracture): consider anabolic therapy first (teriparatide, abaloparatide, or romosozumab), then transition to a bisphosphonate or denosumab.
What Happens When You Stop HRT
This is the catch. HRT protects bone only while you take it. When estrogen is withdrawn, the RANKL/OPG balance tips back, osteoclasts fire up again, and bone loss resumes at roughly the same rapid pace as natural menopause — about 1–3% per year at the spine and hip for the first few years off therapy. Within 3–5 years of stopping, most of the BMD you gained is lost.
Two practical implications:
- If bone protection is a major reason you are on HRT, stopping casually at age 60 "because of the WHI" is not a harmless choice — you are giving up the benefit and accepting rapid catch-up bone loss.
- If you do decide to taper off, your doctor should consider transitioning you onto a bisphosphonate (e.g. yearly zoledronic acid, or 3–5 years of oral alendronate) to lock in the BMD gains. This is analogous to the now-standard practice of transitioning off denosumab onto a bisphosphonate.
Many current menopause specialists are comfortable continuing HRT well past age 60 or even 65 in healthy low-risk women who are benefiting — the 2022 NAMS position statement explicitly endorses continued use based on ongoing risk–benefit review rather than an arbitrary stop age. Talk to your prescriber about a plan rather than a deadline.
Calcium, Vitamin D, K2, and Protein
No drug works well on a depleted foundation. The nutrition baseline for any bone strategy:
- Calcium 1,000–1,200 mg/day, food preferred. Dairy (yogurt 300 mg/cup, milk 300 mg/cup, hard cheese 200 mg/oz), sardines or canned salmon with bones (300–350 mg/can), tofu set with calcium (250–350 mg per ½ cup), collard and turnip greens (250–270 mg/cup cooked), almonds (75 mg/oz), fortified plant milks. Aim to get most from food. High-dose calcium supplements — especially single 1,000 mg pills — have been linked in some analyses to increased cardiovascular and kidney-stone risk; food calcium has not.
- Vitamin D3 800–2,000 IU/day, adjusted to achieve a 25-hydroxy-vitamin-D blood level of 30–50 ng/mL. Heavier bodies, darker skin, and northern latitudes often need the top of that range. See the Vitamin D3 page.
- Vitamin K2 (menaquinone-7) 100–200 mcg/day. K2 activates osteocalcin, which directs calcium into bone matrix rather than arterial walls. Evidence is strongest from Japanese studies using MK-4 at pharmacologic doses; MK-7 at supplement doses shows smaller but consistent BMD benefits. See the Vitamin K page.
- Protein 1.0–1.2 g/kg/day. A 68 kg (150 lb) woman needs 68–82 g of protein per day, spread across meals. Bone is roughly half protein by volume; under-eating protein in your sixties and seventies is one of the strongest predictors of hip fracture, independent of calcium.
- Magnesium 300–400 mg/day, primarily from leafy greens, nuts, seeds, and whole grains. Magnesium is required for vitamin D activation and PTH regulation.
Caffeine above ~400 mg/day, heavy alcohol (≥2 drinks/day), and smoking all measurably accelerate bone loss.
Resistance Training and Impact Exercise
Bone responds to mechanical load. Walking is good for your heart and your mood; it does relatively little for your spine and hip BMD. What moves bone density is loading that exceeds what the bone is used to.
- Progressive resistance training 2–3 days/week. Squats, deadlifts, overhead press, row, lunges — compound movements with increasing weight over time. The LIFTMOR trial (Watson 2018) used heavy resistance (80–85% of one-rep max) in postmenopausal women with low bone mass and produced spine BMD gains of ~3% in 8 months. "Heavy" is safe and effective when taught properly.
- Impact exercise 3–5 days/week. Jumping (10–50 low hops per day), skipping, hopping, step-down drills, and running all load the hip in a way walking does not. Even 10 multidirectional hops a day, done consistently, produces measurable femoral-neck BMD gains.
- Balance and fall prevention. Most hip fractures happen because someone falls, not because bone collapsed on its own. Single-leg stance, tandem walking, tai chi, and targeted ankle and hip stabilizer work reduce fall rate by 20–40%.
- Avoid aggressive spinal flexion if you already have low spine BMD. Full sit-ups, toe-touches, and loaded forward-bending can crush-fracture weakened vertebrae. Extension-biased work (glute bridges, prone back extensions, farmer's carries) is safer and more useful.
DEXA Intervals and the FRAX Score
DEXA (dual-energy X-ray absorptiometry) is the standard bone density scan. It takes 10 minutes, uses a trivial amount of radiation, and reports two numbers per site (spine, hip, sometimes forearm):
- T-score: standard deviations from the average young adult peak bone mass. −1.0 to −2.4 is osteopenia; ≤−2.5 is osteoporosis.
- Z-score: standard deviations from the average person your age and sex. Useful for younger women and men to flag unexpected loss that warrants a secondary workup.
Full detail on how to read your results is on the DEXA T-score and Z-score explained page.
Screening intervals:
- Baseline DEXA at menopause or age 50 if you have risk factors (family history of hip fracture, low body weight <127 lb, smoking, early menopause before 45, long-term glucocorticoids, celiac or IBD, hyperthyroidism). Otherwise, baseline at age 65.
- Repeat every 2 years while on treatment or during the rapid-loss early-menopause window.
- Extend to every 3–5 years once BMD is stable and in the normal range.
FRAX score: the WHO fracture-risk calculator (available free at frax.shef.ac.uk) estimates your 10-year probability of a major osteoporotic fracture and of hip fracture specifically, using your age, sex, weight, height, prior fracture, parental hip fracture, smoking, alcohol, glucocorticoid use, rheumatoid arthritis, and (optionally) femoral-neck BMD. U.S. treatment thresholds are usually ≥20% for major osteoporotic fracture or ≥3% for hip fracture — above those numbers, pharmacologic therapy is recommended regardless of T-score.
Key Research Papers
- Cauley JA, et al. Effects of estrogen plus progestin on risk of fracture and bone mineral density: the Women's Health Initiative randomized trial. JAMA. 2003;290(13):1729–1738.
- Rossouw JE, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women's Health Initiative randomized controlled trial. JAMA. 2002;288(3):321–333.
- The 2022 Hormone Therapy Position Statement of The North American Menopause Society. Menopause. 2022;29(7):767–794.
- Gambacciani M, Ciaponi M, Cappagli B, et al. Effects of low-dose, continuous combined hormone replacement therapy on sleep in symptomatic postmenopausal women and low-dose transdermal estradiol on bone. Maturitas. 2008.
- Watson SL, et al. High-Intensity Resistance and Impact Training Improves Bone Mineral Density and Physical Function in Postmenopausal Women With Osteopenia and Osteoporosis: The LIFTMOR Randomized Controlled Trial. J Bone Miner Res. 2018;33(2):211–220.
- Eastell R, et al. Pharmacological Management of Osteoporosis in Postmenopausal Women: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2019;104(5):1595–1622.
PubMed Topic Searches
For further reading, these PubMed searches return current peer-reviewed work on HRT and bone:
- Hormone therapy and postmenopausal bone mineral density
- Transdermal estradiol and bone density
- WHI, hip fracture, estrogen, and progestin
- Estrogen, RANKL, OPG, and osteoclast regulation
- HRT vs bisphosphonate head-to-head bone trials
- Bone loss after stopping hormone therapy
- Resistance training and postmenopausal bone density
- FRAX score and treatment thresholds
- Vitamin K2 (menaquinone) and bone density
Connections
- Reproductive Medicine
- Menopause: Why the Hormones Fall and What Changes — interactive animation
- Estradiol Formulations: Patch, Gel, Oral Routes
- HRT Risks: Breast Cancer, Clots and Stroke
- Vitamin D3
- Vitamin K
- Micronized Progesterone vs Synthetic Progestins
- DEXA Scan: T-Score and Z-Score Explained
- Calcium
- Osteoporosis
- Testosterone Therapy for Women
- Vasomotor Symptoms: Hot Flashes and Night Sweats
- Genitourinary Syndrome of Menopause and Vaginal Estrogen
- Non-Hormonal Options: SSRIs, Gabapentin, Fezolinetant
- Perimenopause Symptom Tracker and Hormonal Testing
- Menopause and HRT
- Calcium, Vitamin D and Protein Intake
- Bisphosphonates: Alendronate, Risedronate, Zoledronate
- Magnesium
- Perimenopause
- Menopause — the estrogen loss that starts the rapid bone-loss window described here.