Testosterone Therapy for Women
Testosterone is usually framed as a male hormone, but women make it too — and they need it. Ovaries and adrenal glands produce small amounts throughout a woman's life, and circulating total testosterone sits in a range roughly one-tenth of a man's. That small amount powers libido, energy, muscle maintenance, bone density, and mood stability. Between the ages of 20 and 40, a woman's circulating androgen levels fall by about 50%, driven mostly by declining adrenal DHEA production. Natural menopause drops levels further, and surgical removal of both ovaries (bilateral oophorectomy) cuts testosterone roughly in half overnight.
When symptoms of low testosterone become disruptive — most consistently, a distressing loss of sexual desire — carefully dosed testosterone replacement can help. The current evidence base, summarized in the 2019 Global Consensus Position Statement, supports one indication only: Hypoactive Sexual Desire Disorder (HSDD) in postmenopausal women. Use for energy, mood, muscle tone, and cognition is common in practice but rests on thinner evidence and requires honest informed consent.
This article walks through who is actually a candidate, what products clinicians prescribe (and why there is still no FDA-approved female testosterone product in the U.S.), how to dose safely, what to monitor, and which delivery forms — particularly compounded pellets — to avoid.
Interactive Visualization Menopause — run the hormones down and set off a hot flash Empty the ovarian follicle pool and watch estradiol swing, then flatten, while FSH climbs — then trigger a hot flash and see the narrowed thermoneutral zone behind it. Launch →Table of Contents
- Why Female Testosterone Matters
- The Only Approved Indication: HSDD
- Off-Label Use for Energy, Mood, and Muscle
- Products and Dosing — The U.S. Workaround
- Why to Avoid Compounded Pellets
- Monitoring: Labs, Schedule, and Targets
- Side Effects and Red Flags
- Why DHEA Is Not a Reliable Substitute
- Regulatory History: Intrinsa and the Pellet Lawsuits
- Key Research Papers
- PubMed Topic Searches
- Connections
- Featured Videos
Why Female Testosterone Matters
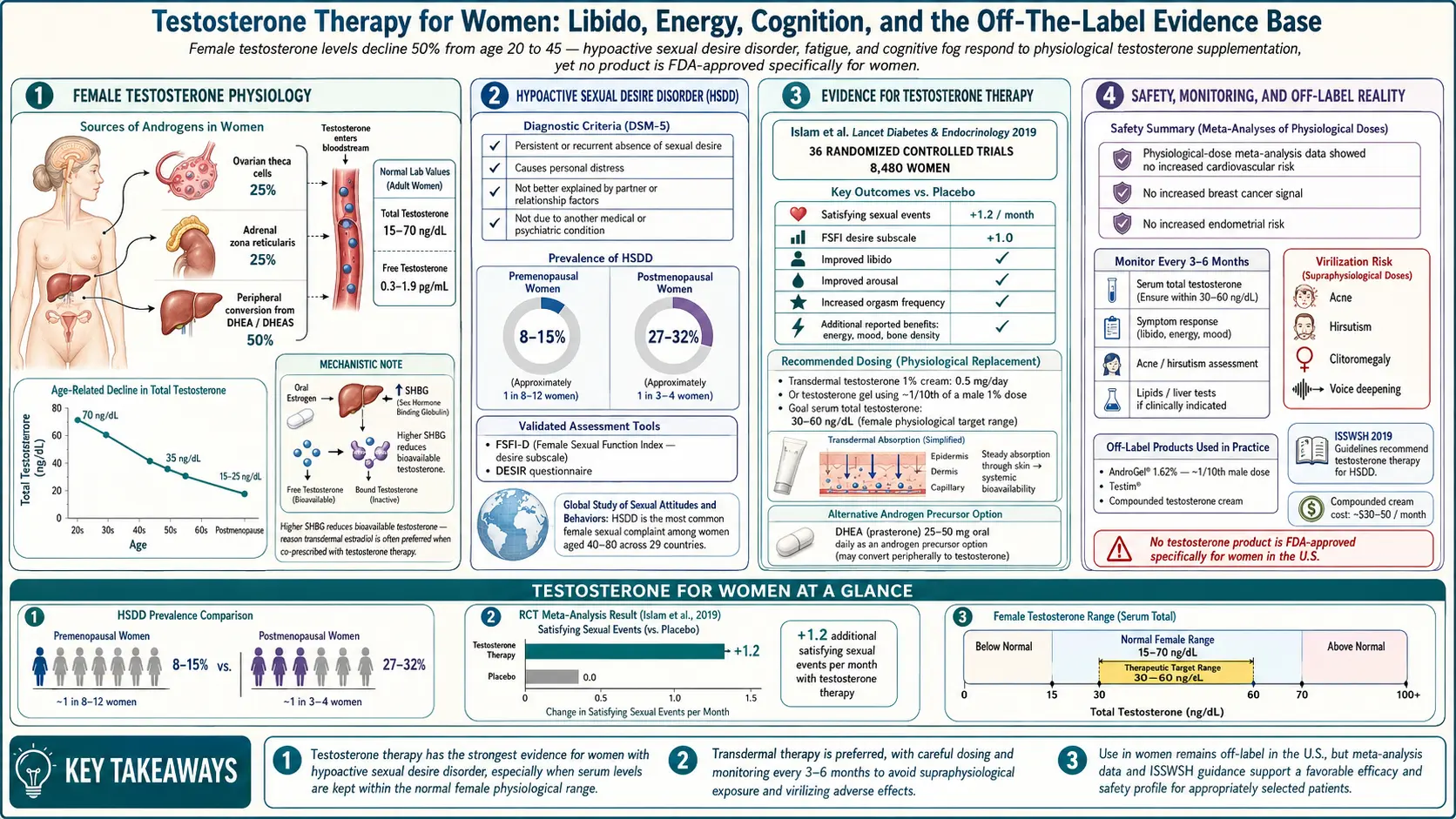
A healthy young woman's total testosterone usually runs 20–70 ng/dL, with free testosterone around 0.3–1.9 pg/mL. About half comes from the ovaries (both direct testosterone secretion and conversion from ovarian precursors) and half from the adrenal glands via DHEA and androstenedione. Unlike estrogen, which drops off a cliff at menopause, testosterone declines gradually over decades. By the time a woman reaches 40, her androgen pool is roughly half of what it was at 20.
Two events accelerate the decline:
- Natural menopause reduces ovarian output further, but postmenopausal ovaries keep producing some androgens for years. Women who enter menopause later and keep their ovaries often maintain better testosterone levels than those who do not.
- Bilateral oophorectomy (surgical removal of both ovaries) abruptly eliminates the ovarian contribution. Circulating testosterone falls by roughly 50% within days. Women who have this surgery before natural menopause often describe a profound drop in libido, energy, and sense of well-being that standard estrogen replacement does not fully fix.
Testosterone in women influences:
- Sexual desire, arousal, and orgasm frequency. The most robust clinical effect.
- Muscle mass and strength. Modest but measurable effects on lean body mass.
- Bone density. Likely contributes alongside estrogen; see Bone Loss Prevention and HRT.
- Mood and energy. Often reported by patients, less consistently demonstrated in trials.
- Cognition. Evidence is weak and inconsistent.
The Only Approved Indication: HSDD
The Global Consensus Position Statement on the use of testosterone therapy for women, published in 2019 and endorsed by eleven major menopause and endocrine societies worldwide, concluded that the only evidence-based indication is Hypoactive Sexual Desire Disorder (HSDD) in postmenopausal women.
HSDD is a clinical diagnosis with three components:
- Persistent or recurrent absence of sexual thoughts, fantasies, or desire for sexual activity.
- The change causes personal distress or relationship strain. (Low desire without distress is not a disorder.)
- Other causes — depression, relationship conflict, medications (especially SSRIs), untreated thyroid or estrogen deficiency, pelvic pain, genitourinary syndrome of menopause — have been considered and addressed.
That last point matters. Before a testosterone trial, a clinician should treat estrogen deficiency and vaginal dryness (see GSM and Vaginal Estrogen), review antidepressants that blunt libido, and screen for depression and relationship factors. Testosterone helps the woman whose estrogen is already optimized and whose desire is still missing.
The consensus statement explicitly does not recommend testosterone for premenopausal women, for general well-being, for cognition, or for "anti-aging." It also does not endorse blood-testosterone levels as a diagnostic criterion — HSDD is diagnosed clinically, and many women with low desire have "normal" lab values.
Off-Label Use for Energy, Mood, and Muscle
In practice, many clinicians — especially in menopause-focused and "hormone optimization" clinics — prescribe testosterone for symptoms beyond HSDD: fatigue, brain fog, depressed mood, loss of muscle tone, and waning motivation. Some women describe a genuine improvement on low-dose therapy; others do not.
The honest summary of the evidence:
- Energy and mood: Randomized trials show a small average effect that barely separates from placebo. A responsive subset probably exists but is hard to predict up front.
- Muscle and body composition: At physiologic female replacement doses, lean mass gains are modest (on the order of 1–2 pounds over 6–12 months). Supraphysiologic doses produce more muscle but also virilizing side effects.
- Cognition and memory: Conflicting trial results. Do not expect dramatic improvement.
- Bone density: Likely a modest additive benefit on top of estrogen, but estrogen remains the dominant driver.
Off-label prescribing is legal and common, but a good clinician will say out loud: "We are trying this based on biological plausibility and your symptoms, not on strong trial evidence. We will reassess in three to six months, and if you are not clearly better, we will stop."
Products and Dosing — The U.S. Workaround
There is currently no FDA-approved testosterone product for women in the United States. Every woman on testosterone therapy in the U.S. is using either a male product at a fraction of the male dose, or a compounded preparation made by a specialty pharmacy. Australia has an approved 1% cream (AndroFeme) at a female dose; the U.K. uses a testosterone gel (Tostran/Testogel) off-label. U.S. clinicians work with three practical options:
- Compounded testosterone 1% cream, 0.5 g daily. This delivers roughly 5 mg of testosterone per day, which is the dose most closely matching AndroFeme and the trial literature. Applied to the inner thigh, outer arm, or lower abdomen — rotating sites. This is the most commonly prescribed U.S. option and is the closest thing to "standard of care." Cost: $30–$80/month from compounding pharmacies.
- AndroGel 1% or Testim (male products), tiny dose. A 1% gel delivers 10 mg per 1 g of product, so women use roughly 0.5 g (half a pump, or a pea-sized amount) daily — about one-tenth of a man's starting dose. Advantage: FDA-manufactured, same quality control as any brand drug. Disadvantage: not designed for this use, awkward measuring, insurance often denies for female patients.
- Compounded testosterone troches (lozenges) or sublingual drops. Less predictable absorption than transdermal. Generally a second-line option if skin reactions rule out creams.
Avoid testosterone injections (too much bump in level for female physiology), oral methyltestosterone (liver toxicity, adverse lipid effects), and — as detailed in the next section — testosterone pellets.
A realistic starting protocol. Compounded 1% testosterone cream, 0.5 g applied to the inner thigh every morning. Baseline labs first (total testosterone, free testosterone, SHBG, CBC, lipid panel). Recheck testosterone levels at 3–6 weeks to confirm the dose is in range, then every 6 months. Reassess symptoms at 3 months — if no meaningful improvement in libido (for HSDD) or energy/well-being (off-label) by 6 months, taper and stop.
Why to Avoid Compounded Pellets
Testosterone pellets — small crystalline implants inserted under the skin of the hip or buttock every 3–4 months — are heavily marketed in the U.S. under brand names like BioTE. They are convenient (no daily routine), and cash-pay clinics love them because each insertion is a billable procedure.
The problems are real:
- Non-physiologic peaks. Pellets deliver a high initial surge that can push testosterone well above the female reference range for weeks. Supraphysiologic levels cause the side effects discussed below and are associated with higher discontinuation rates.
- No off-switch. If a woman develops acne, scalp hair loss, voice changes, or clitoral enlargement, the pellet cannot be removed easily. She has to wait months for the hormone to wear off. A cream can be stopped the same day.
- Unregulated compounding. Pellet dosing varies from pharmacy to pharmacy. Studies of commercial pellet products have documented wide variation in actual hormone content versus label claims.
- Higher adverse event rates. Peer-reviewed case series and FDA adverse-event reports have linked pellet therapy to excess rates of acne, hirsutism, voice deepening, and alopecia compared with transdermal preparations.
- Insertion-site complications. Infection, pellet extrusion, and scarring.
Major professional societies — the Endocrine Society, The Menopause Society (formerly NAMS), and the Global Consensus authors — explicitly recommend against pellet therapy for women. If a clinician is steering you toward pellets, that is a signal to find a different clinician.
Monitoring: Labs, Schedule, and Targets
Testosterone therapy is not "set and forget." The goal is to bring levels into the upper quartile of the normal female range — roughly a total testosterone of 50–70 ng/dL for most assays — and to stay there.
Baseline labs (before starting):
- Total testosterone (ideally by LC-MS/MS for accuracy at low female levels)
- Free testosterone (calculated or direct)
- Sex hormone binding globulin (SHBG) — often elevated by oral estrogen, which lowers free testosterone
- Estradiol and FSH — to confirm menopausal status and estrogen adequacy
- Complete blood count (CBC) — baseline hematocrit
- Lipid panel — testosterone can nudge HDL down at higher doses
- Liver enzymes — baseline only; transdermal testosterone is liver-neutral
See Lab Tests: Hormone Panel for details on how each is drawn and interpreted.
Follow-up schedule:
- 3–6 weeks after starting: Total and free testosterone. Adjust dose if needed.
- 3 months: Symptom reassessment. Honest check: is libido/energy/mood better? If nothing has changed, the therapy is not working.
- Every 6 months thereafter: Total testosterone, free testosterone, SHBG. Annual CBC and lipid panel.
Timing of the blood draw matters. For transdermal cream or gel, draw the lab before that day's application to catch a steady-state trough. For an AM application, a morning lab before the dose is ideal.
The oral estrogen trap. Women on oral estradiol (versus patch or gel) develop a liver-driven rise in SHBG that binds up circulating testosterone, lowering the free fraction even when total testosterone looks fine. A woman taking oral estrogen who still has low libido may benefit more from switching to a transdermal estrogen (see Estradiol Formulations) than from starting testosterone.
Side Effects and Red Flags
At true physiologic replacement doses — meaning blood levels stay within the normal female range — serious side effects are uncommon. Problems generally appear when dosing drifts above the female range, as with pellets or overly enthusiastic cream dosing.
Common and mostly dose-dependent:
- Acne. Often the first signal of too much testosterone. Appears on the chin, jawline, and back. Reversible with dose reduction.
- Increased facial and body hair. Thickening of existing hair on the chin, upper lip, and abdomen. Usually mild at physiologic doses; more marked with pellets.
- Oily skin and scalp.
- Mild fluid retention.
Uncommon but important — stop and call the clinician:
- Voice deepening or hoarseness. This can be permanent even after stopping therapy. It is the single most feared side effect and one of the strongest arguments against pellet dosing.
- Clitoromegaly (clitoral enlargement). Also potentially permanent if dosing stays supraphysiologic for long enough.
- Scalp hair thinning (androgenic pattern). Thinning at the crown and temples.
- Mood irritability, aggression.
Breast cancer and cardiovascular outcome data on testosterone in women remain limited. The 2019 consensus concluded there is no signal of increased breast cancer risk at physiologic doses, but long-term (>5-year) safety data are sparse. Do not use testosterone therapy in women with active hormone-sensitive cancer. See HRT Risks for the broader hormone-therapy risk picture.
Why DHEA Is Not a Reliable Substitute
DHEA (dehydroepiandrosterone) is an adrenal steroid that the body can convert, in small amounts, into testosterone and estrogen. Because it is sold over-the-counter as a supplement, many women try it as a "natural" alternative to prescription testosterone. It mostly doesn't work, for three reasons:
- Unpredictable conversion. How much DHEA becomes testosterone depends on enzyme activity that varies widely between women. Some women convert efficiently and may see modest effects; most don't.
- Supplement quality is wildly inconsistent. Independent testing has repeatedly found commercial DHEA products containing anywhere from 0% to 150% of the labeled dose. You cannot reliably dose what you cannot reliably measure.
- Evidence in postmenopausal women with HSDD is negative. Randomized trials of oral DHEA for postmenopausal low libido have mostly failed to show benefit over placebo.
The one scenario where DHEA has solid evidence is intravaginal DHEA (prasterone, Intrarosa) for genitourinary syndrome of menopause — and that is a local effect on vaginal tissue, not a systemic testosterone substitute. If systemic androgen replacement is the goal, prescription testosterone at a measured dose is the right tool.
Regulatory History: Intrinsa and the Pellet Lawsuits
Intrinsa was a transdermal testosterone patch developed by Procter & Gamble for postmenopausal HSDD, studied most famously in the 2005 trial led by James Simon and colleagues. The trial showed a statistically significant improvement in satisfying sexual events versus placebo. In 2004 the FDA declined to approve Intrinsa, citing concerns about long-term cardiovascular and breast safety given the absence of extended follow-up. Europe approved it in 2006, but the product was withdrawn from the European market in 2012 for commercial reasons after slow uptake. No direct successor has been submitted for U.S. approval, leaving compounded and off-label male products as the only clinical options.
Meanwhile, the testosterone pellet industry has faced a string of lawsuits. Multiple U.S. cases have alleged patient harm from supraphysiologic testosterone levels — permanent voice changes, severe acne, hair loss, and mood disturbance — after pellet insertion at franchise clinics. Settlements and ongoing litigation underscore the regulatory gap: compounded pellets are not FDA-approved, the compounding pharmacies that make them operate under lighter oversight than brand manufacturers, and the clinics inserting them often have financial incentives that tilt toward more frequent and higher-dose insertions.
The practical takeaway for patients: the absence of an FDA-approved female testosterone product does not mean testosterone therapy for women is unsafe. It means the delivery system matters enormously. A measured, daily, reversible, transdermal dose — monitored with labs — is a very different therapy than a 4-month pellet implant from a cash-pay clinic.
Key Research Papers
- Davis SR, et al. Global Consensus Position Statement on the use of testosterone therapy for women. Lancet Diabetes Endocrinol. 2019.
- Simon J, et al. Testosterone patch increases sexual activity and desire in surgically menopausal women with hypoactive sexual desire disorder (INTIMATE SM 1). J Clin Endocrinol Metab. 2005.
- Wierman ME, et al. Androgen therapy in women: a reappraisal — an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2014.
- Davis SR, et al. Testosterone for low libido in postmenopausal women not taking estrogen. N Engl J Med. 2008.
- Glaser R, Dimitrakakis C. Reduced breast cancer incidence in women treated with subcutaneous testosterone, or testosterone with anastrozole — critical appraisal. Menopause. 2018.
PubMed Topic Searches
For current peer-reviewed work on female testosterone therapy, dosing, and safety:
- Testosterone therapy for postmenopausal HSDD
- Transdermal testosterone dosing in women
- Testosterone pellet therapy in women — adverse effects
- Testosterone therapy in women and breast cancer risk
- SHBG, oral estrogen, and free testosterone
- DHEA supplementation and postmenopausal sexual function
- Oophorectomy and androgen deficiency
- Intrinsa testosterone patch trials
Connections
- Reproductive Medicine
- Menopause: Why the Hormones Fall and What Changes — interactive animation
- Estradiol Formulations: Patch, Gel, Oral Routes
- HRT Risks: Breast Cancer, Clots and Stroke
- Bone Loss Prevention and HRT
- Hormone Panel
- Genitourinary Syndrome of Menopause and Vaginal Estrogen
- Depression
- Micronized Progesterone vs Synthetic Progestins
- Vasomotor Symptoms: Hot Flashes and Night Sweats
- Non-Hormonal Options: SSRIs, Gabapentin, Fezolinetant
- Perimenopause Symptom Tracker and Hormonal Testing
- Perimenopause
- Menopause and HRT
- Testosterone
- DHEA-S
- Acne
- Lipid Panel
- Insomnia
- Cardiovascular Disease