Post-Exertional Malaise (PEM) Explained
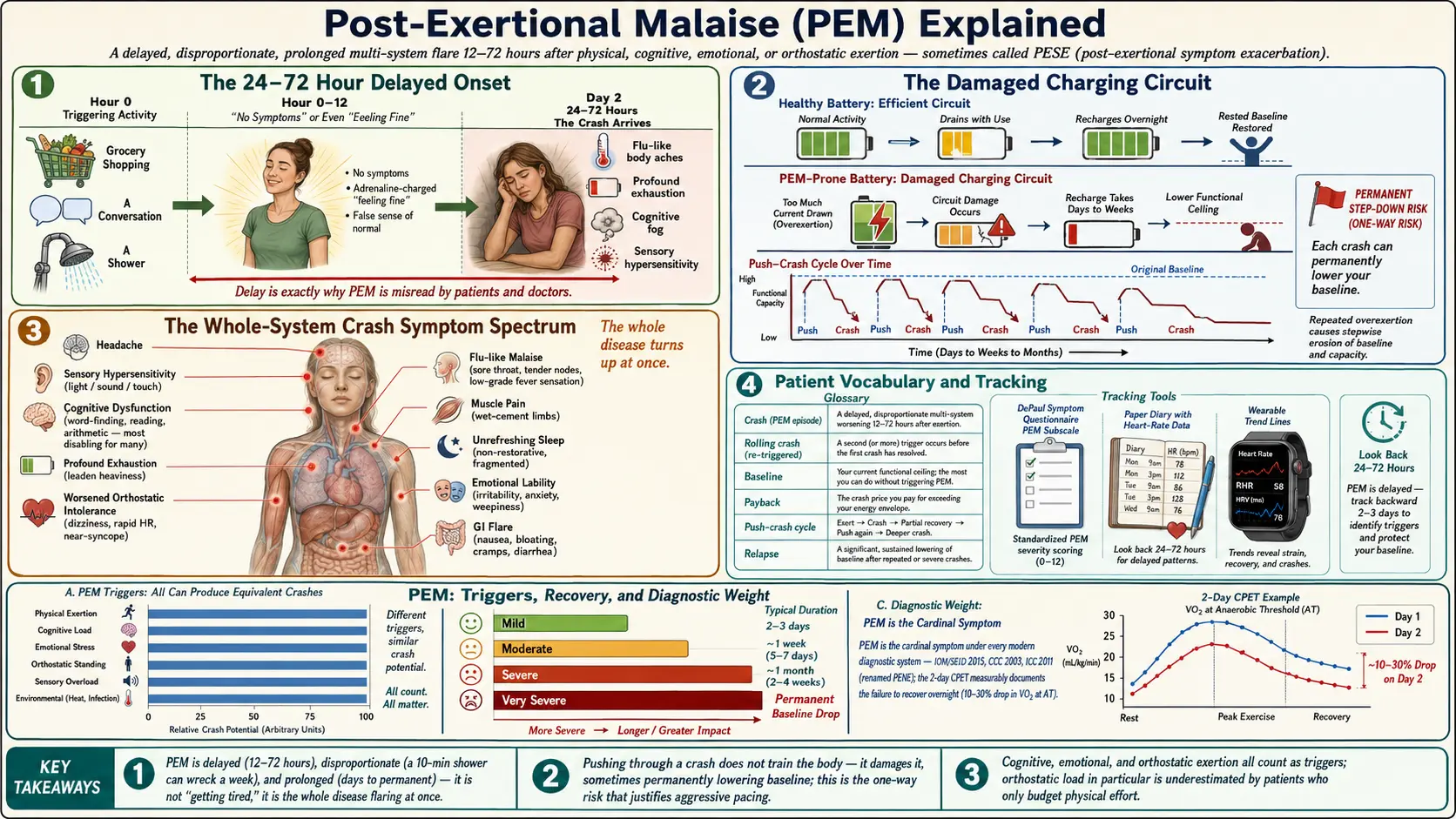
Table of Contents
- What PEM Actually Is (And Isn't)
- The 24–72 Hour Delayed Onset
- Disproportionate Severity: When a Shower Wrecks a Week
- Prolonged Recovery: Days, Weeks, Sometimes Never
- Symptoms Beyond Fatigue
- "Crashes": The Vocabulary Patients Use
- Why PEM Is the Single Defining Feature of ME/CFS
- The DePaul Symptom Questionnaire and Its PEM Subscale
- How to Track PEM Day to Day
- The Energy Envelope — A Working Intro
- Why Graded Exercise Therapy (GET) Is Harmful in ME/CFS
- Practical Advice: Radical Rest, Pre-Emptive Pacing, Saying No
- Talking to Doctors and Family Who Don't Believe You
- Key Research Papers
- Connections
- Featured Videos
What PEM Actually Is (And Isn't)
Post-exertional malaise (PEM) is not "getting tired after doing too much." Every human on earth gets tired after overexertion, recovers with a good night's sleep, and carries on. PEM is something categorically different: a delayed, disproportionate, and prolonged worsening of the entire disease after physical, cognitive, emotional, or orthostatic (upright posture) exertion that a healthy person would barely register.
A useful analogy: a healthy battery drains steadily and recharges overnight. A PEM-prone body is more like a battery with a damaged charging circuit. Drawing too much current doesn't just empty the battery — it damages the charging circuit itself, so the recharge takes days or weeks, and sometimes the battery never returns to its previous capacity. Repeated overdrawing permanently lowers the ceiling.
The word "malaise" undersells it. Malaise sounds like feeling unwell. PEM can flatten a functioning person into bed-bound for a week after walking half a block. Patient advocates have argued for years that the better term is post-exertional symptom exacerbation (PESE) because it captures the full multi-system flare — cognitive, immune, autonomic, muscular — rather than vague "feeling bad."
PEM is the cardinal, required feature of ME/CFS under every modern diagnostic system. It is not a symptom that some patients have and others don't; if it is absent, the diagnosis is wrong. See the diagnostic criteria article for how IOM/SEID, CCC, and ICC all place PEM at the center.
The 24–72 Hour Delayed Onset
The most confusing and most diagnostic feature of PEM is the delay. You do something on Monday. You feel okay that evening, maybe tired but manageable. You sleep. Tuesday morning you wake up and cannot lift your head from the pillow.
This delay is typically 24 to 72 hours after the triggering exertion. In some patients it is shorter (12 hours); in others it stretches to four or five days. The gap between cause and effect is exactly why PEM is so easily misread by both patients and doctors. By the time the crash hits, the triggering activity looks innocent in hindsight — "I just went grocery shopping two days ago, this can't be from that" — but that is exactly the pattern.
The delay is also why the old clinical advice "exercise and you'll feel better" is catastrophic for ME/CFS patients. During and immediately after exertion, many patients feel adrenaline-charged, even good. The disaster arrives on day two or three, long after the cheerful rehabilitation specialist has gone home.
Research-grade evidence of this delay comes from two-day cardiopulmonary exercise testing (CPET), where patients perform a maximal effort test on day one and a repeat test 24 hours later. Healthy people reproduce their day-one numbers on day two. ME/CFS patients show a significant drop in workload at anaerobic threshold and in peak oxygen consumption on day two — an objectively measurable signature of PEM. See the 2-day CPET article for why this test matters for disability claims and research.
Disproportionate Severity: When a Shower Wrecks a Week
Healthy people, and even people with depression or post-viral deconditioning, scale their symptoms to the size of their exertion. Run a marathon, feel wrecked for a day or two. Walk to the mailbox, feel nothing. The relationship is roughly linear.
PEM breaks that scaling. Triggers that are laughably small produce outsized crashes:
- A 10-minute shower can trigger a week of bed-bound crash.
- A 30-minute phone call with a family member can cause three days of cognitive fog so dense that reading a text message feels impossible.
- Sitting upright at a restaurant for an hour can cause a five-day flare of muscle pain, flu-like symptoms, and sore throat.
- Watching an emotionally intense movie can trigger a crash indistinguishable from one caused by physical exertion.
Three practical points follow from this. First, there is no such thing as "just" any activity when you have PEM. The cost is not the activity; the cost is the downstream crash, and it is often much larger than the activity itself. Second, cognitive and emotional exertion count. Many patients can predict and budget physical effort but routinely underestimate the cost of a stressful conversation or a concentrated hour of work email. Third, orthostatic exertion — simply being upright — counts, and for patients with overlapping POTS or orthostatic intolerance, standing in line can be the most expensive activity of the day. See orthostatic intolerance in ME/CFS.
Prolonged Recovery: Days, Weeks, Sometimes Never
A healthy person's post-exercise soreness resolves in 24 to 72 hours. PEM crashes routinely last days to weeks. Mild PEM may lift in two or three days of strict rest. Moderate PEM can stretch a week or more. Severe PEM triggered by a significant overdraw — a wedding, a flight, a cross-town medical appointment — can last a month.
The most feared outcome is a permanent drop in baseline. Repeated or severe crashes can reset the patient's energy ceiling downward, and that new, lower baseline may never recover. People who were mild and working full time have become housebound after a single aggressive push-crash cycle. People who were moderate and housebound have become bedbound the same way. This one-way risk is the reason experienced patients become so cautious, and why the language around pacing can sound almost paranoid to outsiders. The paranoia is earned.
This is the single most important medical fact for the family and friends of someone with ME/CFS to understand: pushing through a crash does not train the body. It damages it, sometimes permanently.
Symptoms Beyond Fatigue
PEM is not "more tiredness." It is a multi-system flare of the whole disease. During a crash, patients commonly experience some combination of:
- Profound exhaustion — far beyond ordinary fatigue; a leaden heaviness that sleep does not touch.
- Cognitive dysfunction ("brain fog") — difficulty finding words, reading, following conversations, doing simple arithmetic. For many patients this is the most disabling symptom.
- Flu-like malaise — sore throat, tender lymph nodes, low-grade fever sensation, body aches. This is why patients so often say "I feel like I'm coming down with the flu that never arrives."
- Muscle pain and weakness — aching, heaviness, the sensation that the limbs are filled with wet cement.
- Headache — often a pressure or migraine-type headache; see migraine.
- Sensory hypersensitivity — light, sound, and touch all become intolerable. A quiet room can feel loud.
- Sleep disturbance — paradoxically, sleep becomes unrefreshing or fragmented exactly when the body most needs it.
- Worsened orthostatic intolerance — standing becomes harder, heart rate swings wider.
- Emotional lability — tearfulness, irritability, a thin skin for any additional stressor. This is neurochemical, not psychological weakness.
- Gastrointestinal flare — nausea, bloating, food intolerances suddenly worse.
Any or all of these can show up together. The characteristic pattern is the whole disease turning up the volume at once, rather than one isolated symptom worsening.
"Crashes": The Vocabulary Patients Use
Most patients don't say "I am having post-exertional malaise." They say "I'm crashing" or "I'm in a crash." The community vocabulary matters because it encodes real distinctions:
- Crash — a specific PEM episode triggered by identifiable overexertion.
- Rolling crash — a crash that gets re-triggered before it resolves, so the patient never returns to baseline.
- Baseline — the patient's current functional ceiling, measured in honest hours of upright or cognitive activity per day.
- Payback — the crash price of a specific activity. "I went to the dentist yesterday; I'll be paying it back for three days."
- Push-crash cycle — the pattern of doing more on a good day, then crashing, then doing nothing for a week, then doing more again. Over time this erodes the baseline.
- Relapse — a sustained drop in baseline that lasts weeks or months and may or may not return.
This vocabulary is worth learning because it is the shortest way to communicate with other patients, advocates, and the few clinicians who understand the disease.
Why PEM Is the Single Defining Feature of ME/CFS
Fatigue exists in dozens of conditions. Depression causes fatigue. Deconditioning causes fatigue. Hypothyroidism (see Hashimoto's), anemia, sleep apnea, cancer, kidney disease, and a long list of others all cause fatigue. What separates ME/CFS from every one of them is PEM with its specific signature: delayed, disproportionate, prolonged, multi-system.
- Depression causes low energy and anhedonia, but exercise typically improves depressive symptoms rather than triggering a 72-hour multi-system flare. The delay signature is missing.
- Deconditioning from prolonged bedrest causes reduced exercise tolerance, but graded reintroduction of activity restores capacity. In ME/CFS, the same graded reintroduction damages capacity.
- Fibromyalgia (see fibromyalgia) causes widespread pain and fatigue; many fibromyalgia patients have PEM too and meet ME/CFS criteria. But fibromyalgia without PEM is a distinct clinical picture and responds differently to movement.
- Chronic fatigue as a symptom is not the same as chronic fatigue syndrome as a disease. Many medical conditions produce chronic fatigue without PEM, and mistakenly labeling them ME/CFS has muddied decades of research.
The 2015 Institute of Medicine report (now called the National Academy of Medicine) made PEM the core required criterion for a new name, systemic exertion intolerance disease (SEID), explicitly to end the confusion. The Bateman 2021 consensus recommendations (see Key Research Papers below) doubled down: if a patient does not have PEM, the clinician should keep looking for a different diagnosis.
The DePaul Symptom Questionnaire and Its PEM Subscale
The most widely used research instrument for measuring PEM is the DePaul Symptom Questionnaire (DSQ), developed by Leonard Jason's research group at DePaul University. The DSQ and its shorter variants ask patients to rate the frequency and severity of dozens of symptoms on a 0–4 scale, then apply algorithms to check whether the patient meets CCC, ICC, and IOM/SEID criteria.
The PEM subscale is a short set of items asking specifically about:
- Dead, heavy feeling after starting to exercise.
- Next-day soreness or fatigue after non-strenuous, everyday activities.
- Mental fatigue after the slightest effort.
- Minimum exercise making you physically tired.
- Physical fatigue, not mental, after exercise.
A positive PEM subscale requires at least one item at moderate frequency and moderate severity or higher (typically scored "at least half the time" plus "moderate" severity or worse). The DSQ is freely available for download from the DePaul research group and is worth filling out before any specialist visit — not because your doctor will recognize it, but because the act of scoring it gives you concrete, comparable numbers to track over time.
How to Track PEM Day to Day
Tracking is not optional. Without data, you cannot see the 48-hour delay, you cannot learn your envelope, and you cannot prove disability to a skeptical clinician or insurer. Three tracking strategies, in order of increasing sophistication:
Paper or plain-text log. A simple daily entry with three numbers: hours of upright activity, subjective energy (1–10), and symptom score (1–10). Over weeks, the 48-hour lag between activity spikes and symptom spikes becomes visible in the numbers. This is the cheapest and most honest method.
Heart-rate monitoring. A chest-strap or wrist heart-rate monitor set to beep when your heart rate exceeds your anaerobic threshold (AT) — often estimated as roughly 60% of (220 − age), but ideally measured by a 2-day CPET. Staying below AT reduces PEM risk by keeping the body in aerobic metabolism. Many patients find this the single most useful technology.
Dedicated pacing apps. Two widely used apps in the ME/CFS and long-illness community are Visible (which pairs with a Polar armband for heart-rate variability and activity tracking) and Bearable (a general symptom tracker with flexible custom metrics). Both let you export data for your own review or for your doctor.
Whatever method you choose, the goal is the same: make the invisible 48-hour feedback loop visible, so you can act on it.
The Energy Envelope — A Working Intro
The energy envelope is the practical concept that flows out of PEM. It is the total amount of physical, cognitive, emotional, and orthostatic activity you can perform in a day without triggering a crash. The envelope is personal, it varies week to week, and it is almost always smaller than you think.
Pacing means staying inside that envelope — not at its edge, but comfortably inside it, with reserve. Specifically:
- Plan the day under your best estimate of capacity, not at it.
- Rest pre-emptively, before symptoms appear, not after.
- Treat cognitive and emotional effort as counting against the same budget as physical effort.
- Build in recovery days after any unavoidable over-expenditure (a medical appointment, a family event).
The full protocol — how to estimate your envelope, how to expand it safely, the role of heart-rate-based pacing — lives in the sibling article on pacing and the energy envelope. Treat this section as the "why"; that article is the "how."
Why Graded Exercise Therapy (GET) Is Harmful in ME/CFS
For decades, British and American clinical guidelines recommended graded exercise therapy (GET) — a protocol in which patients incrementally increase activity regardless of symptoms, on the deconditioning model. The 2011 PACE trial, at the time the largest ME/CFS trial ever run, claimed modest benefit. Subsequent reanalysis of the PACE data, large patient surveys, and mechanistic studies like the 2-day CPET have demolished the deconditioning model:
- Patient surveys consistently report that 50–75% of patients worsen on GET, and a substantial minority suffer permanent drops in baseline.
- The 2-day CPET demonstrates an objective metabolic abnormality on the second day that deconditioning does not reproduce.
- In 2021, the UK's NICE guideline (NG206) formally withdrew its recommendation of GET for ME/CFS and cautioned against any approach requiring fixed incremental activity increases.
- The U.S. CDC removed GET from its clinician recommendations in 2017 and now emphasizes pacing.
The key mechanism: ME/CFS involves measurable impairment in aerobic energy production, particularly on the day after exertion. Forcing exertion on an impaired system does not train it; it damages it. This is why a diagnostic framework that distinguishes PEM-present ME/CFS from PEM-absent chronic fatigue matters so much — the two populations respond in opposite ways to the same intervention.
If a clinician still recommends GET, it is a red flag that they have not kept current with the evidence. Find another clinician.
Practical Advice: Radical Rest, Pre-Emptive Pacing, Saying No
At the first sign of a crash, rest radically. That means horizontal, dark room, no phone, no conversation, no mental stimulation. For moderate and severe patients it means days, not hours. This is the single intervention with the best chance of shortening a crash and protecting baseline. Treat the first warning signs — flu-like malaise, unusual brain fog, increased orthostatic symptoms — as an early alarm, not as something to push through.
Pace pre-emptively, not reactively. Rest before you feel tired. Cap activities by the clock, not by how you feel in the moment. Many patients describe feeling unnaturally good during the "adrenaline window" of exertion; this is not a green light, it is a trap. Set a timer and stop when it rings, even if you feel fine.
Learn to say no, and build scripts for it. "I can't, my health doesn't allow it" is a complete sentence. You do not owe anyone an exhaustive medical explanation. Saving your envelope is saving your long-term health.
Bank recovery days. If you have to travel for a medical appointment, plan to do nothing else that week. If a family event is unavoidable, rest hard for three days before and plan a week of rest after. Treat every major commitment as a debt that must be prepaid and post-paid.
Reduce friction. A shower stool, a grocery delivery subscription, a bedside commode for severe days, meals in the freezer — every conserved unit of effort is envelope preserved. These are medical accommodations, not laziness.
Watch overlapping conditions. POTS and MCAS frequently co-exist with ME/CFS and can each independently trigger PEM-like flares. Treating orthostatic intolerance (compression garments, fluids, salt, medication) and mast-cell activation (H1/H2 blockers, cromolyn) can meaningfully expand the envelope.
Talking to Doctors and Family Who Don't Believe You
A painful reality: most doctors, and many family members, will not initially believe you. They see you on a good hour, they hear "fatigue," they map it onto depression or deconditioning, and they recommend exercise. The misunderstanding is not personal; it is the historical failure of medicine to teach PEM.
A few things that help:
- Bring data. A printed symptom log, a DSQ score, heart-rate data, or — if available — a 2-day CPET report. Numbers move skeptical clinicians in a way narrative does not.
- Use the specific vocabulary. "I have post-exertional malaise. It is the cardinal feature of ME/CFS under the 2015 Institute of Medicine criteria. My symptoms get worse 24 to 72 hours after exertion and take days to weeks to resolve."
- Cite the guidelines. NICE NG206 (2021) and the CDC ME/CFS clinician page both explicitly caution against GET and recommend pacing. These are not fringe positions.
- Pre-empt the deconditioning argument. "I understand the reasoning about deconditioning, but the two-day CPET literature and the Stussman qualitative work show that PEM has a specific metabolic and symptomatic signature that deconditioning does not reproduce."
- For family: the phone-battery analogy often lands. "If I push through today, I don't bounce back tomorrow. I lose the week. And if I do it too often, I lose the year."
- Find an ME/CFS-literate clinician if possible. The Bateman Horne Center (Salt Lake City), Open Medicine Clinic (California), and a growing list of post-viral and long-illness clinics maintain online referral lists. Telemedicine has expanded access enormously.
You will sometimes still not be believed. That is not evidence that you are wrong. It is evidence that medicine, on this disease, is still catching up. Protect your envelope anyway.
Key Research Papers
- Jason LA, et al. Examining case definition criteria for chronic fatigue syndrome and myalgic encephalomyelitis. Fatigue: Biomedicine, Health & Behavior. 2010. — foundational work on PEM and the DePaul Symptom Questionnaire.
- Stussman B, et al. Characterization of post-exertional malaise in patients with myalgic encephalomyelitis/chronic fatigue syndrome. Front Neurol. 2020. — qualitative study describing PEM onset, triggers, and recovery in patients' own words.
- VanNess JM, et al. Postexertional malaise in women with chronic fatigue syndrome. J Womens Health. 2010. — two-day CPET evidence of objective metabolic impairment on the day after exertion.
- Bateman L, et al. Myalgic encephalomyelitis/chronic fatigue syndrome: essentials of diagnosis and management. Mayo Clin Proc. 2021. — the modern consensus clinician guide centering PEM as the required diagnostic feature.
Live PubMed Searches
For deeper reading, the following PubMed topic searches return current peer-reviewed work on PEM biology, measurement, and management:
- Post-exertional malaise in ME/CFS
- Two-day CPET and ME/CFS
- DePaul Symptom Questionnaire validation
- Graded exercise therapy harm in ME/CFS
- Pacing and the energy envelope
- Anaerobic threshold and heart-rate pacing
- NICE NG206 ME/CFS guideline
- Post-exertional symptom exacerbation (PESE)
Connections
- ME/CFS Overview
- Orthostatic Intolerance in ME/CFS
- 2-Day CPET and Objective Testing
- Pacing and the Energy Envelope
- ME/CFS Diagnostic Criteria
- Post-Viral Triggers: EBV and Others
- Severe and Very Severe ME
- LDN, Abilify and Experimental Therapies
- Mitochondrial Dysfunction and Energy Metabolism
- Fibromyalgia
- Fibromyalgia and ME/CFS Overlap
- POTS
- MCAS
- Low-Dose Naltrexone
- Hashimoto's Thyroiditis
- Chronic Pain
- Fatigue
- Brain Fog
- POTS
- MCAS
- Chronic Pain
- Low-Dose Naltrexone