Pacing and the Energy Envelope in ME/CFS
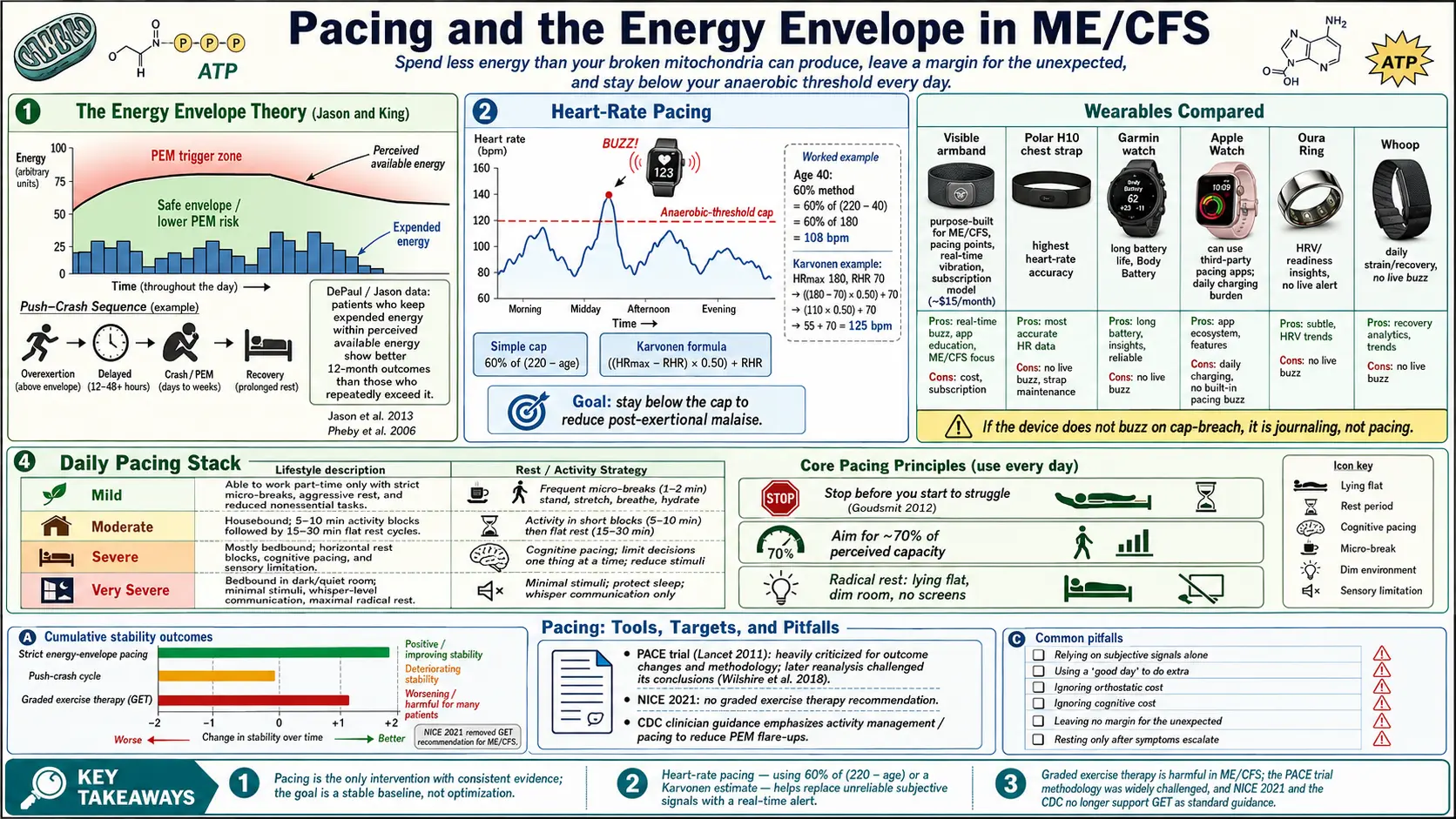
Table of Contents
- What Pacing Actually Means
- The Energy Envelope Theory (Jason & King)
- Heart-Rate Pacing — The Most Useful Tool You Have
- How to Find YOUR Cap
- Wearables Compared
- "Stop Before You Start to Struggle"
- Aggressive Rest and Horizontal vs Upright
- Tracking Payback
- Sample Daily Schedules by Severity
- Cognitive and Social Pacing
- Medication Support for Pacing
- Why Graded Exercise Therapy Is Harmful
- The PACE Trial Controversy in Brief
- Common Pitfalls
- Key Research Papers
- Connections
- Featured Videos
What Pacing Actually Means
Pacing is the only intervention with consistent evidence for ME/CFS. It is not a pep talk about "listening to your body." It is a concrete, measurable discipline: spend less energy in a day than your broken mitochondria can produce, and leave a margin for the unexpected. Exceed the margin and you trigger post-exertional malaise (PEM) — the hallmark crash that can flatten you for 48 hours, two weeks, or permanently drop your baseline.
Think of your daily energy like a bank account that does not refill reliably overnight. A healthy person's account tops up to full every morning. In ME/CFS, overnight recovery is partial and unpredictable, and overdraft fees are catastrophic. Pacing is the household budget you live by so you do not overdraft. The goal is not to push through — pushing through is the disease's trap. The goal is to stay inside the envelope so your baseline stabilizes and, over months to years, may slowly expand.
The Energy Envelope Theory (Jason & King)
The formal framework behind pacing was developed by Leonard Jason and colleagues at DePaul University in the 1990s and refined through the 2000s and 2010s. Their energy envelope theory (Jason 2013, Pheby 2006) proposes that people with ME/CFS have a fixed daily envelope of perceived available energy and a corresponding level of expended energy. Symptoms stabilize or improve when expended energy stays at or below perceived available energy. Symptoms worsen whenever expended energy exceeds it.
In their studies, patients who kept expended energy inside their envelope for 12 months showed measurable improvements in physical functioning, while those who chronically exceeded it got worse. The effect was not large — pacing is not a cure — but it was real and reproducible, and it is one of the few ME/CFS interventions that does not harm patients.
The practical implication is humbling: your envelope is what your body can actually do today, not what you think you should be able to do, not what you could do last year, not what your doctor thinks you should be able to do. The envelope is set by physiology, not willpower.
Heart-Rate Pacing — The Most Useful Tool You Have
Subjective pacing ("I feel okay, I'll keep going") fails because ME/CFS blunts the normal warning signals. By the time you feel tired, you are often already past your limit and a crash is baked in. Heart-rate pacing replaces subjective signals with an objective number you can watch in real time.
The core idea: ME/CFS patients hit their anaerobic threshold (AT) — the point at which the body switches from aerobic to anaerobic metabolism — at very low workloads, often at heart rates a healthy person would consider resting. Crossing AT is what triggers PEM. If you can keep your heart rate below AT for most of the day, you give yourself a fighting chance of avoiding a crash.
Two common ways to estimate AT without a lab test:
- 60% of predicted HRmax. Use the formula HRmax = 220 − age, then multiply by 0.60. A 40-year-old's cap would be (220 − 40) × 0.60 = 108 bpm. Simple, rough, and usually conservative enough as a starting point.
- Karvonen AT estimate. Uses your resting heart rate (RHR) for a more personalized cap: AT ≈ ((HRmax − RHR) × 0.50) + RHR. For a 40-year-old with a RHR of 70: ((180 − 70) × 0.50) + 70 = 125 bpm. The Karvonen method tends to run slightly higher than the flat-60% rule.
Start with the lower of the two. You want the alarm to trip before you have exceeded AT, not after.
How to Find YOUR Cap
The gold standard is a 2-day CPET (cardiopulmonary exercise test), where you perform a maximal test one day, repeat it 24 hours later, and the lab measures your actual AT on day two — which in ME/CFS is typically 10–30% lower than day one. This is discussed in detail in the 2-Day CPET article. A CPET gives you a hard number, but it is expensive ($2,000–$4,000), not widely available, and the test itself can trigger a significant PEM crash. For many patients it is worth it for the diagnostic documentation; for others it is unsafe.
Most people find their cap by trial and error:
- Start with the formula cap (60% HRmax).
- Wear a continuous HR monitor for two weeks and note every time you breach the cap.
- Note any PEM episode and the activity that preceded it by 24–72 hours (PEM is famously delayed).
- If you are crashing despite "staying within" the cap, lower it by 5–10 bpm.
- If you are stable for several weeks, you have found a workable cap. Do not raise it — stability is the goal, not optimization.
Expect your cap to move. It often drops during a viral illness, after stressful events, in hot weather, or around menstruation. Some patients run two caps: a "good day" cap and a "bad day" cap 10–15 bpm lower.
Wearables Compared
You need a device that will alert you in real time when you breach your cap. A daily summary is useless — by then the damage is done. Options vary widely:
- Visible armband (with Visible Plus subscription) — purpose-built for ME/CFS, Long COVID, and POTS. Continuous optical HR plus an in-app "pacing points" system, HRV morning readiness score, and real-time vibration alerts when you exceed a user-set HR cap. The dashboard is designed around energy envelope concepts. The subscription cost (about $15/month) is a real barrier, but for many patients it is the single most useful tool they own.
- Polar H10 chest strap — the most accurate consumer HR monitor made. Paired with a watch or a phone app (Polar Beat, EliteHRV), it gives near-medical-grade readings. Requires wearing a strap under clothing, which some patients find uncomfortable during bed rest.
- Garmin (Venu, Vivoactive, Forerunner) — excellent HR alerts, customizable zones, long battery life (days to weeks). Native "HR alert" function vibrates when you cross a threshold. Body Battery metric is a rough energy proxy.
- Apple Watch — good HR accuracy, supports third-party pacing apps (HeartWatch, Pacy). Battery life is the main weakness — needs daily charging, which means you have to schedule charging into your day. Native high-HR alerts can be set but are clumsy.
- Oura Ring — strong for overnight HRV and readiness, weaker for real-time HR alerts (no display, no buzz). Best used alongside another device for live pacing, not as your primary alert.
- Whoop — strap-only, no screen. Daily "strain" score and HRV trends. Again, no real-time buzz for exceeding a cap, so it complements rather than replaces a watch or armband.
The single most important feature is a vibration alert when you cross your cap. If the device does not buzz, it is not pacing — it is journaling.
"Stop Before You Start to Struggle"
This phrase, popularized by Ellen Goudsmit (2012) in her pacing research, is the single most useful rule in ME/CFS. By the time you feel strain — heavy legs, brain fog thickening, hands shaking on the cup — you are already over the line. The body's warning system in ME/CFS is delayed and unreliable.
Practical translations:
- If a task takes 20 minutes, stop at 10 and rest.
- Break any activity into blocks: 5–10 minutes of activity, 15–30 minutes flat rest, repeat.
- If the HR alert buzzes, stop immediately and lie down — do not finish the sentence, do not finish loading the dishwasher. The next 30 seconds matter more than the task.
- Plan to underachieve. Aim for 70% of what you think you can do. The other 30% is the margin that keeps you stable.
Aggressive Rest and Horizontal vs Upright
"Rest" for a healthy person means sitting on the couch watching TV. "Rest" for someone with ME/CFS usually means lying flat in a dim, quiet room with no screens. This is sometimes called aggressive rest therapy (ART) and is particularly important for patients with any overlap with POTS or other orthostatic intolerance.
Why horizontal matters: upright posture itself is work. Your heart has to pump blood against gravity to your brain, and in ME/CFS plus POTS that is enough to push HR above AT just from sitting at a desk. Lying flat removes the orthostatic load. Symptoms that feel relentless while sitting frequently fade within 10–20 minutes of lying down.
A hierarchy of rest, from most to least restorative:
- Flat supine, dark room, no input (eyes closed or covered, earplugs). The reset button.
- Flat supine, dim room, audio only (music, podcast, audiobook at low volume).
- Reclined (45° or less), dim room. Acceptable maintenance rest.
- Upright sitting, screen on. This is activity, not rest. Count it in your envelope.
Add-ons that can deepen rest: an eye mask, a weighted blanket (light weight only — heavy blankets raise HR), compression garments for orthostatic support while transitioning upright (see the POTS compression program), and a cool room (heat tolerance is usually poor).
Tracking Payback
"Payback" is the delayed cost of today's activity — the PEM crash that arrives 24–72 hours later. Because the delay is long and variable, people routinely blame today's crash on today's activity and miss the real culprit from two days ago.
A minimal tracking log, done for 4–8 weeks, usually reveals the pattern. Each day record:
- Activities (with duration) and any HR breaches.
- Upright minutes total.
- Symptom score 0–10 (fatigue, brain fog, pain, sleep quality).
- Any notable triggers: poor sleep, stress, heat, menstrual phase, alcohol, infection.
Apps that do this well include Visible, Bearable, and a simple paper diary. After a few weeks you will see that crashes on Wednesday track back to Monday's grocery run, not Tuesday's nap. Adjust the envelope accordingly.
Sample Daily Schedules by Severity
These are starting points, not prescriptions. Your envelope is your envelope.
Mild (50–70% function)
- Wake, eat a small breakfast sitting or reclined, 20 min flat rest.
- One block of desk work or light activity, 60–90 min, HR-monitored.
- 30–45 min flat rest.
- Short errand or light household task, 30–45 min.
- Lunch + 30 min flat rest.
- Second activity block, 60–90 min.
- Flat rest before dinner.
- Quiet evening, screen time capped, lights down by 10pm.
Moderate (25–50% function, mostly housebound)
- Wake, breakfast in bed or reclined, 30–60 min flat rest.
- One 20–30 min activity block (shower OR meal prep OR one phone call — pick one, not all).
- 60–90 min flat rest, dark and quiet.
- Another small activity block in the afternoon.
- Most of the day is rest with short activity islands, not the reverse.
- Grocery delivery, disposable plates on bad days, shower seat in the shower.
Severe (under 25% function, mostly bedbound)
- Most of the day flat in a dark, quiet room.
- Meals delivered to the bedside. A bedside commode may replace trips to the bathroom.
- Social contact limited to minutes per day, at low volume.
- Screens off or heavily limited (blue-light glasses, lowest brightness).
- Caregiving support for washing, feeding, and medication.
- See the severe/very severe ME article.
Cognitive and Social Pacing
Brains run on energy too. In ME/CFS, cognitive exertion triggers PEM just as reliably as physical exertion, and people often discover this the hard way after a long work call, a tax return, or a family video chat. Concentration, reading, driving, and emotional conversations all draw from the same envelope.
Practical cognitive pacing:
- Chunk it. 15–25 minutes of focused mental work, then 15–30 minutes flat rest with eyes closed.
- Limit input. One stimulus at a time. No music while reading. No multi-tab web browsing. No podcast while cooking.
- Schedule hard cognitive tasks for your best time of day, usually mid-morning.
- Budget conversations. A 30-minute phone call with a parent is not free. Count it.
Social pacing is its own category. Social interaction in ME/CFS is cognitively and emotionally expensive, and the emotional cost is often larger than the physical. Many patients limit themselves to one social contact per day, with most contacts by text or short voice note rather than live video. Saying no is a medical intervention, not rudeness.
Medication Support for Pacing
Pacing is primary. Medications do not replace it, but a few can lower the HR cost of daily life and make pacing more practical.
- Low-dose beta blockers (propranolol 10–40 mg, or atenolol) — lower resting and exertional HR, particularly useful for patients with POTS overlap. Can shift what was a 125-bpm activity into a 95-bpm activity, expanding the envelope without adding workload. Caution if baseline blood pressure is already low.
- Ivabradine — a heart-rate-lowering drug that acts on the sinus node without affecting blood pressure. Increasingly used in POTS and ME/CFS where beta blockers are poorly tolerated.
- Salt and fluid loading (3–10 g sodium/day, 2–3 L fluid) — expands blood volume, reduces HR spikes on standing, reduces how much of your envelope upright posture eats.
- Fludrocortisone (0.1–0.2 mg) — a steroid that retains sodium and expands plasma volume. Second-line for orthostatic overlap.
- Midodrine — raises blood pressure via vasoconstriction; useful where low BP drives the HR climb.
- Low-Dose Naltrexone (LDN) — 1.5–4.5 mg at bedtime. Anti-inflammatory and neuromodulatory effects; a subset of patients report reduced PEM severity and slightly larger envelopes. See the LDN and experimental therapies article.
None of these are cures, and all should be discussed with a clinician experienced in ME/CFS, POTS, or dysautonomia.
Why Graded Exercise Therapy Is Harmful
Graded Exercise Therapy (GET) is the structured program of gradually increasing exercise duration and intensity that, for decades, was recommended to ME/CFS patients by mainstream medicine. For ME/CFS it is the opposite of pacing: it pushes patients beyond their envelope on the false assumption that fatigue is driven by deconditioning.
Patient surveys consistently show GET worsens ME/CFS in 50–75% of people who try it — the largest harm rate of any prescribed intervention in the condition. Many patients date a permanent drop in baseline to a GET program.
In October 2021, the UK's NICE guideline NG206 for ME/CFS explicitly removed GET as a recommended treatment and warned against "any programme that uses fixed incremental increases in physical activity or exercise." The guideline also rejected Cognitive Behavioural Therapy as a curative treatment (while permitting it as a supportive tool for living with a chronic illness). You can read the guideline directly at nice.org.uk/guidance/ng206.
The U.S. CDC removed GET and CBT from its ME/CFS information pages in 2017. The IOM/NAM 2015 report that defined Systemic Exertion Intolerance Disease (SEID) centered PEM as the core feature — which makes any therapy that provokes PEM fundamentally wrong-headed.
If a clinician recommends GET for ME/CFS in 2026, they are working from retired guidelines. Politely share the NICE 2021 update and ask for a pacing-based approach instead.
The PACE Trial Controversy in Brief
The PACE trial (Lancet 2011) was the headline study behind the GET/CBT recommendation. It reported that GET and CBT were moderately effective for "chronic fatigue." After years of patient advocacy and a freedom-of-information lawsuit, the raw data were released in 2016 and re-analyzed by independent researchers.
The re-analyses found the trial had mid-study lowered its thresholds for "recovery" and "improvement," such that a patient could qualify as "recovered" while still meeting the original entry criteria for disabling fatigue. Using the original, pre-registered thresholds, the effect sizes collapsed to non-significance. The trial's population was also heterogeneous, relying on the broad Oxford criteria that do not require PEM — meaning many participants likely did not have ME/CFS at all.
PACE is now widely regarded in the ME/CFS research community as a cautionary tale in outcome-switching and criterion creep. Its dismantling was the evidence base behind the 2021 NICE reversal.
Common Pitfalls
- The "good day" trap. You feel unusually well, so you clean the kitchen, answer three emails, and go for a short walk. Payback hits on Wednesday. Good days are for rest, not catch-up.
- The gradual creep. You add five minutes of activity a week. After two months you are doing 40 minutes more per day than your envelope allows, and you crash.
- Ignoring cognitive load. You paced your physical activity but worked a five-hour tax session and crashed anyway.
- Unpaced showers. A hot shower can put HR over AT for 10–15 minutes straight. Shower seat, lukewarm water, and short duration. Consider washing in sections on different days.
- Unpaced meals. Digestion itself costs energy and drops blood pressure. Eat smaller, more often, reclined if needed.
- Refusing to use aids. Mobility aids (wheelchair for airport travel, shower seat, grabber tools) are envelope extenders, not defeats.
Key Research Papers
- Jason LA, et al. The energy envelope theory and myalgic encephalomyelitis/chronic fatigue syndrome. Hum Psychopharmacol Clin Exp. 2013.
- NICE Guideline NG206. Myalgic encephalomyelitis (or encephalopathy)/chronic fatigue syndrome: diagnosis and management. National Institute for Health and Care Excellence. 2021.
- Goudsmit EM, Nijs J, Jason LA, Wallman KE. Pacing as a strategy to improve energy management in myalgic encephalomyelitis/chronic fatigue syndrome: a consensus document. Disabil Rehabil. 2012.
- Pheby D, Saffron L. Risk factors for severe ME/CFS. Disabil Rehabil. 2006.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on pacing, the energy envelope, heart-rate-based self-management, and PEM prevention in ME/CFS:
- Energy envelope theory and ME/CFS
- Pacing in myalgic encephalomyelitis
- Heart-rate pacing and anaerobic threshold in ME/CFS
- Post-exertional malaise prevention strategies
- Graded exercise therapy harms in ME/CFS
- PACE trial re-analyses and methodology
- Two-day CPET findings in ME/CFS
- Orthostatic intolerance and heart rate in ME/CFS
Connections
- ME/CFS Overview
- Post-Exertional Malaise
- 2-Day CPET and Objective Testing
- Severe and Very Severe ME
- LDN, Abilify and Experimental Therapies
- ME/CFS Diagnostic Criteria
- Orthostatic Intolerance in ME/CFS
- Post-Viral Triggers: EBV and Others
- Mitochondrial Dysfunction and Energy Metabolism
- POTS
- POTS Compression and Exercise Program
- MCAS
- Fibromyalgia
- Fibromyalgia Exercise Pacing and Graded Movement
- Chronic Pain
- Stress Management
- Sleep Hygiene
- Fatigue