2-Day CPET and Objective Testing for ME/CFS
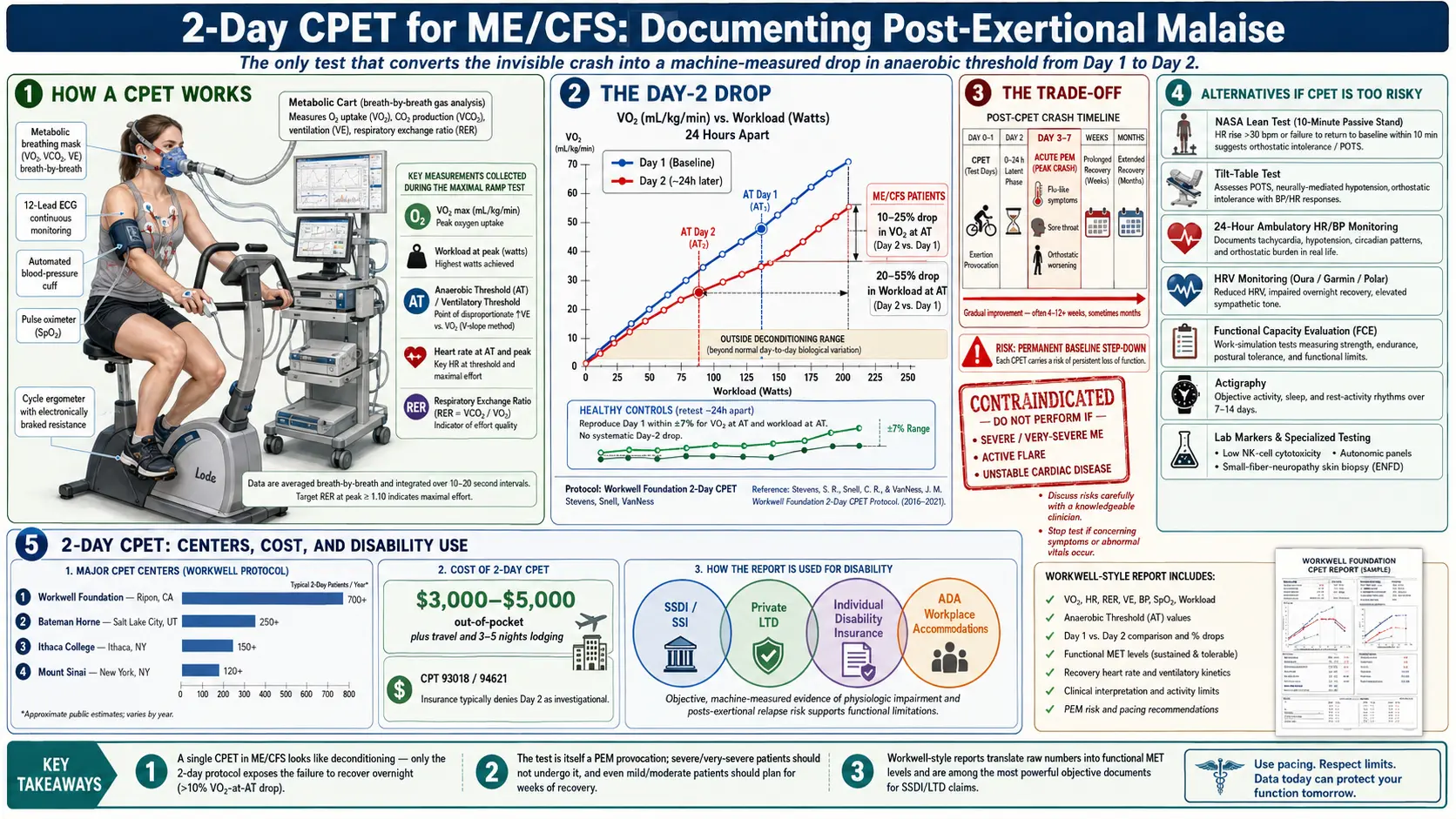
Table of Contents
- Why Objective Testing Matters
- What a CPET Actually Is
- Why Two Days — The Day-2 Drop
- The Day-2 Numbers That Count
- The Trade-Off — This Test Can Crash You
- Who Is Appropriate (and Who Is Not)
- Where to Get a 2-Day CPET
- Cost, Insurance, and Paying Out of Pocket
- Preparing for the Test
- Using the Results for Disability Claims
- Alternatives If You Are Too Sick for CPET
- Autonomic Panels, NK Cells, and Other Objective Markers
- Making the Decision
- Key Research Papers
- Connections
- Featured Videos
Why Objective Testing Matters
If you have ME/CFS, you have probably heard some version of this sentence from a doctor: "Your labs look fine." Complete blood count normal. Metabolic panel normal. Thyroid normal. Inflammatory markers normal. And yet you cannot work, cannot shower without resting, cannot walk to the mailbox without paying for it two days later. The gap between how you feel and what shows up on standard tests is one of the hardest parts of this illness — not only because of the symptoms themselves, but because that gap is used against you by disability insurers, employers, family members, and sometimes your own clinicians.
Objective testing is the bridge. It is how you turn the invisible crash into a number on a page. And in ME/CFS, the single most powerful piece of objective evidence we have is the two-day cardiopulmonary exercise test, or 2-day CPET. It is the only test that reliably documents post-exertional malaise (PEM) — the defining feature of ME/CFS — as a measurable physiological failure rather than a subjective complaint.
This article is written for patients considering whether a 2-day CPET makes sense for them, what the test actually involves, how to prepare, what it costs, how to use the results, and — just as importantly — when not to do it. Because this test is not free in any sense. It is expensive in dollars, and it is expensive in health. For the wrong patient on the wrong day, it can trigger a crash that lasts weeks or months. For the right patient it can be the single document that gets a disability claim approved or finally convinces a skeptical physician that the illness is real.
What a CPET Actually Is
A cardiopulmonary exercise test is a standard piece of cardiology and pulmonology. You sit on a stationary bike (or, less commonly, walk on a treadmill) while a technician measures everything your body does as the resistance gradually increases. You wear a mask that captures every breath. A 12-lead ECG tracks your heart rhythm. A blood pressure cuff cycles automatically. A pulse oximeter clips to your finger. A pedal cadence monitor times your revolutions.
The test runs until you cannot go further — a "maximal" effort ending in volitional exhaustion, usually 8 to 12 minutes of pedaling. During that time the equipment records, breath by breath:
- VO2 max — the peak volume of oxygen your body can use per minute, normalized to body weight (mL/kg/min). This is the classic measure of aerobic fitness.
- Workload at peak — the watts of resistance you were pedaling against when you stopped.
- Anaerobic threshold (AT), also called the ventilatory threshold — the point at which your body shifts from aerobic to anaerobic metabolism. This is the workload you can sustain for hours in daily life without accumulating oxygen debt.
- Heart rate at AT and at peak, respiratory exchange ratio, oxygen pulse, ventilatory efficiency.
In a healthy sedentary adult, these numbers form a predictable pattern. In a deconditioned person, the numbers are low but the pattern is preserved. In ME/CFS, the pattern itself breaks on Day 2 — and that is the whole point of running the test twice.
Why Two Days — The Day-2 Drop
A single CPET on a person with ME/CFS often looks unremarkable. Our bodies can produce one maximal effort. Muscles contract, heart rate climbs, lungs move air, and the numbers fall within the wide range that could pass as "deconditioning" on a cardiologist's report. That is exactly why a single-day CPET is not enough — and exactly why disability insurers who know what they are doing will dismiss it.
The magic of the 2-day protocol, pioneered by the Workwell Foundation (Staci Stevens, Christopher Snell, Mark VanNess) in the early 2000s, is that it forces the body to do what daily life forces it to do: perform again the next day. You come back approximately 24 hours later and do the entire test over. A healthy person — even a profoundly deconditioned healthy person, even a patient with heart failure, even a patient with chronic obstructive pulmonary disease — reproduces their Day-1 numbers within roughly 7%. The body recovers its capacity overnight. That is what healthy aerobic systems do.
People with ME/CFS do not. On Day 2, VO2 at anaerobic threshold and workload at anaerobic threshold drop measurably, sometimes dramatically. This is not fatigue. It is not lack of effort (respiratory exchange ratio confirms maximal effort on both days). It is an objective, reproducible failure of aerobic energy production to recover after a modest exercise challenge. That failure is post-exertional malaise, caught in the act and quantified to two decimal places.
The Day-2 Numbers That Count
The published studies converge on a few key findings:
- In healthy controls, Day-2 VO2 at anaerobic threshold reproduces Day 1 within roughly plus or minus 7%.
- In ME/CFS patients, Day-2 VO2 at AT drops by an average of 10% to 25%, with many patients dropping more.
- Workload at AT (the watts you can sustain without going anaerobic) drops similarly, often by 20% to 55%.
- The drop is reproducible across studies (Snell 2013, Keller 2014, VanNess 2007, Stevens 2018) and across testing centers.
- A Day-2 drop of more than 10% in VO2 at AT is considered outside the range of deconditioning, cardiac disease, or pulmonary disease and is consistent with ME/CFS pathophysiology.
Translated into daily life: if your workload at anaerobic threshold falls from 75 watts on Day 1 to 45 watts on Day 2, you have just documented that after one ordinary-looking exertion you lost 40% of your sustainable capacity overnight. That is the physiological reason you can shower on Monday, attempt to cook dinner on Tuesday, and spend Wednesday flattened. The test is catching what your life already knows.
The Trade-Off — This Test Can Crash You
Here is the part most articles gloss over. The 2-day CPET is, by design, a PEM provocation. You are being asked to push to volitional exhaustion twice inside 24 hours, specifically so that the crash shows up on the instruments. That crash does not politely end when you step off the bike.
Patients commonly report:
- A "normal" ME/CFS crash in the days immediately after — cognitive fog, flu-like symptoms, sore throat, swollen lymph nodes, muscle pain, orthostatic worsening, sleep disturbance.
- Extended recovery of weeks to months before returning to their pre-test baseline.
- In some cases, a permanent step-down in baseline function — they never fully return to where they were before the test.
Workwell and other experienced centers are direct about this with patients before booking. It is not a complication; it is the mechanism. You cannot document PEM without triggering PEM. The only question is whether your particular body, at this particular stage of illness, can tolerate the provocation in exchange for the data.
For someone mildly affected who is fighting for disability benefits, returning to work conversations, or trying to get a skeptical specialist to take them seriously, the trade may be worth it. For someone moderately affected who is just barely holding their life together, the risk of a permanent worsening is real and needs to be weighed honestly. For severe and very severe patients, this test is contraindicated outright — see the severe and very severe ME article.
Who Is Appropriate (and Who Is Not)
The informal rule used by Workwell and similar centers: if you cannot reliably walk into the clinic, change clothes, pedal a bike to exhaustion, and do it again 24 hours later without requiring hospitalization or months of recovery, you are not a candidate.
Generally appropriate:
- Mild ME/CFS — ambulatory, can work part-time or manage household tasks with pacing.
- Moderate ME/CFS — mostly housebound but can do a few hours of light activity per day.
- Patients pursuing Social Security Disability, long-term disability insurance claims, or workplace accommodations where objective documentation is pivotal.
- Patients whose clinicians will not accept the diagnosis without "hard" evidence.
Generally not appropriate:
- Severe or very severe ME/CFS — mostly or fully bedbound, require help with basic daily activities.
- Patients in an active crash or flare.
- Patients with unstable cardiac disease, uncontrolled hypertension, or other standard cardiology contraindications to maximal exercise testing.
- Patients whose disability claim is already progressing on other documentation and for whom the test adds marginal benefit relative to the risk.
No reputable center will run this test on a patient they consider too sick. If you are being offered a 2-day CPET and you think you are too sick for it, trust yourself — decline or defer.
Where to Get a 2-Day CPET
The list of centers with experience running the ME/CFS 2-day protocol is short. The ones patients most commonly use:
- Workwell Foundation (Ripon, California) — the originators of the protocol; decades of ME/CFS-specific experience; produce disability-oriented reports written in the language insurers and administrative judges read. Appointments typically booked months out.
- Bateman Horne Center (Salt Lake City, Utah) — a specialty ME/CFS and fibromyalgia clinic that runs 2-day CPETs as part of broader diagnostic workups. Useful if you want clinical evaluation alongside the test.
- Ithaca College Exercise and Sports Sciences program (Ithaca, New York) — runs 2-day CPETs with ME/CFS-experienced exercise physiologists on the East Coast.
- Mount Sinai (New York, New York) — the post-acute sequelae clinic runs 2-day CPETs as part of its evaluation pathway. Appropriate for patients with ME/CFS from a range of post-viral triggers; not the right route for readers looking for a pandemic-related pathway, which is outside the scope of this site.
A handful of academic cardiology labs will also run a 2-day CPET if a referring physician writes a specific protocol request, but reports from non-specialist labs frequently misinterpret the Day-2 drop or fail to report anaerobic-threshold numbers at all. If the report does not explicitly state VO2 at AT and workload at AT for both days, side by side, it is not a useful ME/CFS CPET.
Cost, Insurance, and Paying Out of Pocket
Expect to pay between $3,000 and $5,000 out of pocket for the 2-day test, depending on the center and whether a clinical interpretation is bundled. Additional costs typically include travel, lodging for 3 to 5 nights (arrival day, two testing days, at least one recovery day before attempting the trip home), and someone to accompany you.
Insurance coverage is the exception, not the rule:
- Most insurers consider the second day of testing "investigational" for ME/CFS and deny it.
- Day 1 is sometimes reimbursable under standard CPET CPT codes (93018, 94621), especially when ordered by a cardiologist to rule out cardiac disease.
- Some patients successfully submit appeals after the fact, particularly when the test results are pivotal to an approved disability claim.
- Health savings account (HSA) and flexible spending account (FSA) dollars generally cover the test.
Plan financially for the full cost up front. Treat any insurance reimbursement as a bonus.
Preparing for the Test
Preparation starts weeks before. The goal is to arrive as close to your personal baseline as possible so the Day-1 numbers reflect your actual capacity rather than a flare.
- Pace rigorously for two to four weeks beforehand. This is the opposite of "training" — you want to arrive rested, not conditioned. See the pacing and energy-envelope article for the underlying framework.
- Medication adjustments per your center's protocol. Beta-blockers, stimulants, and some autonomic medications alter heart-rate and ventilatory responses and may need to be held for 24 to 48 hours. Do not stop any medication without written instructions from the testing center and clearance from your prescribing physician.
- Travel a day early and rest. Do not fly and test in the same 24-hour window.
- Bring someone with you. You will not be capable of navigating an airport or driving safely after Day 2, and possibly not after Day 1. A spouse, parent, adult child, or paid caregiver who can handle logistics is essential.
- Hydration and electrolytes. Many ME/CFS patients also have orthostatic intolerance (see the orthostatic intolerance article). Arriving dehydrated will worsen both the test experience and the recovery.
- Book recovery time. Do not schedule anything important in the weeks after the test. Assume you will be flat.
- Sleep plans on the road. Reserve a quiet hotel room, blackout curtains, and a flexible check-out time in case you cannot leave on schedule.
Using the Results for Disability Claims
The reason most patients pay for a 2-day CPET is to build a disability file. The report, properly written, is one of the most powerful single documents in ME/CFS adjudication for two reasons: it is objective (machine-measured), and it speaks a language insurance medical directors already understand (they use single-day CPETs routinely for cardiac and pulmonary claims).
A useful report translates the numbers into functional capacity. Instead of stopping at "VO2 at AT dropped 22%," it says: "The patient's sustainable workload on Day 2 corresponds to a metabolic equivalent (MET) level of 2.5, which is below the threshold for sustained sedentary desk work and consistent with a disability determination of unable to perform any substantial gainful activity on a reproducible daily basis."
The test is used successfully in:
- Social Security Disability Insurance (SSDI) and Supplemental Security Income (SSI) claims, where administrative law judges increasingly recognize the 2-day CPET as addressing the "reproducibility" standard for sustained work.
- Private long-term disability (LTD) claims under employer-sponsored policies, where insurers often demand functional capacity evidence beyond physician opinion.
- Individual disability insurance policies, which tend to have even stricter documentation requirements.
- Workplace accommodation requests under the Americans with Disabilities Act (ADA).
Workwell and Bateman Horne produce reports written specifically for this purpose. If you go through a non-specialist cardiology lab, you may get raw data without the functional-capacity narrative, which forces your attorney or physician to do the translation work — sometimes badly. Budget accordingly.
Alternatives If You Are Too Sick for CPET
If the 2-day CPET is too risky for you — or you cannot afford it, or you cannot travel — there are gentler objective tests that contribute meaningful evidence. None individually carries the weight of a 2-day CPET, but a combination builds a credible file.
- NASA Lean Test (10-minute passive stand test). Free, requires no equipment beyond a blood pressure cuff, can be done at home with a partner. Documents orthostatic intolerance by measuring heart rate and blood pressure at baseline (supine) and every minute for 10 minutes of quiet standing. A sustained heart-rate rise of 30 beats per minute or more (40 bpm in adolescents), or a systolic blood pressure drop of 20 mmHg or more, is abnormal. See the POTS deep-dive article on tilt-table and NASA Lean testing for the protocol.
- Tilt-table test. The formal, hospital-based version of the NASA Lean Test. Recognized by cardiology and neurology, often covered by insurance. Useful when POTS or orthostatic hypotension is prominent. See the POTS overview.
- 24-hour ambulatory heart-rate and blood-pressure monitoring. Documents the day-to-day reality of orthostatic dysfunction in ways a single clinic measurement cannot.
- Heart rate variability (HRV) monitoring. Consumer wearables (Oura, Garmin, Polar H10 chest strap with apps such as HRV4Training, Welltory, or Elite HRV) track overnight HRV and morning readiness. Trends showing persistently low HRV and suppressed readiness on days following even minor activity are consistent with autonomic dysfunction. Not diagnostic on their own, but useful as pattern evidence.
- Functional Capacity Evaluation (FCE). A full-day standardized evaluation run by an occupational or physical therapist who measures lifting, carrying, sitting tolerance, standing tolerance, and repetitive tasks. Widely used in disability determinations. Be cautious — many FCE examiners do not understand PEM and will score you on your "good" effort without noting the crash that follows. Insist on a two-day FCE when possible, and request that PEM be explicitly documented.
- Actigraphy. Wrist-worn accelerometers log activity continuously for one to four weeks, producing a paper trail of how much — or how little — you actually move. Inexpensive, non-provoking, and hard to argue with.
- Symptom diaries with wearable data. Not flashy, but contemporaneous daily logs of step counts, heart rate, and symptoms carry real weight when paired with any of the above.
Autonomic Panels, NK Cells, and Other Objective Markers
Beyond exercise-based testing, a few laboratory and physiologic measures are consistently abnormal in ME/CFS and can round out an objective workup:
- Natural killer (NK) cell function. Low NK cell cytotoxicity is one of the most reproducible laboratory abnormalities in ME/CFS across studies and decades. The test (often labeled "NK cell function" or "K-cell activity") measures how effectively your NK cells kill target cells in vitro — not simply how many you have. Low function suggests a persistent immune dysregulation consistent with the post-viral pathophysiology of the illness. Available through specialty labs (e.g., ARUP, Quest research menu); not always covered by insurance.
- Autonomic function panels. Sudomotor testing (QSART), deep-breathing heart-rate variability, Valsalva ratio, and tilt-table together form a formal autonomic battery available at academic neurology autonomic labs (Mayo, Vanderbilt, Cleveland Clinic, others). Abnormal findings document the small-fiber and autonomic component of the illness.
- Skin biopsy for small-fiber neuropathy. A 3 mm punch biopsy of the lower leg, stained for intraepidermal nerve fiber density, can document small-fiber neuropathy, which is common in ME/CFS and overlapping conditions such as fibromyalgia.
- Cognitive testing. Formal neuropsychological batteries — ideally repeated before and after a provocation such as exercise or cognitive load — can document the cognitive component of PEM.
- Basic immune and inflammatory labs. While CBC and CMP are typically normal, some patients show low morning cortisol, reactivated herpes-family viruses (EBV, HHV-6), low IgG subclasses, or elevated cytokines. See post-viral triggers for context.
None of these replaces the 2-day CPET as evidence of PEM, but in combination they build a convergent picture. For disability purposes in particular, a file showing abnormal NK function, abnormal autonomic testing, abnormal NASA Lean Test, and an actigraphy record of profoundly limited activity can approach the weight of a CPET without the crash risk.
Making the Decision
A practical way to think about whether the 2-day CPET is right for you:
- Are you in the mild-to-moderate range, and does your physical situation allow two days of maximal effort plus weeks of recovery?
- Is there a specific, high-stakes use for the report — pending SSDI hearing, LTD appeal, contested diagnosis with a specialist?
- Have you exhausted gentler objective evidence (NASA Lean Test, tilt-table, NK function, actigraphy) and found the file still insufficient?
- Can you arrange travel, companionship, and recovery time without destabilizing the rest of your life?
- Are you emotionally prepared for the possibility of a prolonged crash, including the possibility that your baseline does not fully return?
If the answer to most of these is yes, the 2-day CPET is one of the most powerful tools available in this illness. If the answer to several is no, start with the alternatives and build your objective file piece by piece. A disability claim almost never rises or falls on a single test. The goal is a coherent, reproducible, machine-measured record of an illness that standard medicine was not built to see — and there is more than one road to that record.
Key Research Papers
- VanNess JM, Snell CR, Stevens SR. Diminished cardiopulmonary capacity during post-exertional malaise. J Women's Health. 2007.
- Snell CR, Stevens SR, Davenport TE, VanNess JM. Discriminative validity of metabolic and workload measurements for identifying people with chronic fatigue syndrome. Phys Ther. 2013.
- Keller BA, Pryor JL, Giloteaux L. Inability of myalgic encephalomyelitis/chronic fatigue syndrome patients to reproduce VO2 peak indicates functional impairment. J Transl Med. 2014.
- Stevens S, Snell C, Stevens J, Keller B, VanNess JM. Cardiopulmonary exercise test methodology for assessing exertion intolerance in myalgic encephalomyelitis/chronic fatigue syndrome. Front Pediatr. 2018.
Live PubMed Searches
For further reading, these PubMed topic searches return current peer-reviewed work on exercise testing, autonomic evaluation, and objective biomarkers in ME/CFS:
- Two-day CPET in chronic fatigue syndrome
- Post-exertional malaise and cardiopulmonary exercise testing
- Anaerobic threshold in myalgic encephalomyelitis
- Natural killer cell function in chronic fatigue syndrome
- Tilt-table testing and orthostatic intolerance in ME/CFS
- NASA Lean Test and orthostatic evaluation
- Functional capacity evaluation in chronic fatigue syndrome
- Small-fiber neuropathy and chronic fatigue syndrome
Connections
- ME/CFS Overview
- Post-Viral Triggers: EBV and Others
- Severe and Very Severe ME
- Orthostatic Intolerance in ME/CFS
- Post-Exertional Malaise
- Pacing and the Energy Envelope
- ME/CFS Diagnostic Criteria
- LDN, Abilify and Experimental Therapies
- Mitochondrial Dysfunction and Energy Metabolism
- POTS
- Tilt-Table and NASA Lean Test
- Fibromyalgia
- MCAS
- Chronic Pain
- Fatigue
- Complete Blood Count
- Inflammatory Markers